2836
Cohort Stratification by Clinical Symptoms through Unsupervised Learning Reveals Metabolic and Microstructural Brain Alterations in Former American Football Players1Radiology, Brigham and Women's Hospital, Boston, MA, United States, 2Psychiatry Neuroimaging Laboratory, Brigham and Women's Hospital, Boston, MA, United States, 3Child and Adolescent Psychiatry, Ludwig-Maximilians-Universität, Munich, Germany, 4Boston University, Boston, MA, United States, 5Laboratory of Mathematics in Imaging, Brigham and Women's Hospital, Boston, MA, United States, 6Massachusetts General Hospital, Boston, MA, United States, 7VA Boston Healthcare System, Brockton, MA, United States
Synopsis
Chronic Traumatic Encephalopathy (CTE) is a neurodegenerative disease associated with exposure to repetitive head impacts. This study aims to characterize the differing clinical presentations of CTE using MR Spectroscopy and Diffusion Tensor Imaging. Unsupervised Learning was first used to divide a cohort of former NFL players into sub-groups based on the degree of mood/behavior symptoms and cognitive impairment relative to controls. The neurometabolite concentrations and measures of diffusivity were then compared between the sub-groups. Athletes with increased mood/behavior symptoms showed alterations reflective of neuroinflammation, whereas the cognitive impairment sub-group showed more neuronal and structural alterations.
Purpose
Chronic Traumatic Encephalopathy (CTE) is a neurodegenerative disease associated with exposure to repetitive head impacts. CTE can only be diagnosed post-mortem. The clinical symptoms of CTE include impairments in mood, behavior, cognition, and motor function1. Previously, the clinical symptoms have been divided into two broad categories: mood/behavior changes