2859
Novel Sequence for Improving Detection and Identification of Brain Tumor Lesions1Radiology, University of Cincinnati, Cincinnati, OH, United States, 2Radiation Oncology, University of Cincinnati, Cincinnati, OH, United States, 3Division of Biostatistics and Epidemiology, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, United States, 4Philips, Cincinnati, OH, United States
Synopsis
Early detection and accurate identification of
lesions are very important for diagnosis and treatment of brain tumors. Contrast-enhanced (CE) magnetic resonance imaging (MRI) is the gold standard method for the non-invasive
identification of primary brain tumors and cerebral metastases. In clinical
practice, current CE MRI protocols are acquired with an isotropic resolution
around 1.0 millimeter at 3.0 T that is limited by tumor-tissue
contrast to noise efficiency. In this investigation, our purpose was to improve
the efficiency by incorporating inversion recovery prepared spoiled gradient
recalled (IR-GRE) sequence with hybrid k-space and variable flip angles to reach
submillimeter resolution in clinical acceptable scan time.
PURPOSE
Early detection and accurate identification of brain tumors are very important for diagnosis and treatment. Contrast-enhanced (CE) magnetic resonance imaging (MRI) is the gold standard method for non-invasive identification of primary brain tumors and cerebral metastases. In clinical practice, current CE MRI protocols acquired with an isotropic resolution around 1.0 millimeter (mm) at 3.0 T1 are limited by tumor-tissue contrast to noise (CNR) efficiency. In this investigation, our purpose was to improve the efficiency by incorporating an inversion recovery prepared spoiled gradient recalled (IR-GRE) sequence with hybrid k-space and variable flip angles to reach submillimeter resolution in a clinically acceptable scan time.
METHODS
Simulation: Using the solution of Bloch equations in MATLAB (Math Works), we simulated contrast efficiencies between T1, T2, and proton density of CE tumor, and averaged white matter (WM) and gray matter (GM) at 3.0 T2. In the simulation, the values of T1, T2, and relative proton density of contrast enhanced lesions are assumed to be 400 ms, 200 ms and 0.8 at 3.0 Tesla3, respectively. The values of T1, T2, and relative proton density of normal brain tissue can be approximated by the averages of gray matter and white matter at 3.0 Tesla, which are 1150 ms, 95 ms, and 0.70, respectively after the administration of contrast agent.
