2873
3D broadband IR-prepared UTE bone Imaging for assessment of ossification of the posterior longitudinal ligament (OPLL) in the cervical spine1Philips Japan, Tokyo, Japan, 2Philips Australia & New Zealand, North Ryde, Australia, 3University of Miyazaki, Miyazaki, Japan, 4Philips Healthcare, Tokyo, Japan
Synopsis
We proposed a new technique for the cervical spine MR bone imaging based on broadband inversion recovery prepared segmented multispoke UTE sequence (3D BoneVIEW) for assessment of ossification of the posterior longitudinal ligament (OPLL). 3D BoneVIEW provided robust spinal bone imaging with sufficient background suppression. This sequence might be useful for
Purpose
Ossification of the posterior longitudinal ligament (OPLL) is a multifactorial condition caused by ectopic hyperostosis and calcification of the posterior longitudinal ligament1. To diagnose OPLL, both magnetic resonance imaging (MRI) and computed tomography (CT) examinations are critical2. MRI better delineates the extent of soft tissue abnormalities, whereas CT more readily identifies the foci of frank ossification2. CT analysis must be performed to differentiate spondylotic myelopathy, which is essential when considering operative intervention3.
Recently, MR bone imaging, using ultrashort echo-time (UTE) or zero echo-time (ZTE) sequence, has gained more attention for detection and assessment of bone pathology as an alternative to computed tomography (CT) bone imaging4-8. Challenge of MR bone imaging for clinical application in the cervical spine is to increase the robustness of image quality. Bone weighted imaging based on simultaneous long- and short T2 suppression inversion-recovery (IR) technique9,10 may suffer from insufficient fat and long-T2 suppression due to B0 inhomogeneities caused by the complex anatomical structure of the cervical area.
To overcome this problem, we proposed a new technique based on broadband IR prepared segmented (multispoke) UTE sequence (3D BoneVIEW). The purpose of this study was to evaluate the feasibility of 3D BoneVIEW technique in the cervical spine for assessment of OPLL.