and cognitive decline1. The current study aims to better understand the clinical presentation of CTE in vivo through the use of Magnetic Resonance Spectroscopy (MRS), Diffusion Tensor Imaging (DTI), and neuropsychological/neuropsychiatric testing. MRS allows for the in vivo detection of a variety of neurometabolites such as glutathione (GSH), myo-inositol (mI), creatine (tCr), and N-acetyl aspartate (tNAA). DTI allows for the quantification of measurements of diffusivity, such as fractional anisotropy (FA) and trace.Methods
87 former NFL players and 23 healthy controls and former non-contact sports athletes from the DETECT study cohort were analyzed. Short echo, single voxel spectroscopy with a 32-channel head coil (3T, PRESS, TE=30ms, TR=2s, 128 averages, 2x2x2 cm3) was acquired in the posterior cingulate gyrus (PCG), parietal white matter (PWM), and anterior cingulate gyrus (ACG). Diffusion MRI was acquired using the following parameters: TR=11.7s, TE=85ms, FOV 256 mm, 128x128 matrix, 2.0 mm slice thickness, 73 slices were acquired using 64 diffusion directions, consisting of 59 diffusion-weighted images with multiple b values from 80s/mm2 to 3000s/mm2 and 5 images with b-value of 0s/mm2 for anatomical reference3. Clinical tests were divided into two categories: self-report measures of mood and behavior symptoms and objective measures of cognitive functioning. The K-means clustering algorithm was used to divide the NFL group into sub-groups based on the degree of mood/behavior symptoms and cognitive impairment relative to controls, in order to create homogenous groups within a heterogeneous dataset. The neurometabolite concentrations and measures of diffusivity were then compared between the groups. Multiple cluster analyses allow for investigation of metabolic and microstructural alterations among differing clinical presentations.Results
