2808
Endovascular thrombectomy using stentretrievers affects the vessel wall: impact demonstrated by wall enhancement at 7T1Medical Imaging Neuroradiology, Skåne University Hospital Lund, Lund, Sweden, 2Dept. of Clinical Sciences, Lund University, Lund, Sweden, 3Lund University Bioimaging Center, Lund University, Lund, Sweden, 4Philips Healthcare, Copenhagen, Denmark, 5Dept. of Neurology, Skåne University Hospital Lund, Lund, Sweden, 6Dept. of Diagnostic Radiology, Skåne University Hospital Lund, Lund University, Lund, Sweden
Synopsis
Stroke is increasingly treated by removing the vessel obstruction via endovascular thrombectomy. 3T imaging has shown wall enhancement after endovascular thrombectomy, and we hypothesize that 7T MR will be beneficial to visualize this enhancement as the higher field strength allows for higher resolution imaging. Seven patients were examined at 7T within two days after endovascular thrombectomy. Vessel wall images pre- and post-contrast administration were reviewed by two neuroadiologists, who rated the image quality as excellent in all cases. In all patients, wall enhancement was found, and correlated to the site of the stent-retriever rather than the site of the embolus.
Introduction
Stroke is a large cause of mortality, dementia and adult disability worldwide. Endovascular thrombectomy has rapidly been established as the standard care for acute stroke with large vessel occlusion [1,2]. Studies at 3T show that the vessel wall is affected by the procedure [3,4]. However, as imaging of the vessel wall requires high-resolution acquisitions, and the black blood MR sequences used inherently have low SNR, we hypothesize that imaging of the vessel wall injury after mechanical thrombectomy will benefit from 7T.Materials and Methods
Seven patients (age range 55-84 years) treated with endovascular thrombectomy for acute stroke in the anterior circulation were included in the study. All had a CTA verified thrombus in the distal internal carotid artery or M1 or M2 segments of the Middle Cerebral Artery. The study was approved by the local ethics committee and written informed consent was obtained from all patients. A 7T examination (Philips Achieva AS, Best, The Netherlands) was performed within two days after the thrombectomy. Black blood vessel wall images were acquired using a 3D magnetization prepared inversion recovery turbo spin-echo (3D MPIR-TSE [5,6]) with 0.8 mm isotropic resolution. Full brain coverage was obtained in 8:30 min. The vessel wall imaging was performed prior to contrast agent administration (pre-Gd) (0.2 ml/kg bodyweight, Dotarem, Gothia Medical, Sweden), as well as twice post contrast (first and second post-Gd).
To reduce motion artifacts during the long vessel wall scans, prospective motion correction was applied (iMOCO [7,8]). This correction is based on a fat-selective navigator which is played out in each echo train. The navigator image is registered to the first image, and the scan geometry is updated in real-time. If the motion exceeds a set threshold, the last data is required, which prolongs the scan.
Image grading was made independently by two neuroradiologists. First, the images were reviewed for location of any vessel wall enhancement, the amount of motion artifacts was graded on a predefined scale, and over-all image quality was graded in all three contrast phases according to another pre-defined scale. Secondly, the location of Gd-uptake in the vessel wall was correlated to the locations of the embolus, based on the pre-operative CT angiography, and the stent-retriever, based on the pre-operative DSA images.