Methods
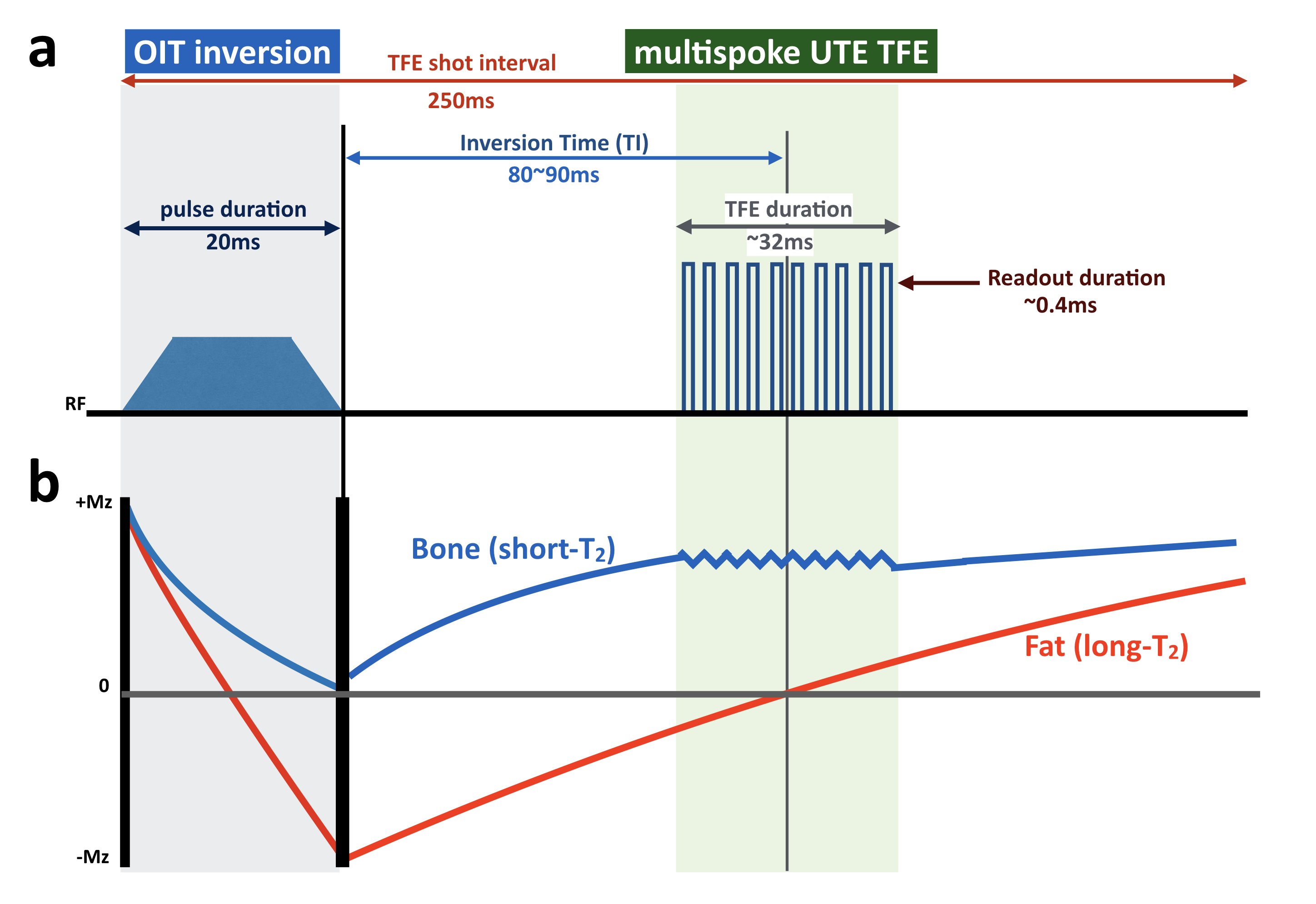
3D BoneVIEW is based on inversion recovery prepared segmented multispoke UTE 3D stack-of-stars radial sequence9 (IR-prepared turbo field echo, IR-TFE) [Fig.1a]. Adiabatic inversion pulses selectively invert long-T2 species and fat simultaneously10. For robustness against B1 and B0 sensitivity, we applied a broadband offset independent trapezoid (OIT) pulse, which has already been used for brachial plexus MR neurography11,12. To suppress the background signals sufficiently, we used a long duration OIT inversion pulse (≥20ms). By using such a longer pulse duration, long T2 species are inverted whereas short T2 species are saturated9 because the T2 relaxation time of bone is significantly shorter than the duration of the RF pulse. The TFE shot interval (otherwise repetition time, TR) and inversion delay (TI) are chosen such that optimal nulling of the signal from both muscle and fat13 is achieved [Fig.1b]. This provides high contrast morphological imaging of bone.
To prevent the blurring of the bone due to T2* decay during the readout period, the literature14 suggests that readout duration should be less than 0.81xT2*. Since the T2 value of cortical bone is on the order 400us15, we kept the actual readout duration within 400us. For the TFE (multispoke) excitation, a shot duration of 250ms was applied because the T1 relaxation time of bone is around 250ms. In addition, we set the constant shot length (actual TRxTFE factor) around 32ms to prevent the recovery of fat signals during TFE shot.
A total of seven volunteers and two patients with OPLL were examined with a 3.0T whole-body clinical system (Ingenia CX, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects.
Imaging parameters for BoneVIEW were; 3D stack-of-stars radial UTE-TFE, Sagittal or Coronal acquisition, voxel size=1.4*1.4*2.5mm, FOV=400*400mm, TFE shot interval=250ms, flip angle=16°, turbo factor=11, TR/TE=2.6/0.09ms, TI=84ms, and total acquisition time=7 to 10minutes (depend on the body habitus).
