2789
Contributions of cardiovascular risk and smoking to chronic obstructive pulmonary disease (COPD)-related changes in brain structure and function1Institute for Molecular and Clinical Sciences, St George's University of London, London, United Kingdom, 2Institute for Infection and Immunity, St George's University of London, London, United Kingdom, 3Clinical Research and Imaging Centre, University of Bristol, Bristol, United Kingdom, 4Academic Respiratory Unit, School of Clinical Sciences, University of Bristol, Bristol, United Kingdom
Synopsis
Structural and functional brain abnormalities have been reported in chronic obstructive pulmonary disease (COPD), however, it is unclear whether these occur independently of cardiovascular risk. Neuroimaging and clinical markers of brain structure and function were compared between 27 COPD patients and 23 age-matched non-COPD smoker controls. Clinical relationships and group interactions with brain structure were tested. COPD patients showed a specific pattern of structural (lower grey matter volume) and functional (lower cognitive function and psychological status) brain abnormalities that could not be explained by cardiovascular risk. Lower lung function and psychological ill-health were associated with markers of white matter damage.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disease characterised by persistent, typically progressive, airflow limitation and lung inflammation which is commonly due to cigarette smoking.1 It is also associated with extra-pulmonary manifestations including cardiovascular disease and cognitive impairment.2-4 However, the disease presentation is highly heterogeneous and it is unclear whether these co-morbidities are pathogenically linked to the disease process or reflect the co-existence of a number of age-related risk factors and conditions.5 Previous neuroimaging findings indicate that COPD and reduced lung function are associated with structural and functional brain changes 6-17 consistent with cerebral small vessel disease (SVD).18 However, the majority of these studies failed to control for differences in cardiovascular risk and smoking history - factors known to accelerate SVD.19 This study was designed to test whether neuroimaging findings in COPD can be attributed to cardiovascular risk factors and smoking.Methods
