2854
Differentiation between Vestibular Schwannomas and Meningiomas with Atypical Appearance using Diffusion Kurtosis Imaging and Three-dimensional Arterial Spin Labeling Imaging1Department of Radiology, Fujian Cancer Hospital & Fujian Medical University Cancer Hospital, Fuzhou, China, 2Department of Radiology, Fujian Medical University Union Hospital, Fuzhou, China, 3Philips Healthcare, Guangzhou, China
Synopsis
An accurate differentiation between vestibular schwannomas (VS) and meningiomas is critical in determining treatment strategies and clinical prognoses, but misdiagnoses may occur when typical imaging appearances are absent. We prospectively assessed the performances of diffusion kurtosis imaging (DKI) and three-dimensional arterial spin labeling imaging (3D-ASL) in the differentiation of VS and meningiomas with atypical appearance. Our study showed that DKI and 3D-ASL are useful for differentiating VS and meningiomas with atypical appearance, with kurtosis values of DKI have the best diagnostic efficiency.
Purpose
Vestibular schwannomas (VS) and meningiomas are the most common tumors in the cerebellopontine angle (CPA), but the treatment strategies and clinical prognoses for the patients with these two entities could be varied. Thus, an accurate differentiation of these two lesions is critically important. However, the differentiation may be difficult when typical imaging features are absent. The purpose of this study was to assess the performances of diffusion kurtosis imaging (DKI) and three-dimensional arterial spin labeling imaging (3D-ASL) in the differentiation of VS and meningiomas with atypical appearance.Methods
Thirty-eight patients with pathologically proven VS and meningiomas were consecutively enrolled. All patients had no typical appearance and underwent DKI and 3D-ASL scan. The MRI examinations were performed on a 3.0T MR scanner with an eight-channel receiver head coil. DKI used a SE-EPI diffusion sequence for image acquisition (TR/TE = 4,540/72.8 ms, NEX = 1, matrix = 256 × 256, sections thickness = 4 mm, spacing = 0 mm, FOV = 24 cm, number of b values = 3, b = 0, 1000 and 2000s/ mm2, number of directions = 30 for each, acquisition time = 4 min 51 seconds).1 3D-ASL imaging was performed by pseudo-continuous ASL pulse sequence using a stack of spirals with a background-suppressed 3D fast spin echo imaging sequences. The parameters used were: TR/TE = 4,653/10.5 ms, NEX = 3, matrix = 512 × 8, FOV = 24 cm, post-labeling delay = 1525 ms, slice thickness = 4 mm, inter-slice gap = 0 mm, acquisition time = 4 min 30 seconds.2 For