2821
Sodium MRI at 21.1 T to Assess Stroke Recovery Following Adult Human Mesenchymal Cell Transplantation1National High Magnetic Field Laboratory, Florida State University, Tallahassee, FL, United States, 2Chemical & Biomedical Engineering, FAMU-FSU College of Engineering, Tallahassee, FL, United States, 3Center of Excellence for Aging & Brain Repair, University of South Florida, Tampa, FL, United States
Synopsis
This study evaluates recovery following transplantation of human mesenchymal stem cell (hMSC) aggregates labeled with micron-sized particles of iron oxide (MPIO) in a rodent model of ischemic stroke at 21.1 T. Unlike previous studies using single cells, intact aggregates were implanted directly into the contralateral ventricle. Longitudinal MRI post-implantation was used to investigate T2-weighted lesion volume and sodium (23Na) distribution as well as hMSC aggregate localization and cell migration following middle cerebral artery occlusion. MR results correlate with behavioral assessments and histology of tissue recovery. In particular, sodium decreases indicate recovery of tissue homeostasis following hMSC aggregate implantation.
Introduction
Stroke is a leading cause of long-term disability in the United States, with ~800,000 people suffering a stroke annually.1 Human mesenchymal stem cells (hMSC) have shown therapeutic effects following neurological damage, and are a promising approach to minimize acute and chronic injury.2 Most studies and clinical trials have