2871
A predictive model for postlaminar optic nerve invasion in retinoblastoma basedon radiomic features from MR images1Department of Radiology, Beijing Tongren Hospital, Capital Medical University, Beijing, Beijing, China
Synopsis
Retinoblastomas (RB) with postlaminar optic nerve invasion (PLONI) increases the risk for systemic metastasis or local recurrence. MRI is the only method to detect the PLONI in patients with eye-saving treatment strategies. But accuracy of MRI in identifying PLONI was relatively limited. Radiomics is an emerging field with a number of different uses being proposed. We hypothesized that radiomics can have an additional contribution to predicting PLONI in patients with retinoblastoma. This study validated our hypothesis.
INTRODUCTION
Retinoblastomas (RB) with postlaminar optic nerve invasion (PLONI) increases the risk for systemic metastasis or local recurrence1-5. Although histopathologic examination is the gold standard for finding the postlaminar optic nerve invasion, MRI is the only method to detect the PLONI in patients with eye-saving treatment strategies6, 7. To date, several studies have investigated the relationships between MR imaging features with PLONI6 8-19. These studies reported that the accuracy of MRI in identifying PLONI was relatively limited (52%–79%)11, 19, 20. Radiomics uses the high-throughput extraction of advanced quantitative features to objectively and quantitatively describe tumor phenotypes. These quantitative features, which may fail to be appreciated by the naked eye, can potentially provide valuable diagnostic, prognostic or predictive information in oncology. 21 Recent studies22, 23 have shown that many radiomic features were able to significantly differentiate between early and advanced stage diseases. The aim of the study was to investigate whether MR images-based radiomics signature could predict PLONI for RB patients.METHODS
One hundred twenty-four patients with pathology-proven RB (54 patients with PLONI, 70 patients without PLONI) were divided into training and validation cohorts. A total of 2058 quantitative imaging features were extracted from T2-WI and contrast-enhanced T1-WI (CET1-WI). To reduce dimensionality of features, we used variance threshold, select K best and least absolute shrinkage and selection operator (LASSO) algorithm methods to gradually select the optimal features. We use support vector machine (SVM) to build a predictive model for predicting PLONI for RB patients. Discriminating performance was assessed by the area under the receiver operating characteristic curve (AUC).RESULTS
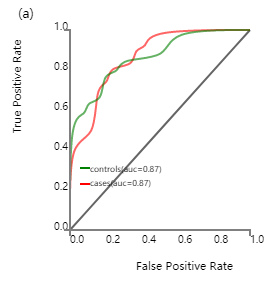
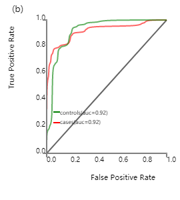
we selected 13 optimal features from CET1-WI, 4 optimal features from T2-WI and 15 optimal features (Table.1) from joint CET1-WI and T2-WI. When training with SVM classifier, the area under the curve (Fig.1), sensitivity, and specificity for predicting PLONI based on CET1-WI and T2-WI were 0.919, 0.79, and 0.93 in the primary cohort, respectively, while they were 0.870, 0.73, and 0.79 in the validation cohort, respectively. The signature based on CET1-WI predicted PLONI with an AUC of 0.889 and 0.799 in the primary and validation cohorts respectively. The signature based on T2-WI predicted PLONI with an AUC of 0.881 and 0.831 in the primary and validation cohorts respectively. A radiomics model derived from joint CET1-WI and T2-WI showed better prognostic performance than models derived from CET1-WI or T2-WI alone.DISCUSSION
Predicting PLONI for RB patients based on preoperative MRI is challenging (especially early-stage PLONI)12. In the current study, we identified MRI-based radiomics as a new approach for predicting PLONI before enucleation in RB patients. To our knowledge, this is the first study of MRI-based radiomics for predicting PLONI in RB patients. We built a predictive model for PLONI in retinoblastoma based on radiomic features from MR images, which was effective in predicting PLONI in RB patients. And the model can provide quantitative image features such as texture analysis as an objective and quantitative way to assess PLONI. Especially the radiomics signature derived from T2-WI alone shows a relatively good diagnostic accuracy in the prediction of PLONI, which is meaningful for those patients with contraindications to contrast media. The limitations of this study were that the study was retrospective in nature and did not cover clinical information such as the stage by the International Retinoblastoma Staging.CONCLUSION
MRI-based radiomics provided a reasonably good diagnostic accuracy in the prediction of PLONI for RB patients. These results provide an illustrative example of precision medicine and may select the best treatment for individual patients.Acknowledgements
No acknowledgement found.References
1. Khelfaoui F, Validire P, Auperin A, et al. Histopathologic risk factors in retinoblastoma: a retrospective study of 172 patients treated in a single institution. Cancer-Am Cancer Soc. 1996;77(6):1206-1213.