Results and Discussion
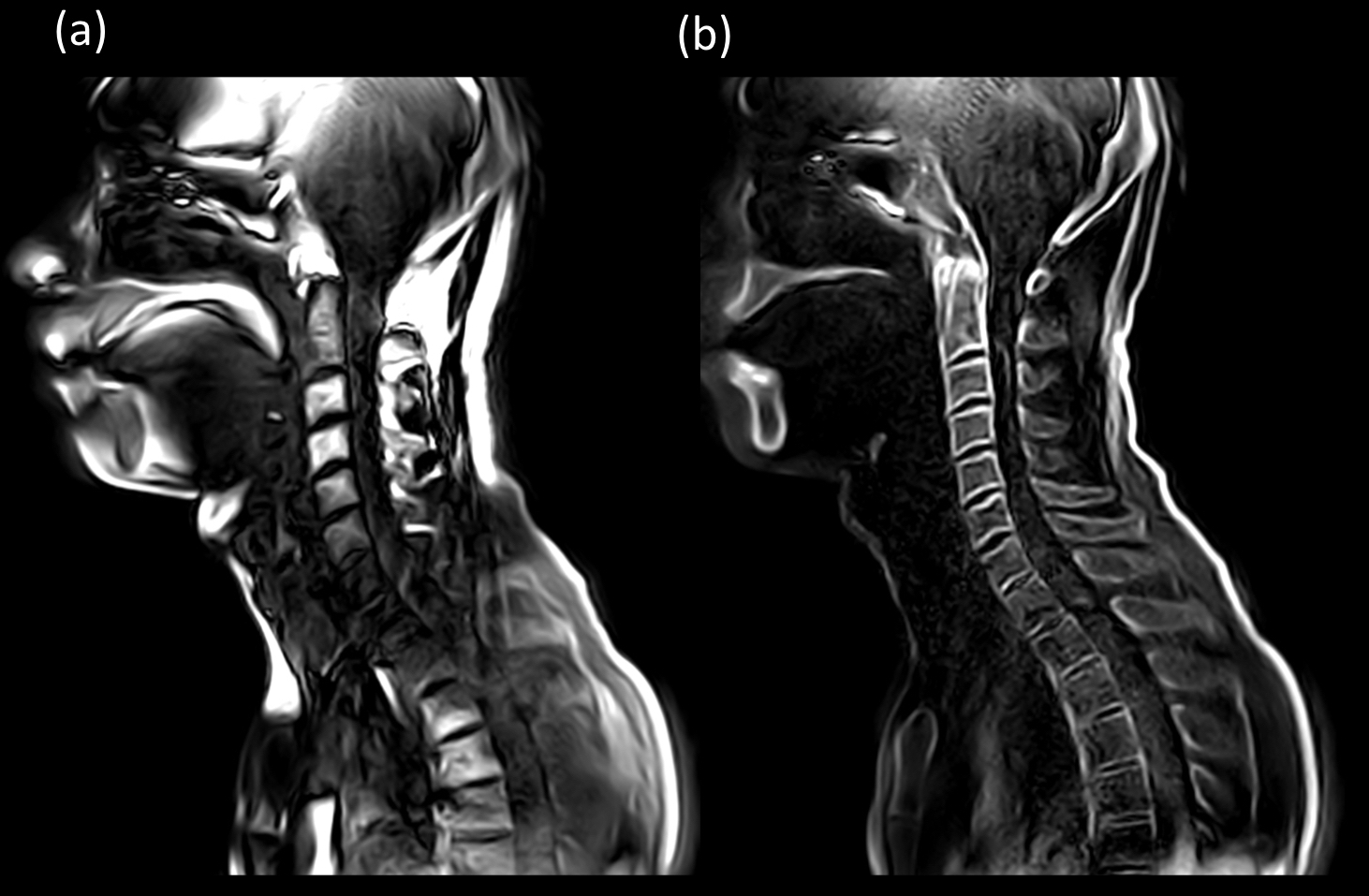
Figure 2 demonstrates the effect of broadband inversion pulse. The OIT pulse was more robust to B1 and B0 inhomogeneities compare to conventional adiabatic pulse in the complex anatomical structure of the cervical area.