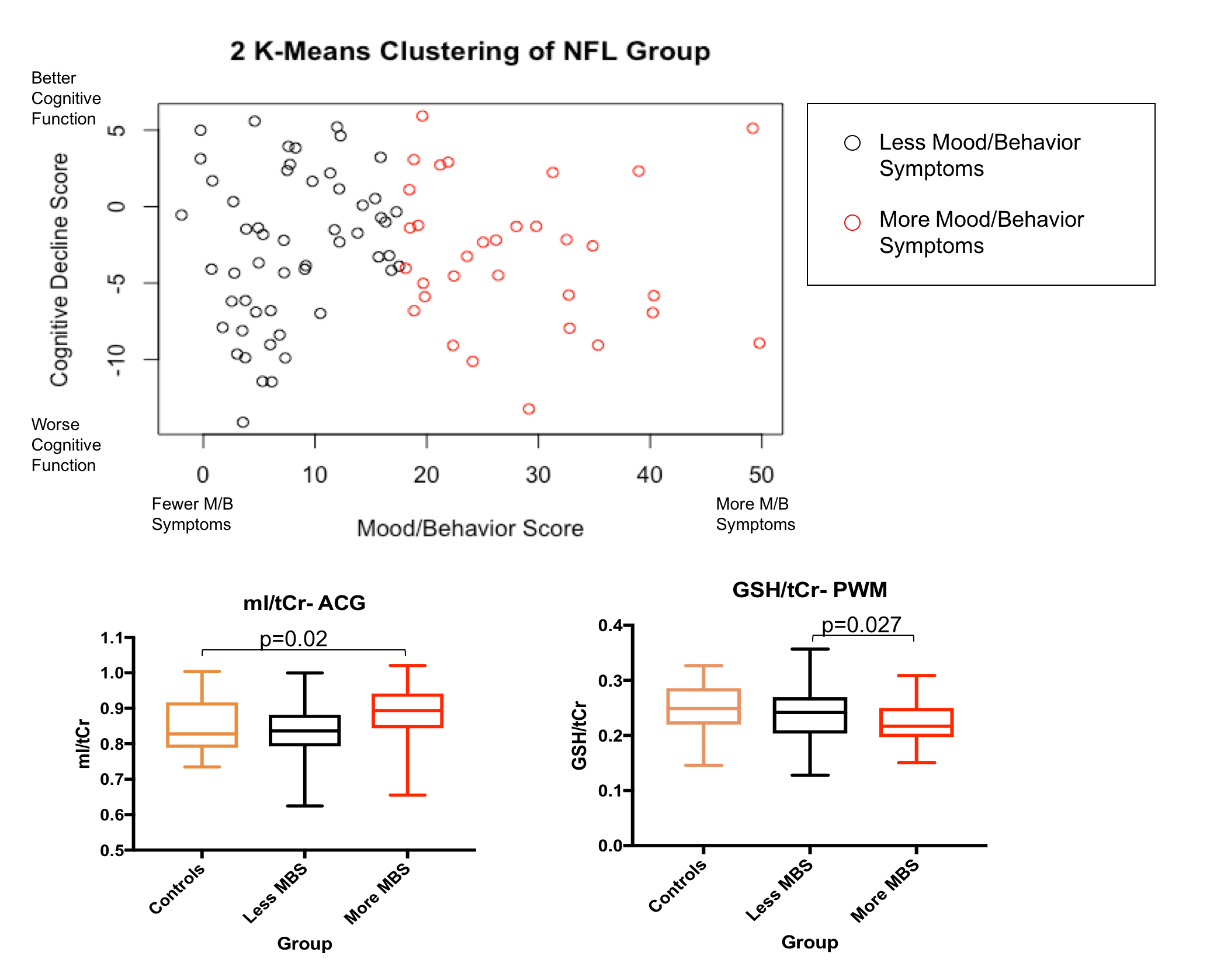
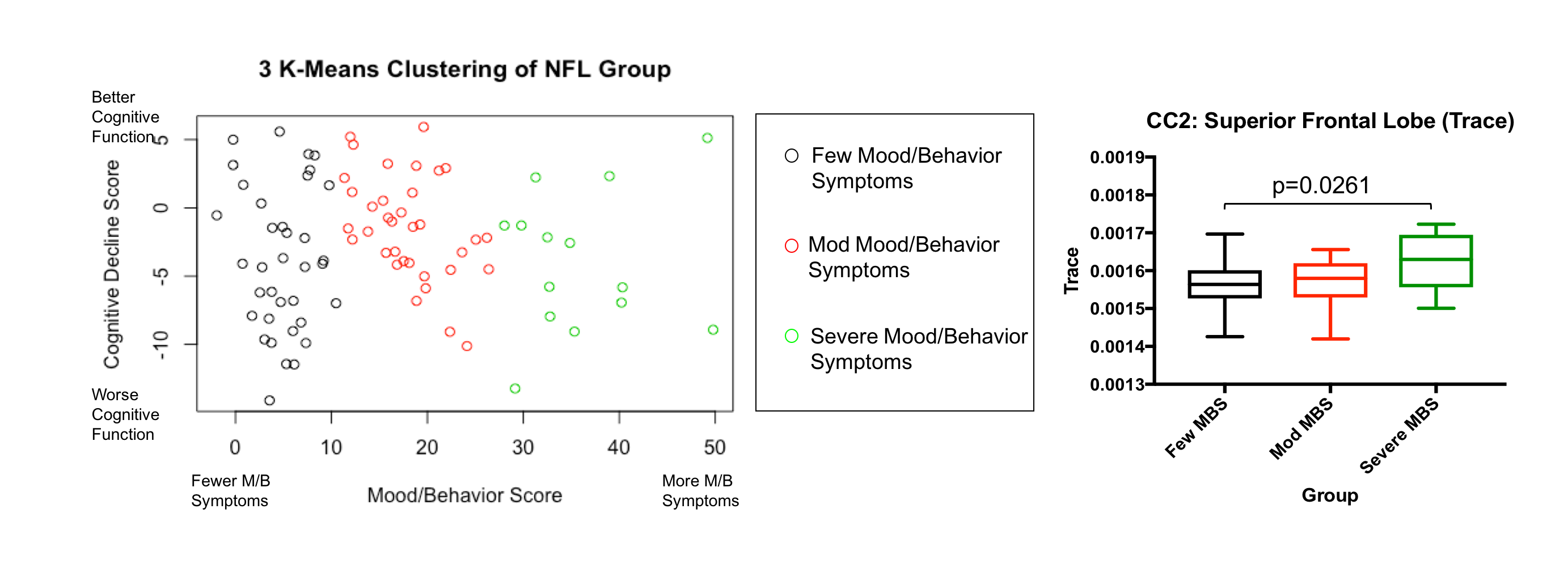
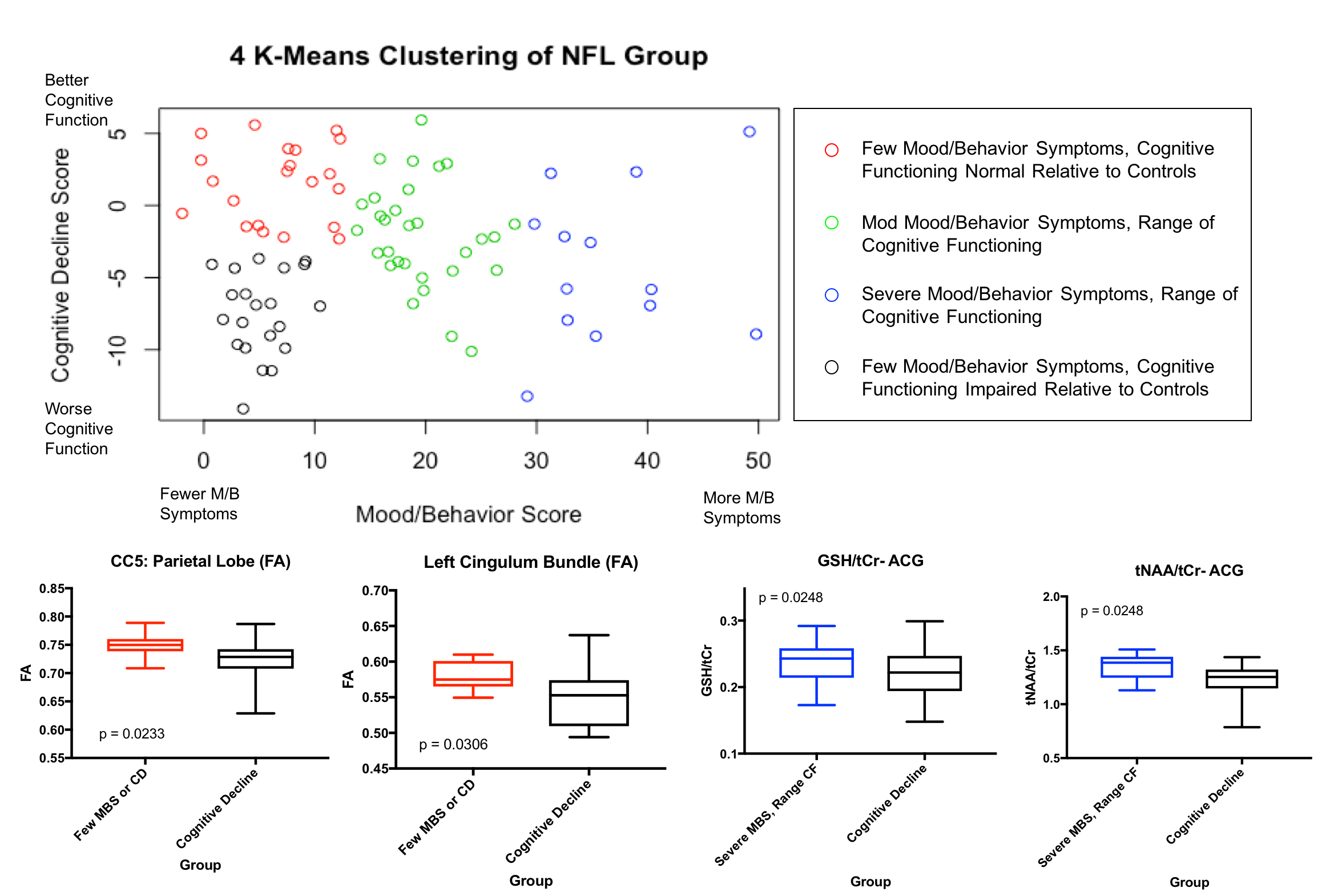
In the 2 K-means cluster analysis, the NFL group was divided into a subgroup with more mood and behavior symptoms and a subgroup with less mood and behavior symptoms, both with a range of cognitive decline. In the PWM, there was significantly decreased GSH/tCr (p=0.0463) in the group of NFL players with high mood and behavior symptoms compared to controls (Figure 1). In addition, a significant negative correlation between GSH/tCr and age was observed (p=0.0271). However, the group with high mood and behavior symptoms and decreased GSH/tCr was significantly younger than the low mood and behavior symptoms group (p=0.018), suggesting that these changes are not due to age. In the ACG, an increase in mI/tCr (p=0.02) was observed in the high mood and behavior symptoms sub-group compared to NFL players with less mood and behavior symptoms (Figure 1). In the 3 K-means cluster analysis, significantly increased trace in the Superior Frontal Tract of the Corpus Callosum (CC) (p=0.0261) was observed in the NFL players with the greatest mood/behavior symptoms compared to NFL players with the fewest mood/behavior symptoms (Figure 2). In the 4 K-means cluster analysis, one cluster represents NFL players with worse performance on cognitive measures and minimal mood and behavior symptoms. This group has significantly decreased tNAA/tCr (p=0.0104) and GSH/tCr (p=0.0248) in the ACG compared to a cluster of NFL players with the highest mood and behavior symptoms and a spectrum of cognitive performance (Figure 3). In addition, decreased FA was found in the Parietal Tract of the Corpus Callosum (p=0.0233) and Left Hemisphere Cingulum Bundle (CB) Tract (p=0.0306) in the NFL players with worse cognitive performance compared to those with few mood/behavior symptoms and normal cognitive functioning (Figure 3).Conclusion