MR diffusion imaging, Diffusional Kurtosis Estimator (version 2.5.1, Medical University of South Carolina) was implemented to calculate Mean kurtosis (MK), radial kurtosis (RK), axial kurtosis (AK), fractional anisotropy (FA), and mean diffusivity (MD) using the constrained linear least squares-quadratic programming algorithm.3 For MR perfusion imaging, cerebral blood flow (CBF) maps were automatically generated by the software FuncTool 9.4.05.4 The quantitative measurement of MR parameter maps was performed on Image J (Version 1.50i; U.S. NIH). We performed a semiautomatic ROI setting method, and the absolute values of tumors were used for comparison.1 Statistical analyses were performed using independent-sample t-tests, Mann-Whitney U tests and receiver operating characteristic (ROC) curve analyses.Results
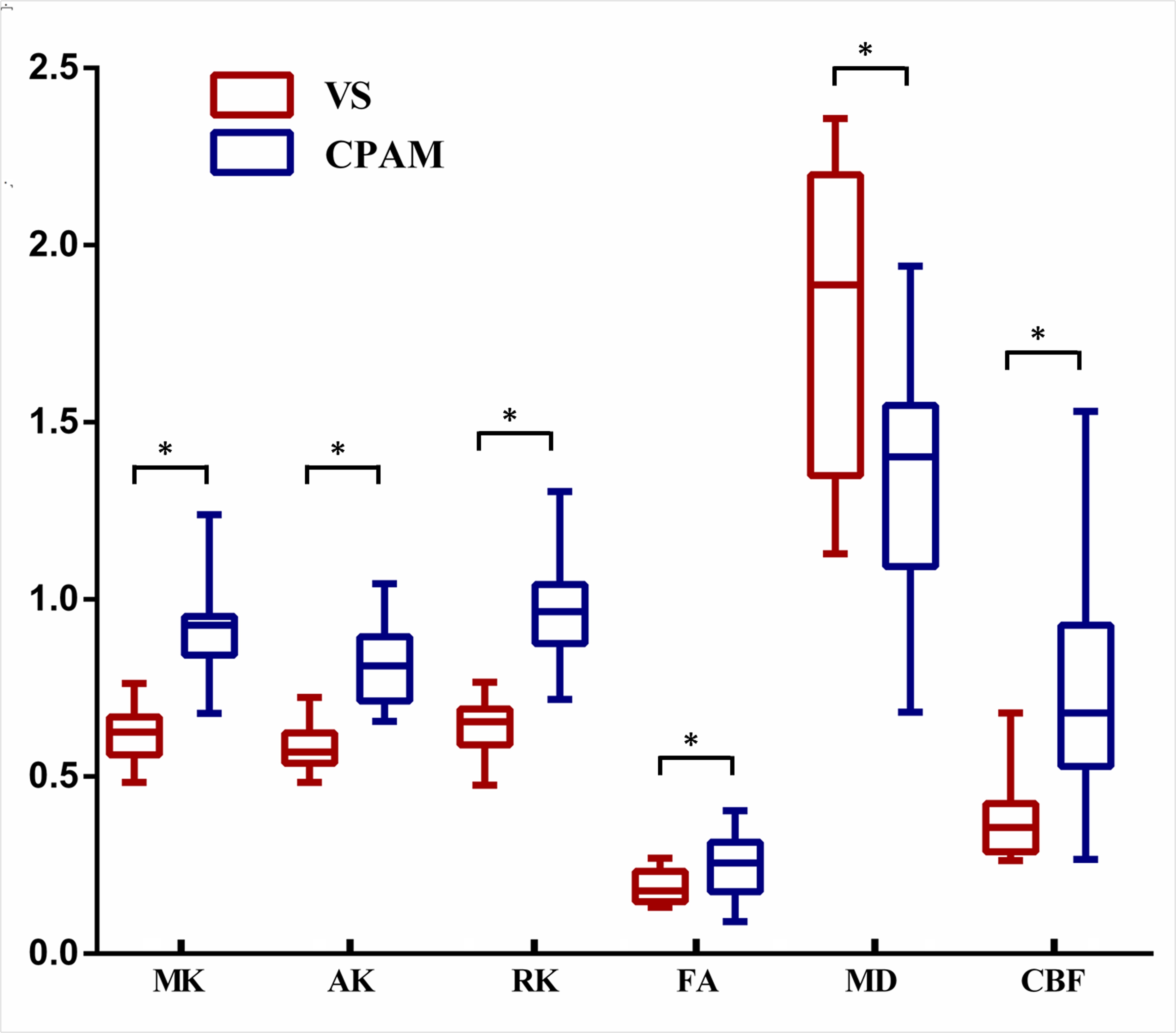
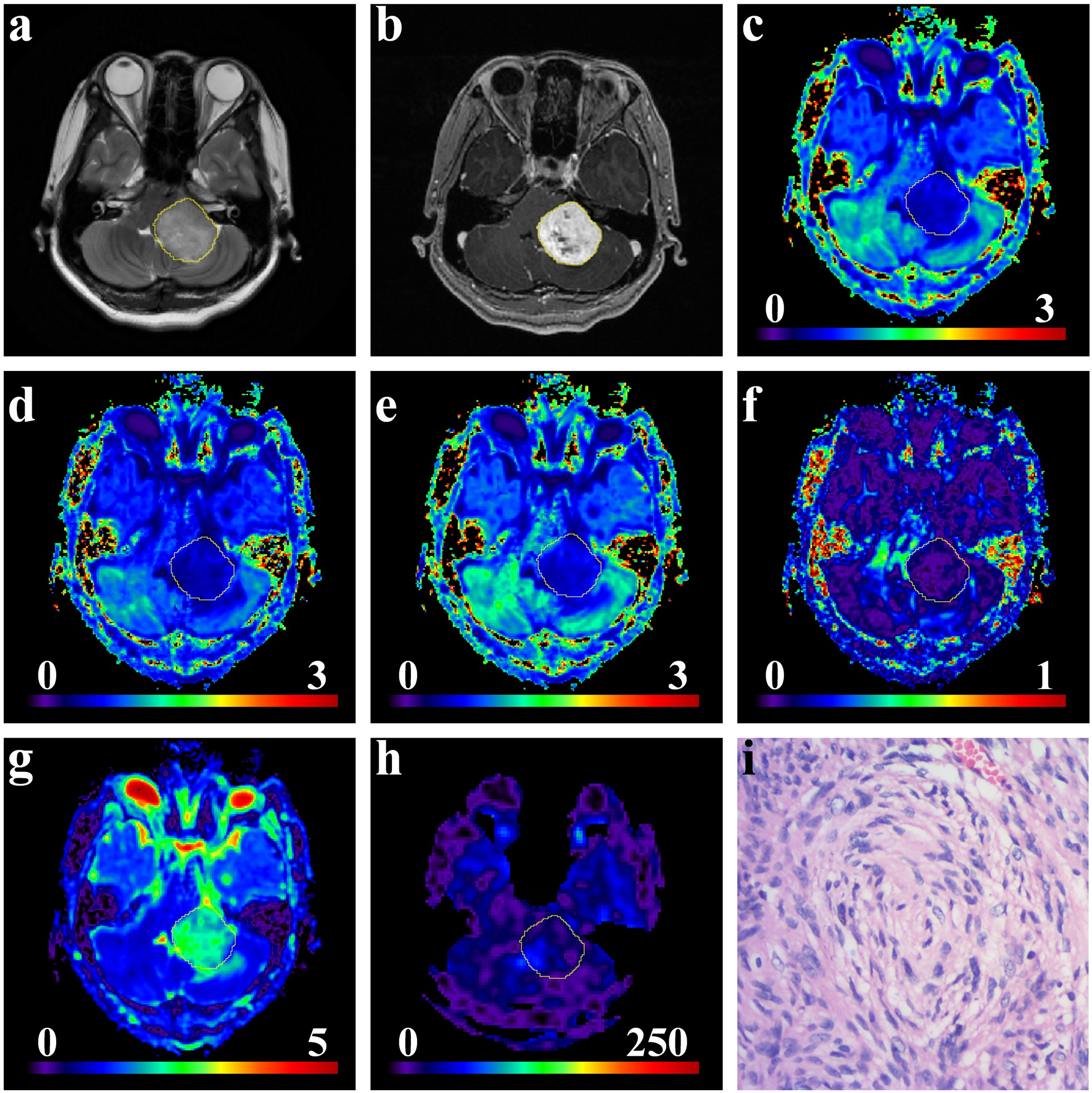
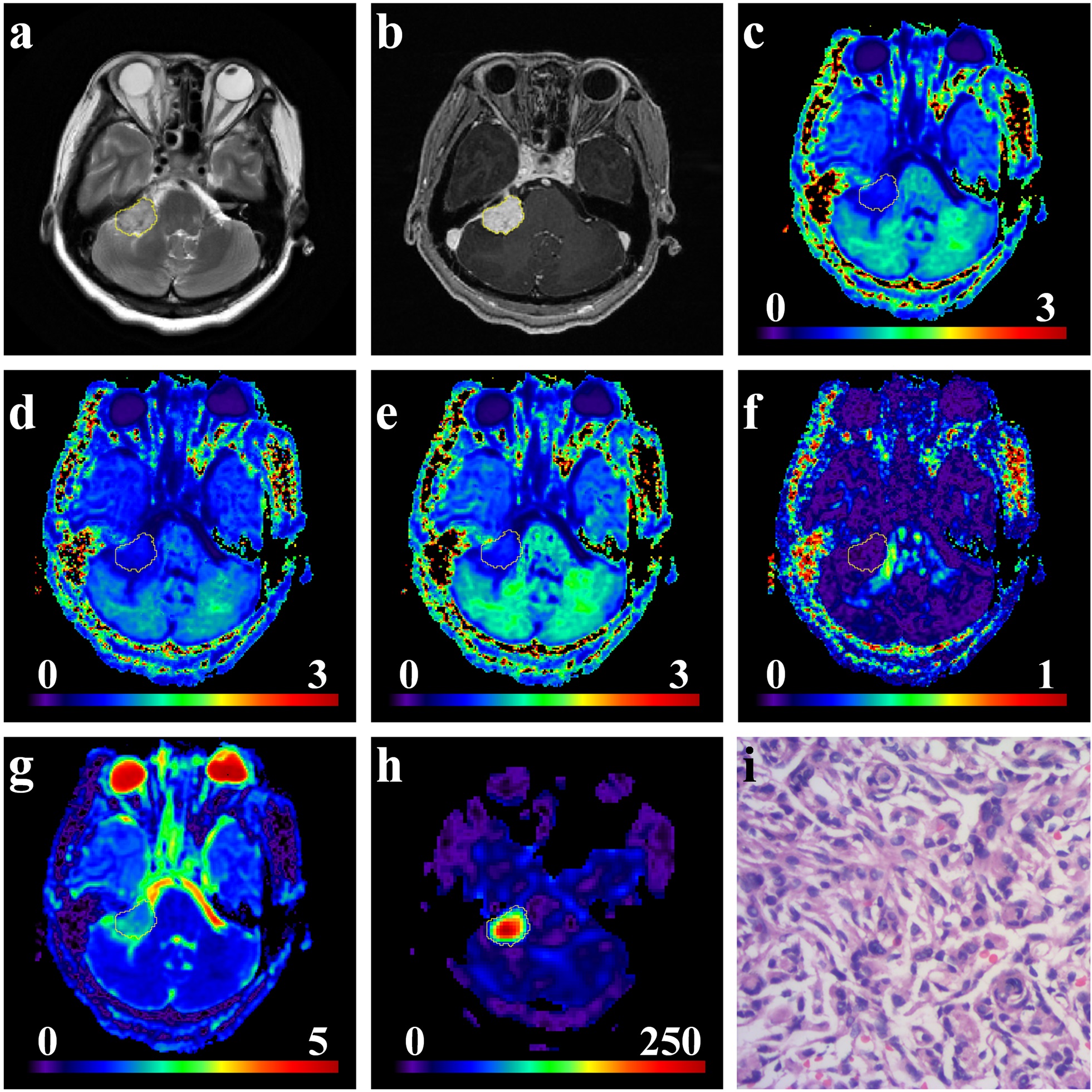
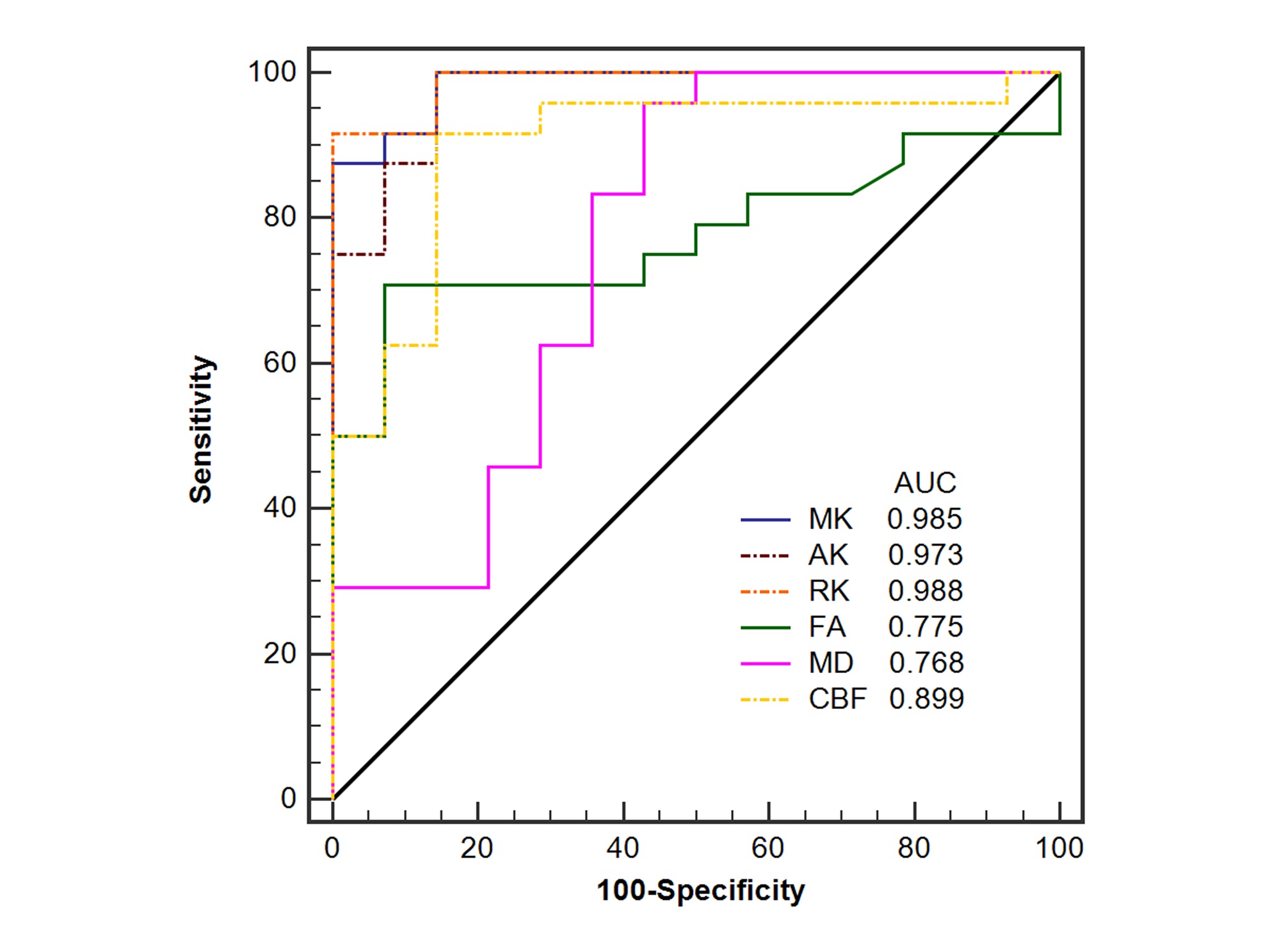
MK, RK, AK, FA and CBF were significantly lower in VS than those in meningiomas, MD were significantly higher in VS than that in meningiomas (all P < 0.05). Box-whisker plots were obtained to illustrate the group-wise differences (Fig. 1). Representative cases of VS and CPAM were illustrated in Fig. 2 and Fig. 