2. Kopelman JE, Mclean IW, Rosenberg SH. Multivariate analysis of risk factors for metastasis in retinoblastoma treated by enucleation. Ophthalmology. 1987;94(4):371-377.
3. Shields CL, Shields JA, Baez K, Cater JR, De Potter P. Optic nerve invasion of retinoblastoma. Metastatic potential and clinical risk factors. Cancer-Am Cancer Soc. 1994;73(3):692-698.
4. Messmer EP, Heinrich T, Höpping W, De SE, Havers W, Sauerwein W. Risk factors for metastases in patients with retinoblastoma. Ophthalmology. 1991;98(2):136-141.
5. Kaliki S, Shields CL, Rojanaporn D, et al. High-Risk Retinoblastoma Based on International Classification of Retinoblastoma: Analysis of 519 Enucleated Eyes. Ophthalmology. 2013;120(5):997-1003.
6. Galluzzi P, Cerase A, Hadjistilianou T, et al. Retinoblastoma: Abnormal gadolinium enhancement of anterior segment of eyes at MR imaging with clinical and histopathologic correlation. Radiology. 2003;228(3):683-690.
7. Rauschecker AM, Patel CV, Yeom KW, et al. High-Resolution MR Imaging of the Orbit in Patients with Retinoblastoma. Radiographics. 2012;32(5):1307-1326.
8. Lee BJ, Kim JH, Kim DH, Park S, Yu YS. The validity of routine brain MRI in detecting post-laminar optic nerve involvement in retinoblastoma. Brit J Ophthalmol. 2012;96(9):1237-1241.
9. Lemke AJ, Kazi I, Mergner U, et al. Retinoblastoma - MR appearance using a surface coil in comparison with histopathological results. Eur Radiol. 2007;17(1):49-60.
10. Hiasat JG, Saleh A, Al-Hussaini M, et al. The predictive value of magnetic resonance imaging of retinoblastoma for the likelihood of high-risk pathologic features. Eur J Ophthalmol. 2018:1369776408.
11. Song KD, Eo H, Kim JH, Yoo S, Jeon TY. Can preoperative MR imaging predict optic nerve invasion of retinoblastoma? Eur J Radiol. 2012;81(12):4041-4045.
12. Brisse HJ, de Graaf P, Galluzzi P, et al. Assessment of early-stage optic nerve invasion in retinoblastoma using high-resolution 1.5 Tesla MRI with surface coils: a multicentre, prospective accuracy study with histopathological correlation. Eur Radiol. 2015;25(5):1443-1452.
13. Sirin S, Schlamann M, Metz KA, et al. High-resolution MRI using orbit surface coils for the evaluation of metastatic risk factors in 143 children with retinoblastoma. Neuroradiology. 2015;57(8):815-824.
14. Chawla B, Sharma S, Sen S, et al. Correlation between Clinical Features, Magnetic Resonance Imaging, and Histopathologic Findings in Retinoblastoma: A Prospective Study. Ophthalmology. 2012;119(4):850-856.
15. de Jong MC, de Graaf P, Noij DP, et al. Diagnostic Performance of Magnetic Resonance Imaging and Computed Tomography for Advanced Retinoblastoma. Ophthalmology. 2014;121(5):1109-1118.
16. Wilson MW, Rodriguez-Galindo C, Billups C, Haik BG, Laningham F, Patay Z. Lack of Correlation between the Histologic and Magnetic Resonance Imaging Results of Optic Nerve Involvement in Eyes Primarily Enucleated for Retinoblastoma. Ophthalmology. 2009;116(8):1558-1563.
17. Brisse HJ, Guesmi M, Aerts I, et al. Relevance of CT and MRI in retinoblastoma for the diagnosis of postlaminar invasion with normal-size optic nerve: a retrospective study of 150 patients with histological comparison. Pediatr Radiol. 2007;37(7):649-656.
18. De Jong MC, van der Meer FJ, Goricke SL, et al. Diagnostic Accuracy of Intraocular Tumor Size Measured with MR Imaging in the Prediction of Postlaminar Optic Nerve Invasion and Massive Choroidal Invasion of Retinoblastoma. Radiology. 2016;279(3):817-826.
19. de Graaf P, Barkhof F, Moll AC, et al. Retinoblastoma: MR imaging parameters in detection of tumor extent. Radiology. 2005;235(1):197-207.
20. Schueler AO, Hosten N, Bechrakis NE, et al. High resolution magnetic resonance imaging of retinoblastoma. Br J Ophthalmol. 2003;87(3):330-335.