evaluated dissociated hMSC in treatment of stroke3, but the use of cell aggregates may increase therapeutic benefit. Here, hMSC aggregates were intraventricularly transplanted into ischemic and naïve rats. High resolution 1H fast spin echo (FSE) and gradient recalled echo (GRE) images were acquired at 21.1 T to track lesion recovery and cell dissociation. Initially elevated sodium distributions measured from 3D 23Na GRE scans demonstrated reductions in volume and signal following aggregate administration.Methods
Cell Source and Animal Model: hMSC were acquired from the Tulane Center for Stem Cell Research and Regenerative Medicine. A WAVE bioreactor (GE Healthcare, PA) was utilized to induce 400-µm diameter hMSC aggregation that were cultured individually prior to implantation. At 24-h before implantation, aggregates were exposed to 0.45-µg/mL micron-sized particles of iron oxide (MPIO) labeled with a green fluorophore for 12 h. Transient Middle Cerebral Artery Occlusion (MCAO) was instituted following techniques previously established5 using a rubber coated filament (Doccol Corp., MA) for 1.5 h. Sprague-Dawley rats (200-250 g) were assigned randomly to the following groups: MCAO with aggregates (MCAO+Agg; n=6), MCAO with saline vehicle (MCAO+PBS; n=7), or naïve with aggregates (Naïve+Agg; n=5). Immediately after MCAO, twenty MPIO-labeled hMSC aggregates suspended in phosphate buffered saline (PBS) or PBS alone were injected into the contralateral ventricle of MCAO rats and compared