3, respectively. Kurtosis metrics (MK, AK, and RK) had better diagnostic efficiencies than any other MR parameters for differentiating between VS and CPAM. The AUC, Youden Index, sensitivity, specificity and accuracy were 0.988, 91.67%, 91.67%, 100.0% and 94.74%, for a cut-off RK value of 0.766; the AUC, Youden Index, sensitivity, specificity and accuracy were 0.899, 77.38%, 91.67%, 85.71% and 89.47%, for a cut-off CBF value of 42.562 ml/100g/min. Moreover, The AUC values for kurtosis metrics were significantly greater than those for FA and MD in differentiating these two tumors (P < 0.05).Discussion and Conclusion
Advanced MRI techniques like DKI and 3D-ASL can provide microstructural heterogeneity and hemodynamic information of tumor tissues. Our study demonstrated that DKI and 3D-ASL are useful for differentiating VS and meningiomas with atypical appearance. A solid CPA tumor with high kurtosis/anisotropy/perfusion or restricted diffusion supports a diagnosis of meningioma. Conversely, low kurtosis/anisotropy/perfusion or facilitated diffusion is consistent with a diagnosis of schwannoma. Moreover, the ROC analyses showed that kurtosis values outperformed diffusion, anisotropy and perfusion values in differentiating these two tumors. And kurtosis metrics had significantly