21. Yip SS, Aerts HJ. Applications and limitations of radiomics. Phys Med Biol. 2016;61(13):R150-R166.
22. Mu W, Chen Z, Liang Y, et al. Staging of cervical cancer based on tumor heterogeneity characterized by texture features on F-18-FDG PET images. Physics in Medicine & Biology. 2015;60(13):5123-5139.
23. Dong X, Xing L, Wu P, et al. Three-dimensional positron emission tomography image texture analysis of esophageal squamous cell carcinoma: relationship between tumor 18F-fluorodeoxyglucose uptake heterogeneity, maximum standardized uptake value, and tumor stage. Nucl Med Commun. 2013;34(1):40-46.
Figures
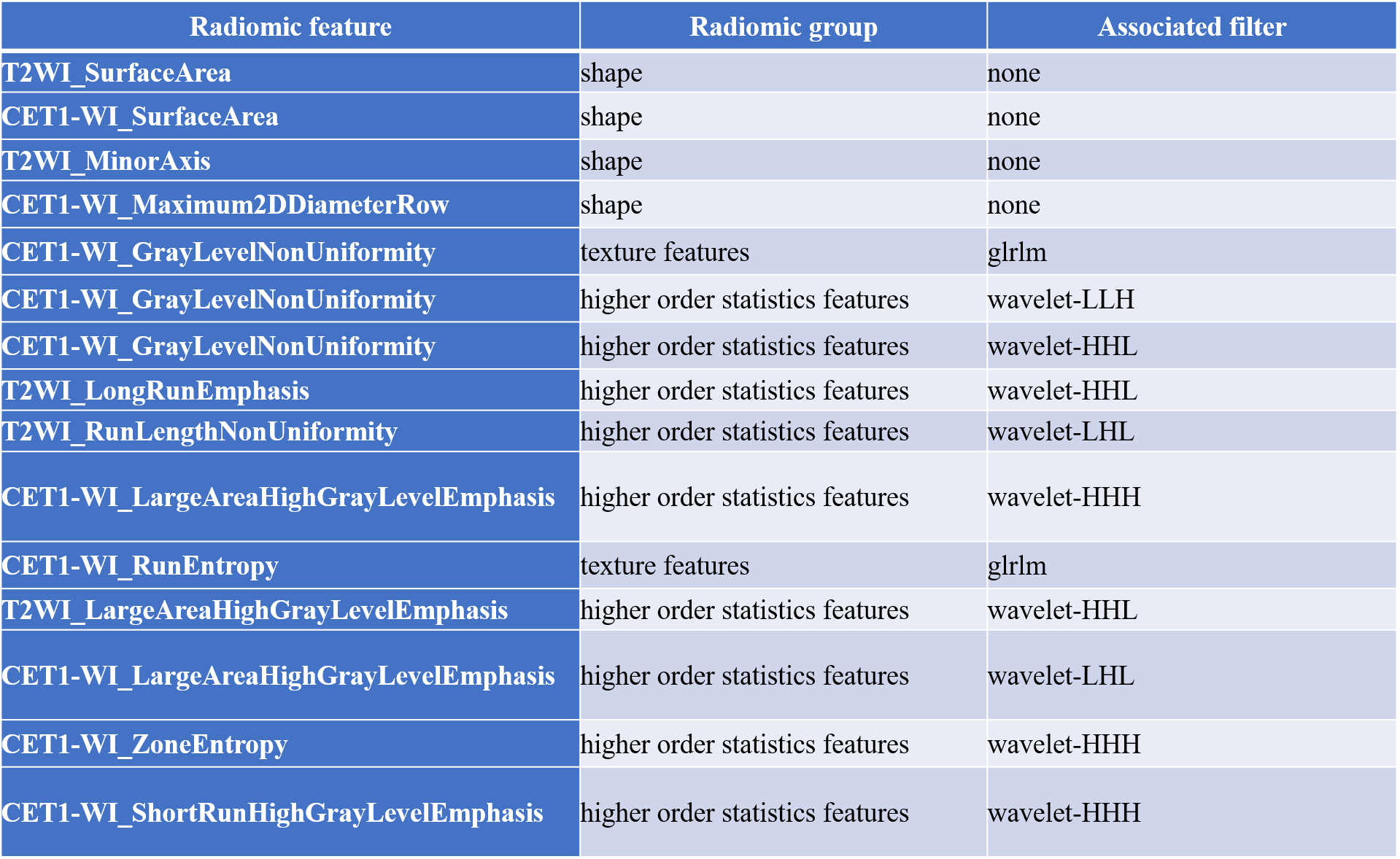
Table 1. 15 description of the selected radiomic features from joint CET1-WI and T2-WI images with their associated feature group and filter
Label: glrlm=Gray Level Run Length Matrix