to aggregates injected into naïve rats. Behavioral assessments were conducted concurrently with MR scanning. Following, the animals were transcardially perfused with 4% paraformaldehyde for ex vivo MRI and immunohistochemistry (IHC).
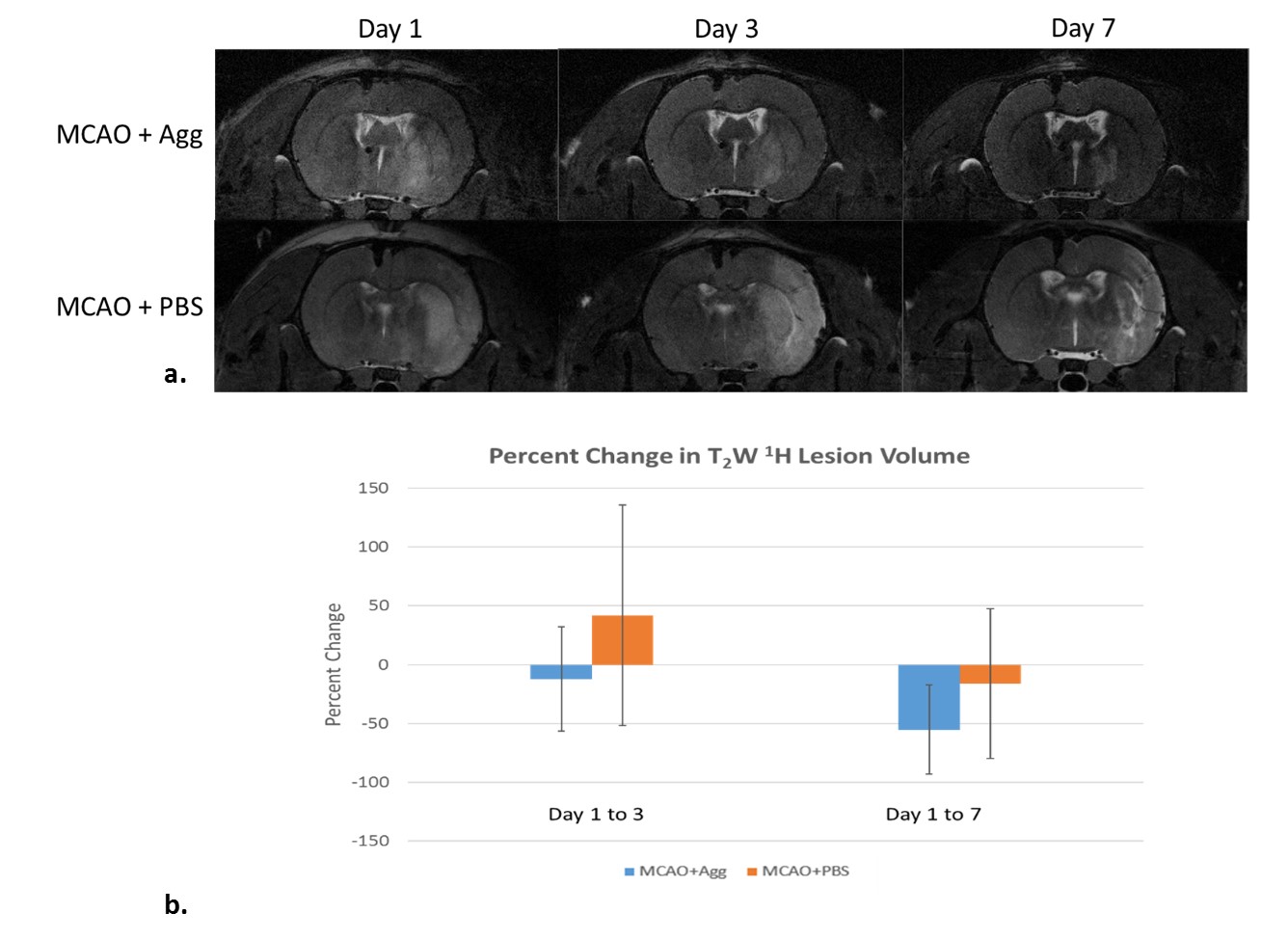
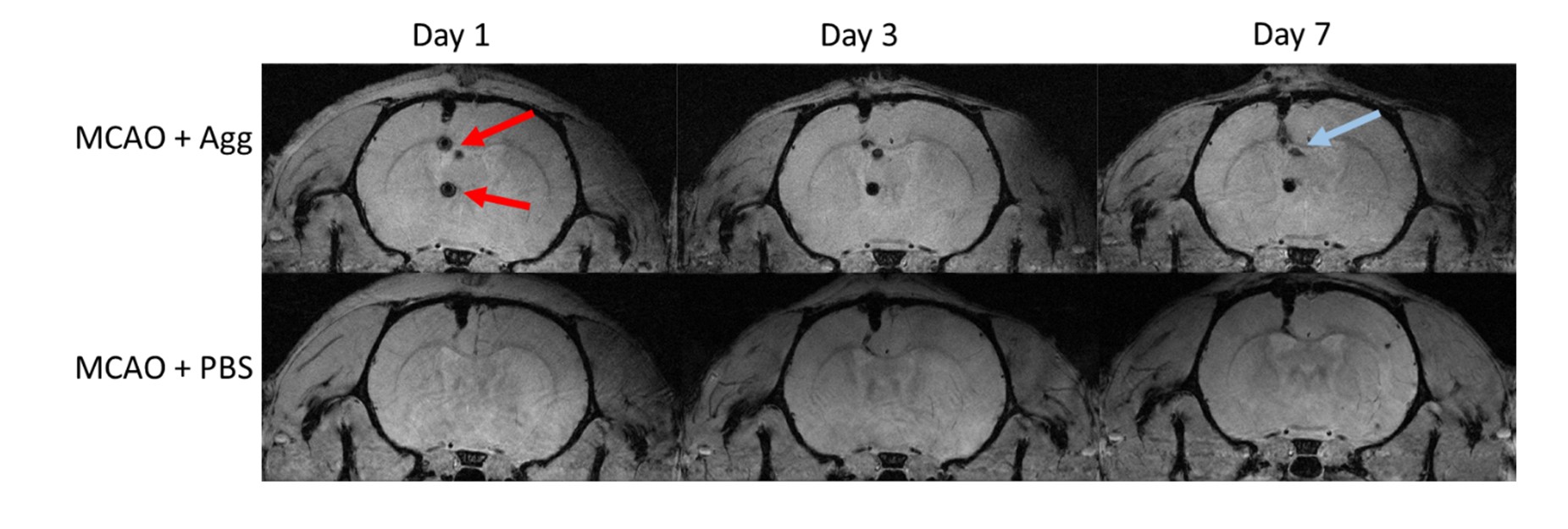
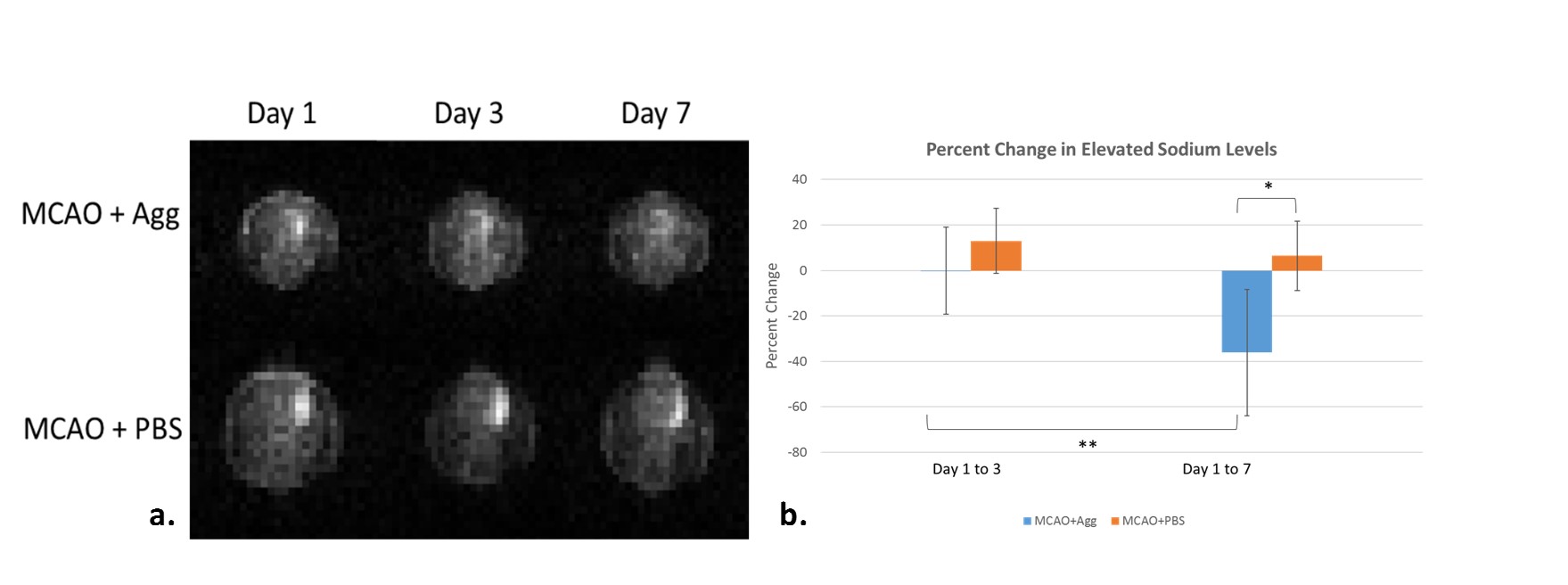
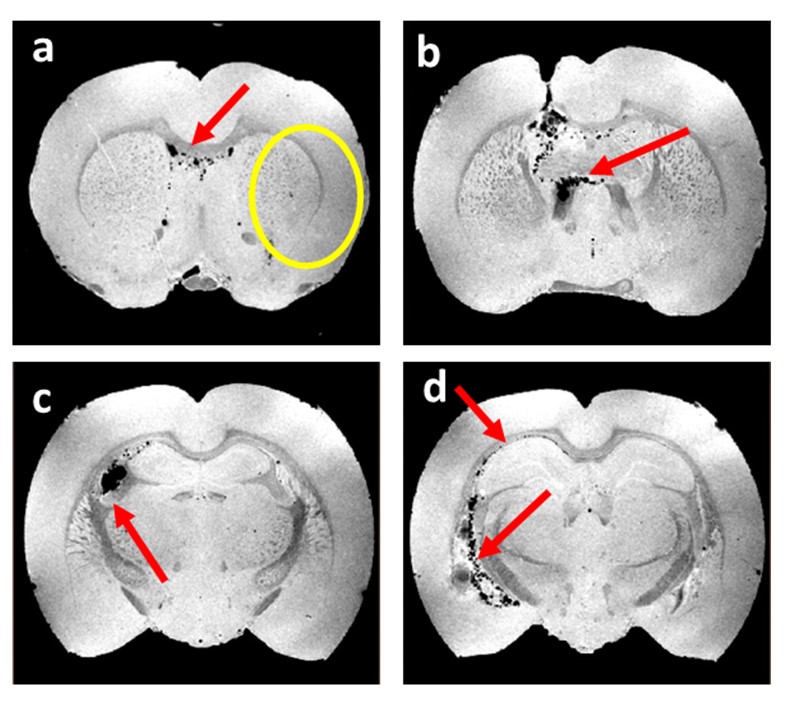
MR Acquisition: High resolution MRI was acquired in vivo on day 1, 3 and 7 post-MCAO utilizing the 21.1-T magnet at US National High Magnetic Field Laboratory (NHMFL). T2-weighted images were generated utilizing a 1H FSE sequence with 100x100-µm in-plane resolution to measure ischemic lesion volumes (Fig.1). Aggregate localization within the ventricular system and cell dissociation were assessed using a 1H GRE sequence with 50x50-µm in-plane resolution (Fig.2). Functional recovery of sodium homeostasis was evaluated via 3D 23Na GRE at 1.6-mm isotropic resolution (Fig.3a). Ex vivo images were acquired at 50-µm isotropic resolution using a 3D GRE at 11.75 T to assess cell dissociation from implanted aggregates (Fig.4).
Analysis: Data were reconstructed to quantify lesion volume and aggregate/cell location. Ischemic lesion was delineated based on thresholding defined by average contralateral signal and standard deviation (SD) on day 1 post-MCAO for 1H FSE (threshold = +1 SD) and 23Na GRE (threshold = +2.5 SD). Percent changes in lesion volumes were measured (Fig.3b) relative to day 1 post-MCAO.