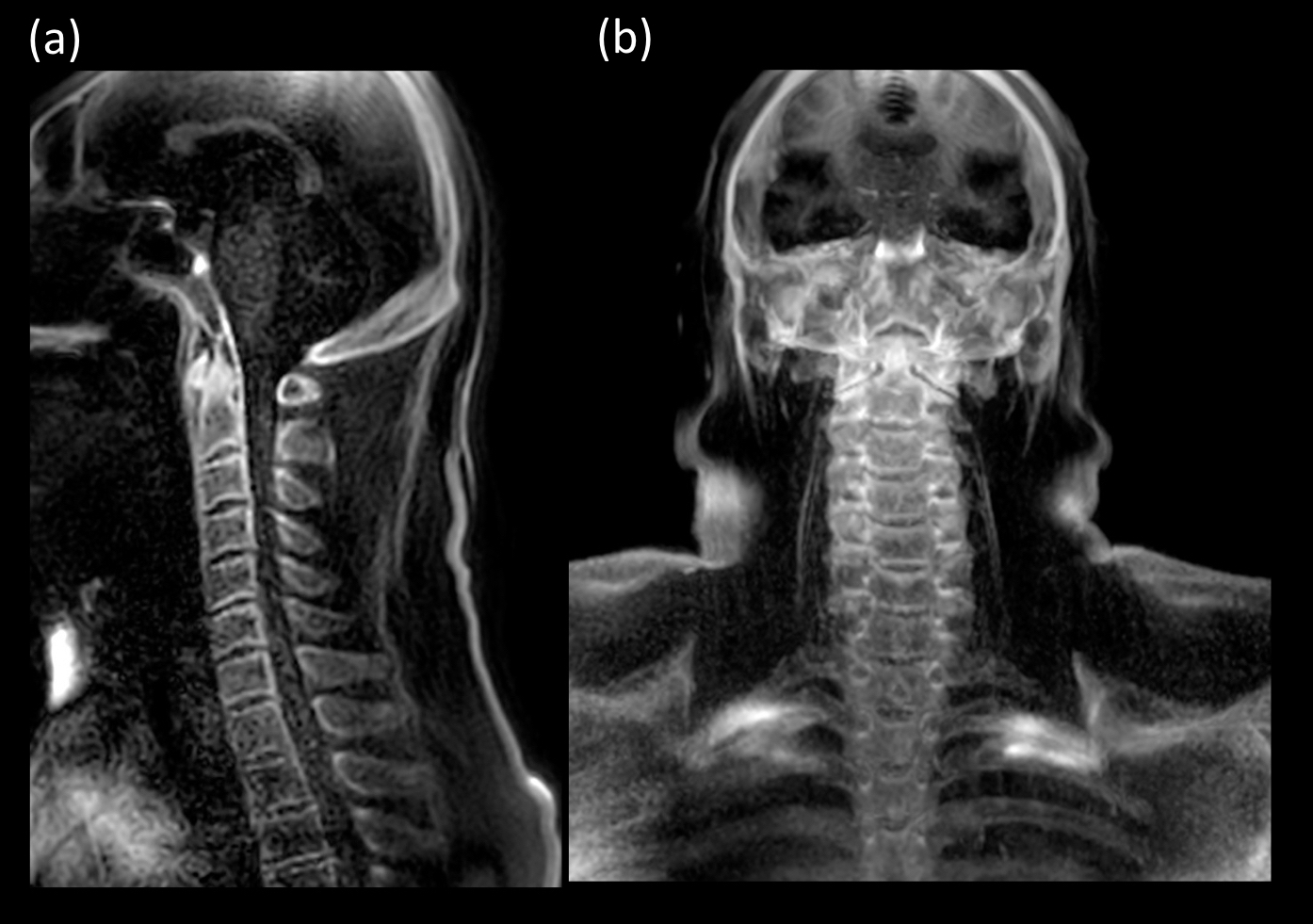
Representative coronal and sagittal BoneVIEW images with partial MIP are shown in Figure 3. BoneVIEW clearly depicted the cortical bone structure of the cervical spine while suppressing background signals sufficiently.