Results
In general, all patients tolerated the examination well. In three cases, the examination was terminated after the first post-contrast scan due to patient discomfort (two cases) or technical issues (one case).
In all patients, both reviewers agreed that vessel wall enhancement was present and that it correlated to the site of the stent-retriever rather than the site of the embolus.
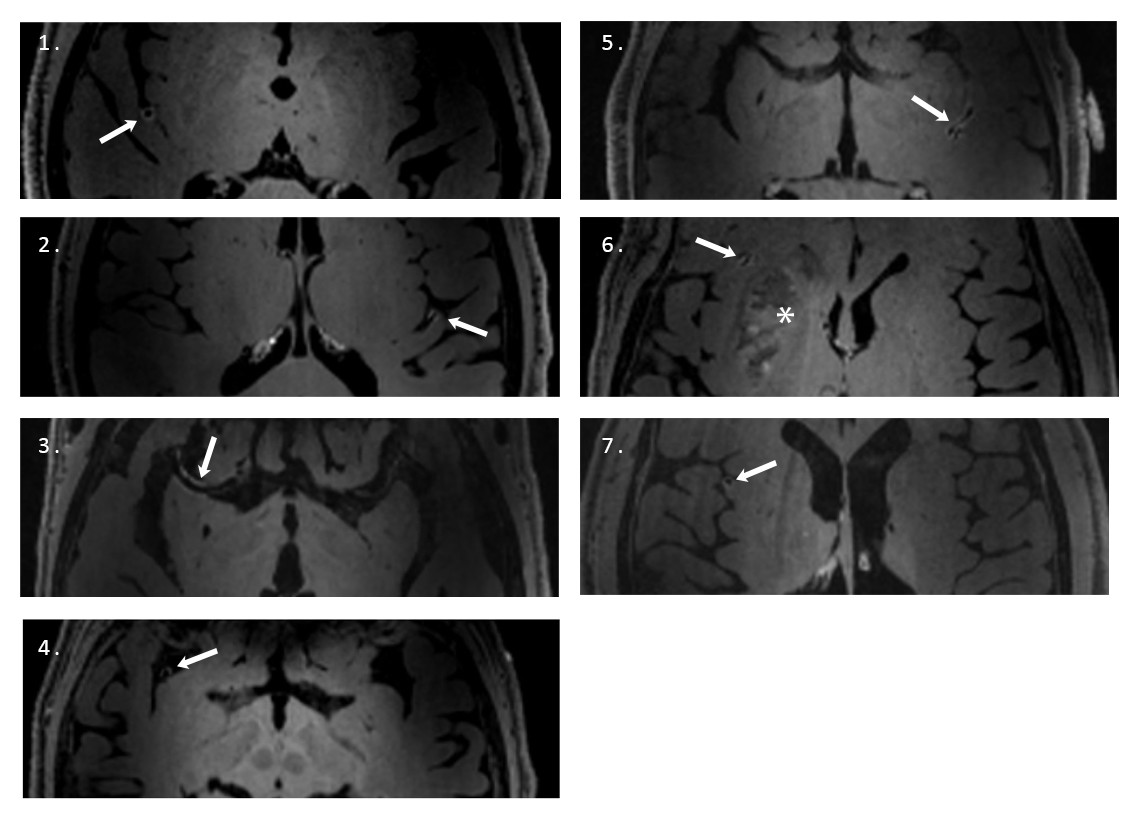
Figure 1 shows axial images from the first post-Gd vessel wall 3D MPIR-TSE from all seven patients. The wall enhancement at the site of the stent-retriever is marked with an arrow. The images also demonstrate the lack of enhancement on the contralateral side.
The results of the image assessment by the two reviewers are shown in Table 1. Overall image quality was graded highest on a 3-grade scale for all contrast phases, with complete agreement between the reviewers. Motion artifacts was not rated as “impairing the diagnostic quality” for any case by any reviewer. This is noteworthy as there in several cases was considerable patient motion during the long scans, indicating that the prospective motion correction strategy was efficient.
Conclusions
To draw firm conclusions, a larger number of subjects need to be included in the study. Longitudinal data could reveal if the wall enhancement persists for an extended period of time.
Overall, 7T vessel wall imaging in the sub-acute phase following endovascular thrombectomy seems safe, robust and reliably yields excellent diagnostic images. The location of contrast enhancement corresponds with the location of the stent-retriever deployment rather than the location of the embolus.
Acknowledgements
Lund University Bioimaging Center (LBIC), Lund University is gratefully acknowledged for providing experimental resources.
The authors are grateful to Prof. Dr. J. Hendrikse, UMC Utrecht, for providing the 3D MPIR-TSE sequence.
References
1. O. A. Berkhemer et al., A randomized trial of intraarterial treatment for acute ischemic stroke, N. Engl. J. Med. 372(1): p. 11-20 (2015)
2. D. M. Mandell et al., Intracranial Vessel Wall MRI: Principles and Expert Consensus Recommendations of the American Society of Neuroradiology, Am. J. Neuroradiol. 38(2): p. 218-229 (2017)
3. S. Power et al., Vessel wall magnetic resonance imaging in acute ischemic stroke: effects of embolism and mechanical thrombectomy on the arterial wall, Stroke 45(8): p. 2330-2334 (2014)
4. W. K. Seo et al., Clinical Significance of Wall Changes After Recanalization Therapy in Acute Stroke: High-Resolution Vessel Wall Imaging, Stroke 48(4): p. 1077-1080 (2017)
5. A. G. van der Kolk et al., Intracranial vessel wall imaging at 7.0-T MRI, Stroke
42(9): p. 2478-84 (2011)
6. A. G. Van Der Kolk et al., Multi-sequence whole-brain intracranial vessel wall imaging at 7.0 tesla, Eur. J. Radiol. 23(11): p. 2996-3004 (2013)
7. M. Andersen et al., A Generalized Prospective Motion Correction Framework for Improved Spectroscopy, Structural and Angiographic Imaging, Annual Meeting of the ISMRM, Honolulu, HI, USA, abstract 3934 (2017)
8. V. Boer et al., High resolution imaging at 7T using interleaved prospective motion correction (iMOCO), Annual Meeting of the ISMRM, Paris, France, abstract 1307 (2018)
Figures
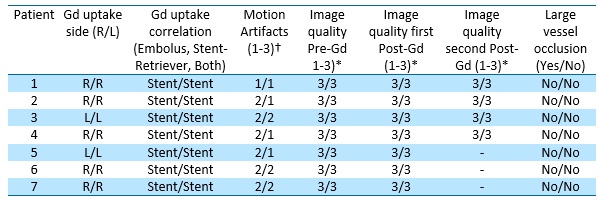
✝: Level of Motion Artifacts: 1=None, 2=Visible But Not affecting Image Quality, 3=Impairing Image Quality
*: Overall Image Quality: 1=Non-Diagnostic, 2= Acceptable, 3=Excellent