Results
Hyperintense 1H signal in T2W images corresponding to the ischemic lesion decreased longitudinally on day 3 and 7 post-MCAO (Fig.1). However, no significant changes were seen between groups for percent change in 1H lesion volumes. In vivo 1H GRE scans demonstrate successful aggregate implantation with prolonged retention of MPIO-labeled aggregates (Fig.2). Evidence of cell dissociation from aggregates was confirmed in ex vivo 3D GRE data (Fig.4) and IHC (Fig.5). Significant decreases in 23Na lesion volume from day 1 to 7 in the MCAO+Agg group were evident compared to the MCAO+PBS (ANOVA with Tukey HSD, p=0.0106) and indicate improved recovery with aggregate implantation (Fig.3).
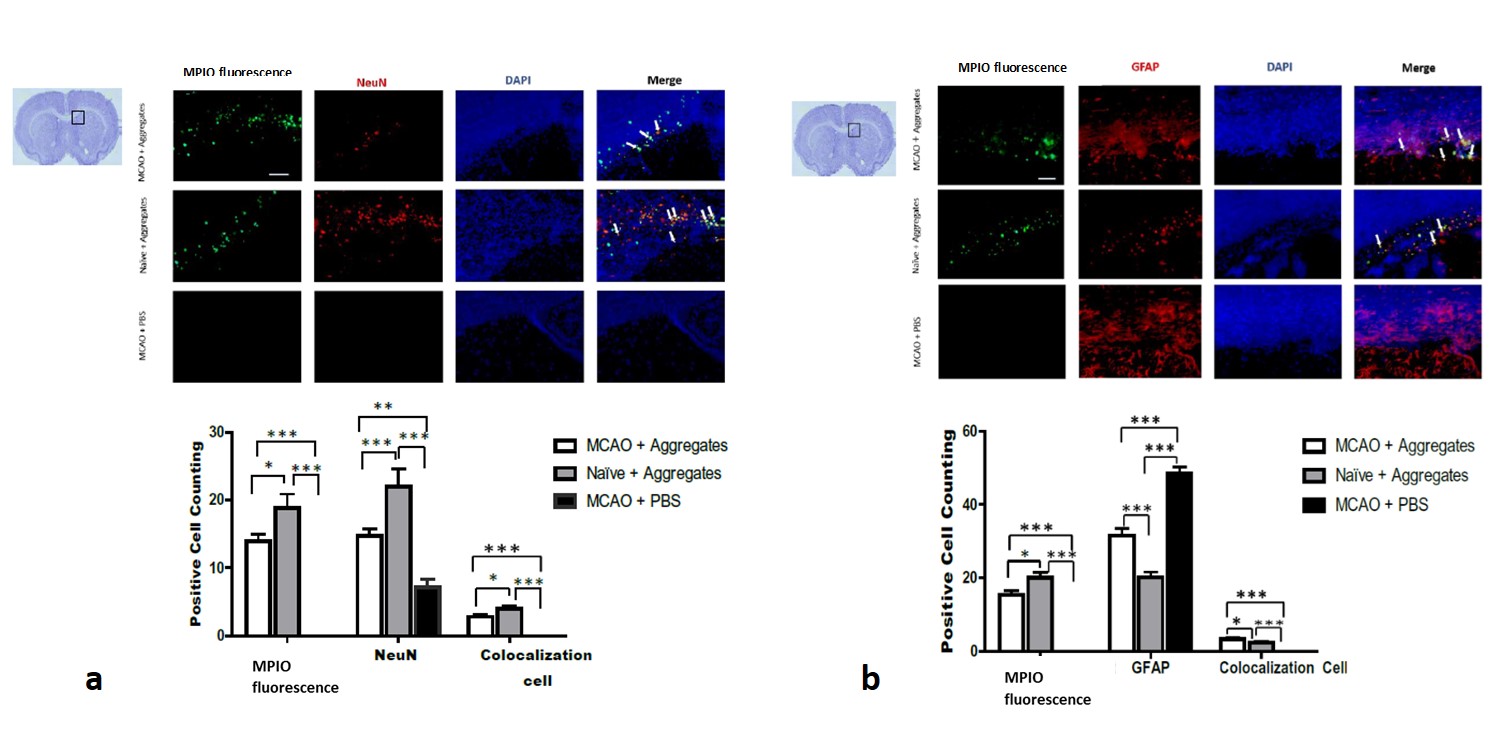
Behavioral assessments of limb-asymmetry demonstrate longitudinal improvement correlated with recovery of sodium homeostasis; significant improvements were identified for the MCAO+Agg group compared to MCAO+PBS (data not shown). IHC (Fig.5) shows co-localization of MPIO and hMSC indicating intracellular retention of MPIO by hMSC. Importantly, neuron differentiation (NeuN) is significantly increased in MCAO-Agg animals compared to MCAO-PBS.
Discussion
Sodium was the most MR sensitive parameter of lesion recovery resulting from aggregate implantation, indicating recovery of ionic homeostasis and supported by behavioral and IHC measures. Significantly increased NeuN staining for neuronal differentiation in aggregate implanted animals provides evidence