In vivo experiment: Three patients with brain pituitary adenoma, high-grade glioma, intracranial metastases were respectively scanned on a 3T General Electric HDxt scanner equipped with a neurovascular array head coil after administration of 0.1 mmol/kg Gadavist (Bayer HealthCare). Brain images were obtained using both routine 3D IR-GRE sequence and then with our optimized parameters. The recommended 3D IR-GRE parameters by Food and Drug Administration (FDA) and Nation Cancer Institute (NCI)1 included: 1.0 mm isotropic resolution, TI 450 ms, and total scan time of 4 minutes and 30 seconds. Our proposed parameters included: 0.7 mm isotropic resolution, TI 500 ms, partial Fourier acquisition factor of 0.7, and total scan time of 4 minutes and 29 seconds.
RESULT AND DISCUSSION
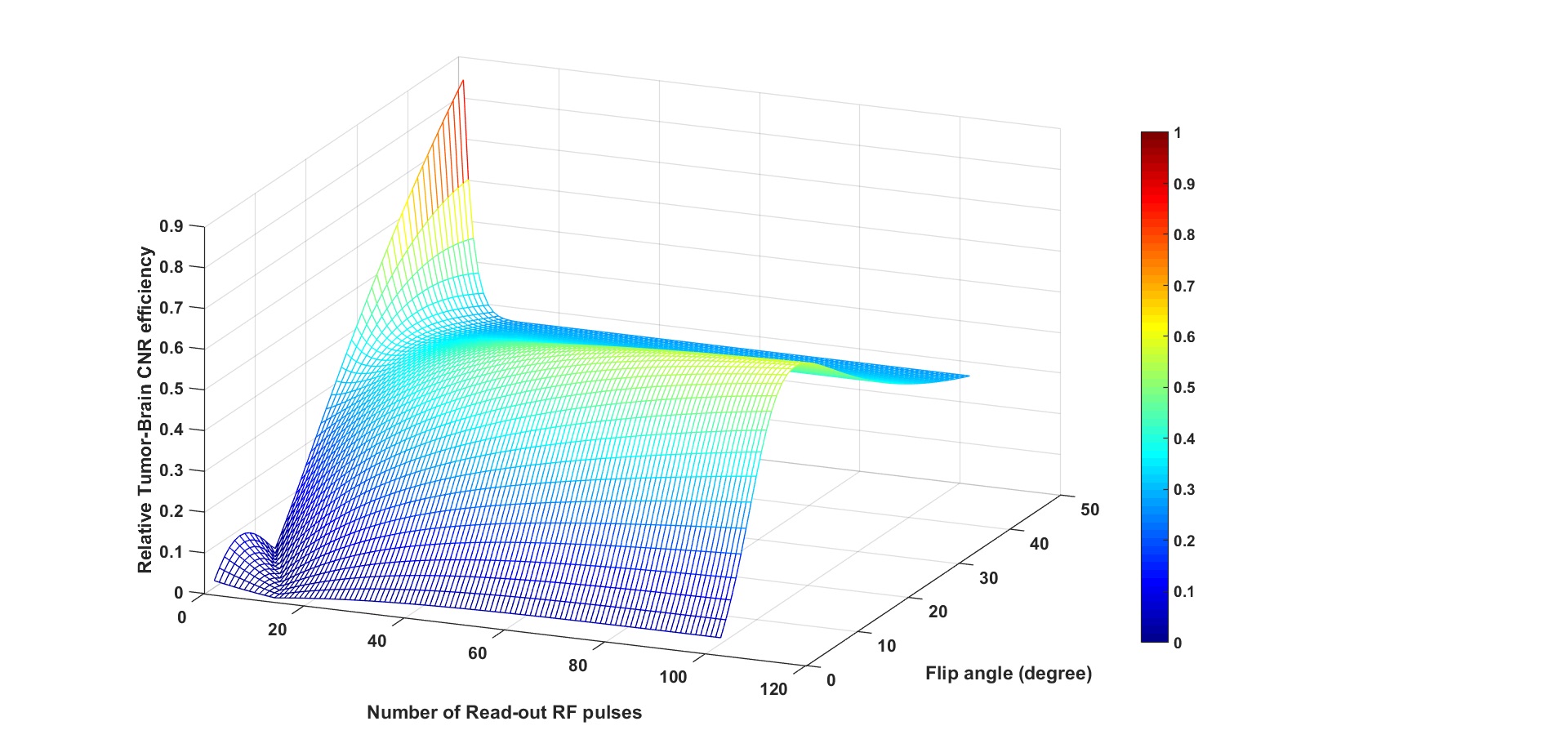
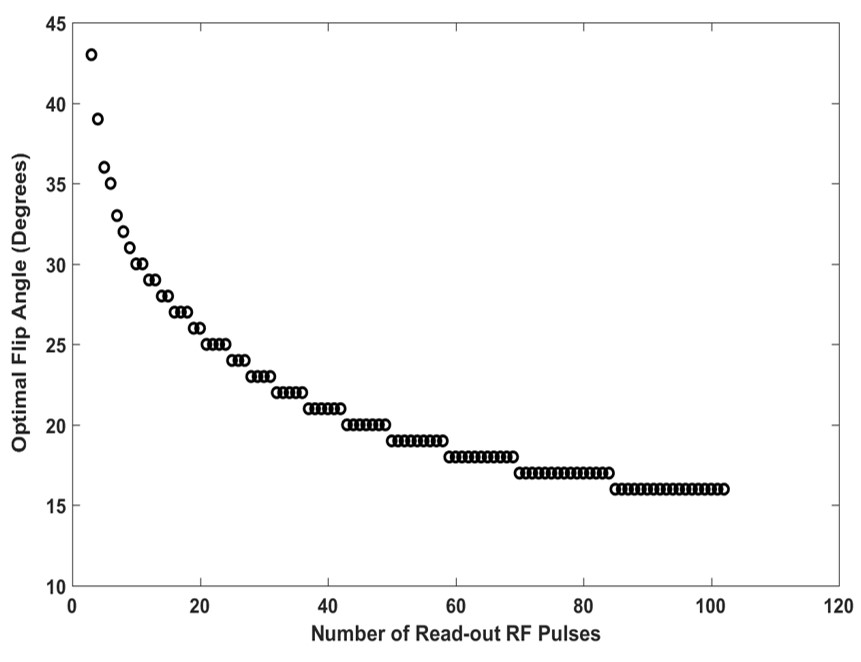
Figure 1 shows enhanced tumor-brain tissue CNR efficiency as a function of the number of echo acquisitions. At the transient state of excitation RF echo train, tumor-tissue CNR efficiency varies rapidly and reduces with the increasing echo acquisition before the transverse magnetization reaches a steady state. Further analysis indicated that the optimal variable flip angle distribution to maximize the enhanced tumor-brain tissue efficiency depends on the number of excitation radiofrequency pulses, as shown in Figure 2. The optimal flip angles and k-space strategy were determined across whole k-space because low and high spatial frequency k-space components respectively determine tumor- tissue CNR efficiency and spatial resolution.
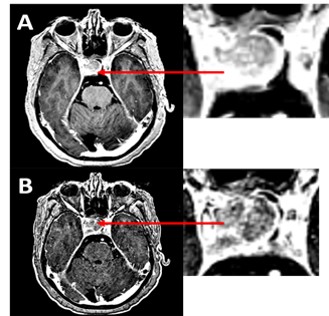
Figure 3 shows in vivo brain images acquired with IR-GRE protocol after the administration of 0.1 mmol/kg Gadavist. We compared our protocol (Fig. 3B) with the recommended protocol by FDA and NCI (Fig. 3A). The enhanced tumor lesion is more conspicuous and better delineation the image acquiring using our optimized sequence (Fig. 3B). Quantitative analysis indicates that the tumor-brain tissue CNR and its efficiency are approximately 39 and 2.4 s-1/2 for the recommended protocol, and 81 and 4.9 s-1/2 for our novel protocol. The CNR efficiency of our novel protocol is 104% higher than that of recommended protocol.
CONCLUSION
We incorporated an IR-GRE sequence with hybrid k-space and variable flip angles, and demonstrated improved tumor-brain tissue contrast efficiency by 104%. This novel protocol with ultra-high-resolution holds potential to better characterize enhancing lesions including detection of smaller lesions.
Acknowledgements
No acknowledgement found.References
1. Ellingson, B.M., et al., Consensus recommendations for a standardized Brain Tumor Imaging Protocol in clinical trials. Neuro-Oncology, 2015. 17(9): p. 1188-1198.
2. Wang, J., et al., Optimizing the magnetization-prepared rapid gradient-echo (MP-RAGE) sequence. PLoS One, 2014. 9(5): p. e96899.
3. Nöth, U., et al., Improved visibility of brain tumors in synthetic MP-RAGE anatomies with pure T1 weighting. NMR in Biomedicine, 2015. 28(7): p. 818-830.
Figures