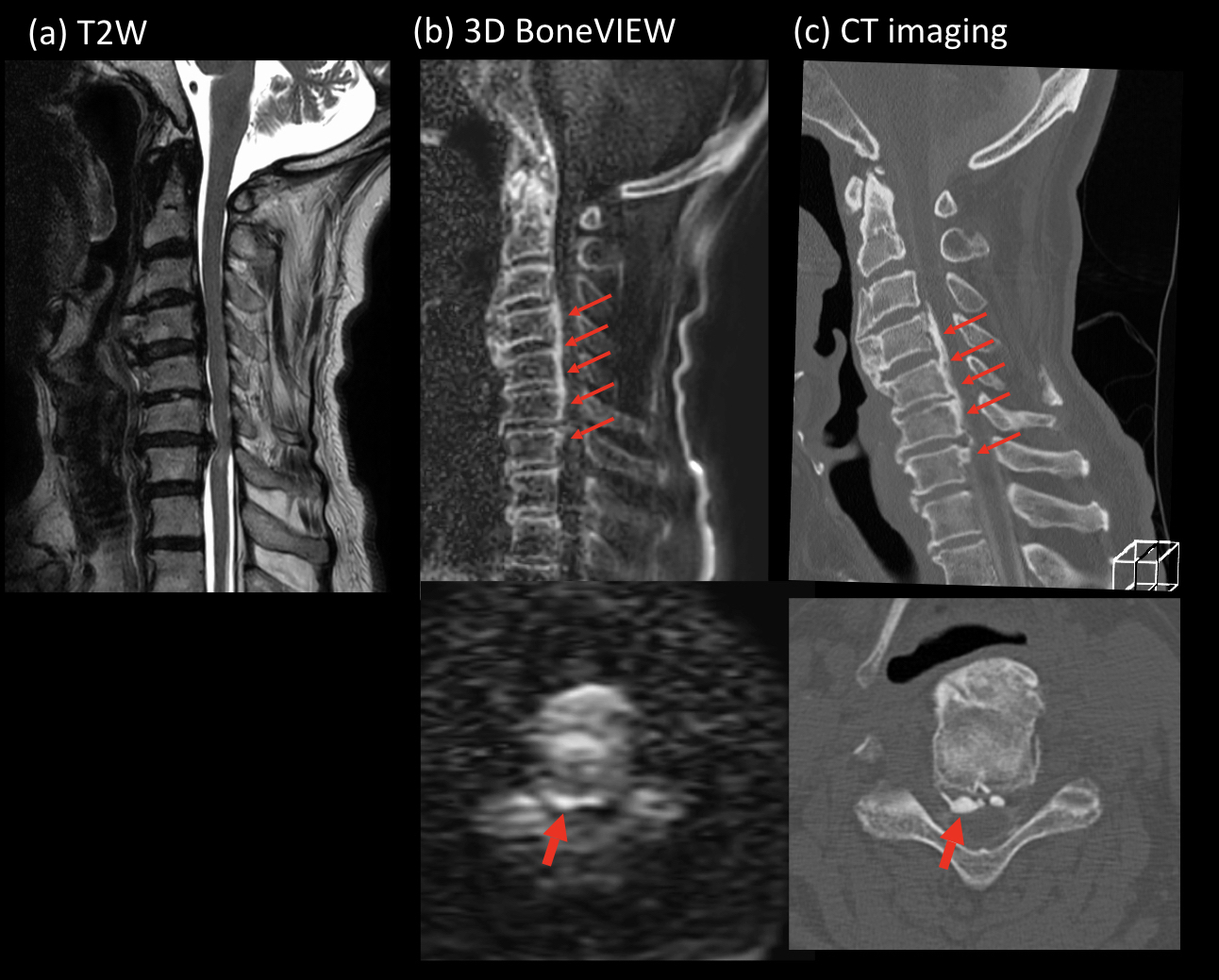
Figure 4 shows representative clinical case in a patient with OPLL comparison with CT scan. BoneVIEW clearly showed the existence of ectopic hyperostosis as well as CT scan. Although further clinical investigation is needed, this technique can provide comparable information with CT imaging.