higher accuracy and potencies than diffusion and anisotropy values for discriminating them. Hence, the kurtosis metric may serve as a more appropriate MR metric for differentiating between VS and CPAM.Acknowledgements
No acknowledgement found.References
1. L. Lin, R. Bhawana, Y. Xue, Q. Duan, R. Jiang, H. Chen, X. Chen, B. Sun, H. Lin, Comparative Analysis of Diffusional Kurtosis Imaging, Diffusion Tensor Imaging, and Diffusion-Weighted Imaging in Grading and Assessing Cellular Proliferation of Meningiomas, AJNR. American journal of neuroradiology 39(6) (2018) 1032-1038.
2. L. Lin, Y. Xue, Q. Duan, B. Sun, H. Lin, X. Huang, X. Chen, The role of cerebral blood flow gradient in peritumoral edema for differentiation of glioblastomas from solitary metastatic lesions, Oncotarget 7(42) (2016) 69051-69059.
3. A. Tabesh, J.H. Jensen, B.A. Ardekani, J.A. Helpern, Estimation of Tensors and Tensor-Derived Measures in Diffusional Kurtosis Imaging, Magnetic resonance in medicine 65(3) (2011) 823-36.
4. D.C. Alsop, J.A. Detre, X. Golay, M. Gunther, J. Hendrikse, L. Hernandez-Garcia, H. Lu, B.J. MacIntosh, L.M. Parkes, M. Smits, M.J. van Osch, D.J. Wang, E.C. Wong, G. Zaharchuk, Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia, Magnetic resonance in medicine 73(1) (2015) 102-16.
Figures