These results suggest that differing metabolic and microstructural alterations occur along a spectrum of mood and behavior symptoms and cognitive functioning in former NFL players at increased risk for CTE. Alterations in GSH and mI suggest neuroinflammation is associated with mood and behavior symptoms. A decrease in NAA in former NFL players with cognitive decline may suggest neuronal loss in these subjects. Increased trace in the superior frontal tract of the CC in NFL players with more mood/behavior symptoms suggests an association between white matter microstructural alterations and neuropsychiatric symptoms. In addition, decreased FA in the worse cognitive performance sub-group in tracts associated with sensory processing in the CC and working memory in the CB provides further evidence of microstructural alterations in white matter tracts associated with clinical/cognitive presentation. Additional studies are needed to correlate these results with neuropathology.Acknowledgements
We would like to acknowledge the following funding source: R01AG038758-01References
1. Stern, Robert A. et al. “Clinical Presentation of Chronic Traumatic Encephalopathy.” Neurology 81.13 (2013): 1122–1129.
2. Alosco, Michael L. et al. “Magnetic Resonance Spectroscopy as a Biomarker for Chronic Traumatic Encephalopathy.” Semin Neurol 37.5 (2017): 503-509.
3. Zhang, Fan. et al. “An anatomically curated fiber clustering white matter atlas for consistent white matter tract parcellation across the lifespan.” NeuroImage 179 (2018): 429-447.
Figures