Conclusion
We have demonstrated the feasibility of a new scheme for MR bone imaging for the cervical spine by using broadband IR-prepared segmented multispoke UTE sequence. This sequence might be useful for assessment of the OPLL as an alternative to CT bone imaging.Acknowledgements
No acknowledgement found.References
1. Abiola R, et al. Ossification of the Posterior Longitudinal Ligament: Etiology, Diagnosis, and Outcomes of Nonoperative and Operative Management. Global Spine J. 2016;6:195–204.
2. Epstein N. Diagnosis and surgical management of cervical ossification of the posterior longitudinal ligament. Spine J. 2002;2:436-49.
3. Kadoya S, et al. Neuroradiology of ossification of the posterior longitudinal spinal ligament. Comparative studies with the tomography. Neuroradiology. 1978;16:357-8.
4. Delso G, et al. Clinical evaluation of zero-echo-time MR imaging for the segmentation of the skull. J Nucl Med. 2015;56:417-22.
5. Wiesinger F, et al. Zero TE MR bone imaging in the head. Magn Reson Med. 2016;75:107-14.
6. Nazaran A, et al. Three-dimensional adiabatic inversion recovery prepared ultrashort echo time cones (3D IR-UTE-Cones) imaging of cortical bone in the hip. Magn Reson Imaging. 2017;44:60-64.
7. Wiesinger F, et al. Zero TE-based pseudo-CT image conversion in the head and its application in PET/MR attenuation correction and MR-guided radiation therapy planning. Magn Reson Med. 2018;80:1440-1451.
8. Gersing AS, et al. Evaluation of MR-derived CT-like images and simulated radiographs compared to conventional radiography in patients with benign and malignant bone tumors. Eur Radiol. 2018 Jun 12. doi: 10.1007/s00330-018-5450-y.
9. Carl M, et al. UTE imaging with simultaneous water and fat signal suppression using a time-efficient multispoke inversion recovery pulse sequence. Magn Reson Med. 2016;76:577-82.
10. Larson PE, et al. Using adiabatic inversion pulses for long-T2 suppression in ultrashort echo time (UTE) imaging. Magn Reson Med. 2007;58:952-61.
11. Yoneyama M, et al. Motion-Sensitized Driven-Inversion (MSDI) for improvement of diffusion-prepared MR neurography (SHINKEI) in the brachial plexus. Proc Intl Soc Mag Reson Med. 2017;25:0854.
12. Yoneyama M, et al. Quantitative MR Neurography with Robust Fat Suppression. Proc Intl Soc Mag Reson Med. 2018;26:5400.
13. Li S, et al. Effects of inversion time on inversion recovery prepared ultrashort echo time (IR-UTE) imaging of bound and pore water in cortical bone. NMR Biomed. 2015;28:70-8.
14. Gai ND, et al. Optimized Ultra-short Echo Time Breathhold 3D Lung Imaging. Proc. Intl. Soc. Mag. Reson. Med. 2015;23:3977.15. Carl M, et al. Radiofrequency pulses for simultaneous short T2 excitation and long T2 suppression. Magn Reson Med. 2011;65:531-7.
Figures