of endogenous recruitment towards the ischemic lesion. Significantly increased GFAP staining in MCAO+PBS compared to MCAO+Agg suggests improvements in astrocyte scaring6 with treatment. Co-localization of human cell markers in proximity to MPIO fluorescence supports retention of hMSC within cerebral tissue.Conclusions
Recovery of 23Na homeostasis and neuronal differentiation in acute stroke demonstrate that hMSC aggregates promote tissue recovery. Natural resistance to ischemic environments7,8 and larger aggregate size could contribute to the prolonged retention in ischemic cerebral tissue while providing an enhanced dose of regenerative cytokine secretions and an extended cell therapy source.Acknowledgements
All work has been conducted in accordance with the FSU Animal Care and Use Committee. Funding provided by NIH (RO1-NS102395). The National High Magnetic Field Laboratory is supported by the National Science Foundation through the NSF (DMR-1644779 & DMR-1644779) and State of Florida.References
1. Benjamin EJ, et al. 2017. AMA, Statistics Committee and Stroke Statistics Subcommittee.
2. Wakabayashi K., et al. 2010. JNR. 88:1017-1025.
3. NIH. 2018. ClinicalTrials.gov.
4. Lee V., et al. 2012. Translational Stroke Research. 3(2):236-245
5. Longa E.Z., et al. 1989. Stroke. 20(1):84-91.
6. Sofroniew M.V., et al. 2010. Acta Nueropahtol. 119(1):7-35.
7. Ma T., et al. 2015. Tissue Eng Part A. 21(9-10):1705-1719.
8. Ma T., et al. 2014. Tissue Eng Part B Rev. 20(5):365-380.
Figures