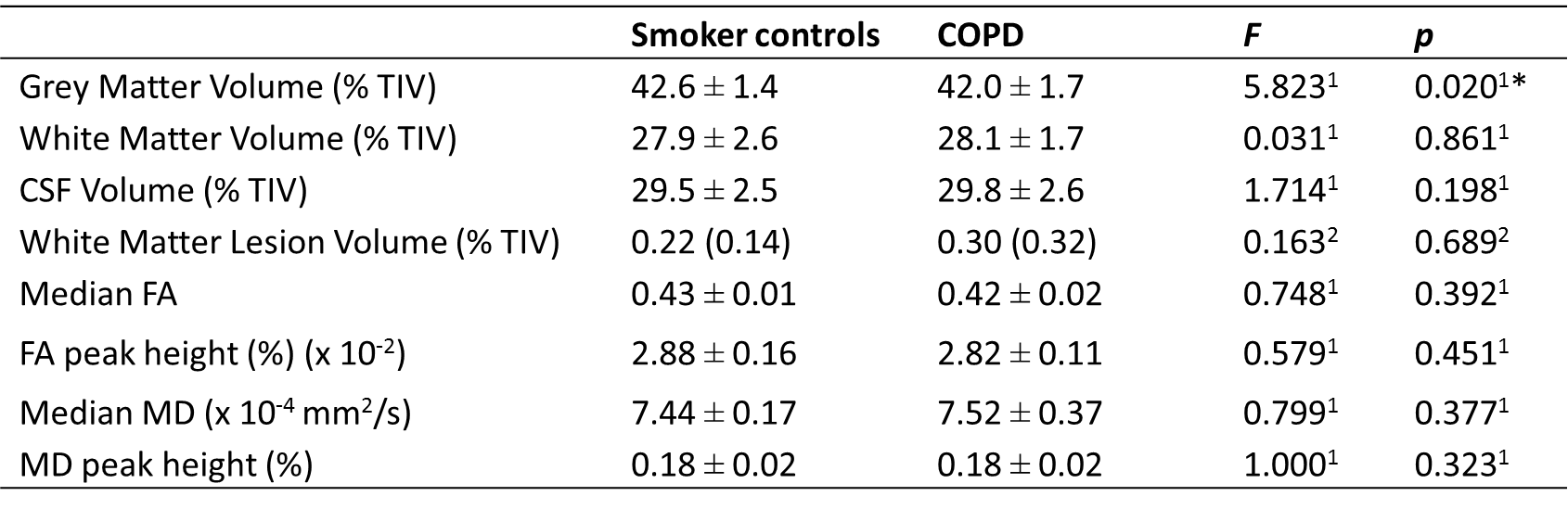
27 stable COPD patients (age: 63.0 ± 9.1 years, 59.3% male, FEV1: 58.1 ± 18.0 % pred.) and 23 non-COPD controls with a history of smoking (age: 66.6 ± 7.5 years, 52.2% male, FEV1: 100.6 ± 19.1 % pred.) were recruited. Clinical measures of disease severity, cardiovascular risk, central arterial stiffness (aortic pulse wave velocity), psychological status (Hospital Anxiety and Depression Scale - HADS) and cognitive function (Montreal Cognitive Assessment Test – MoCA) were obtained. T1-weighted, Fluid Attenuated Inversion Recovery and Diffusion Tensor Imaging sequences were acquired using a 3T magnetic resonance imaging (MRI) system, providing measures of brain macrostructure (grey matter, white matter, cerebrospinal fluid and white matter hyperintensity (WMH) volumes normalised for intracranial volume) and white matter microstructure (normalised histograms of fractional anisotropy (FA) and mean diffusivity (MD) values). Between-group differences in clinical measures and brain structure were tested using analyses of covariance. Relationships between clinical measures and brain structure and whether these relationships differed between COPD and smoker controls were tested using multiple linear regression. All models controlled for the following demographic and cardiovascular risk factors: age, sex, smoking status, pack years smoked, mean arterial pressure and aortic pulse wave velocity.Results
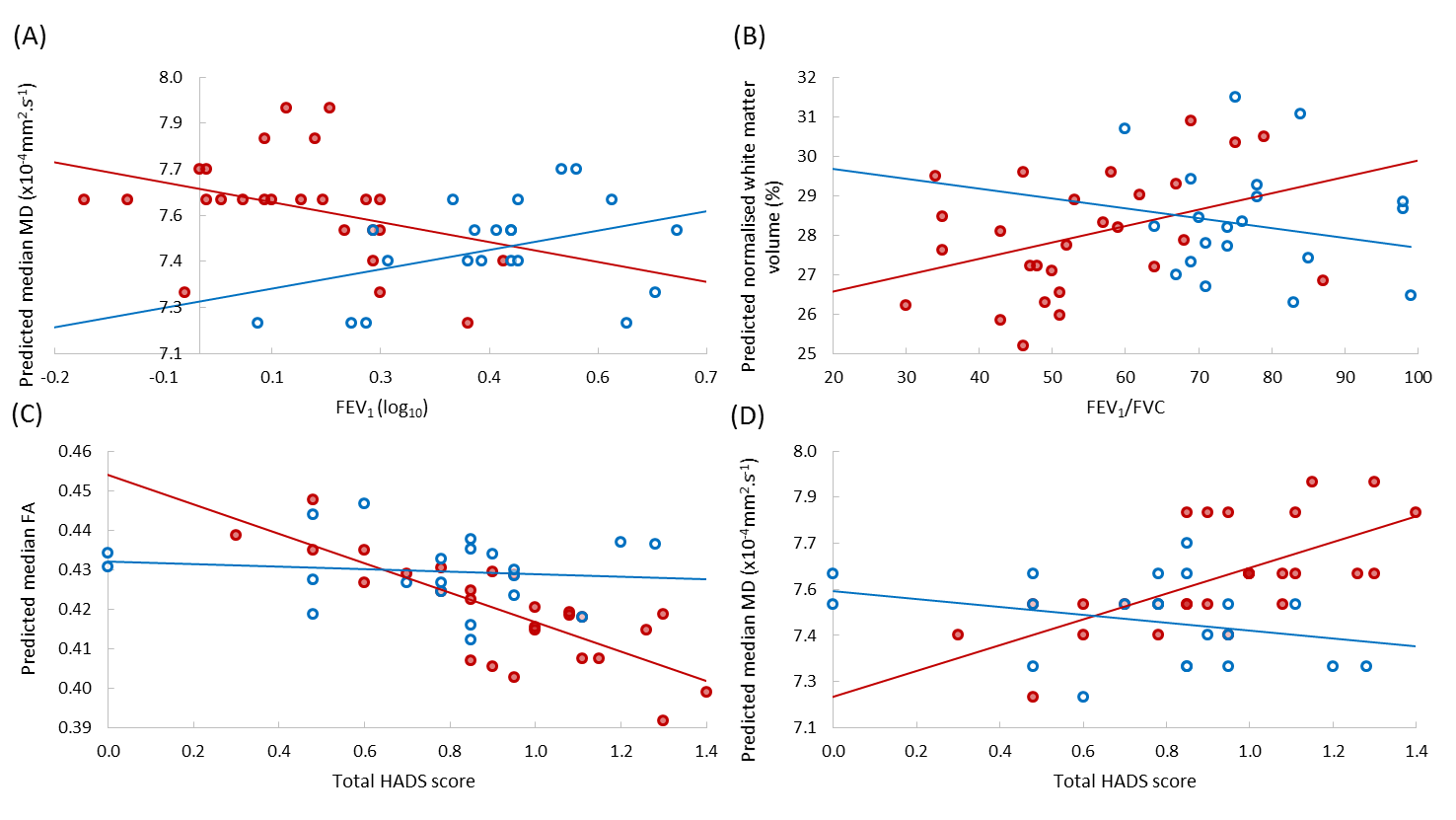
COPD patients had significantly lower MoCA (p=0.011) and normalised grey matter volume (p=0.020), and significantly higher HADS depression score (p=0.016) (see Figure 1). In COPD patients, higher total HADS score was associated with white matter microstructural measures (lower median FA: p<0.001, higher median MD: p<0.001 and lower MD peak height: p<0.001) (see Figure 2). Reduced lung function (FEV1/FVC and FEV1) was associated with lower normalised white matter volume (p=0.047) and abnormal white matter microstructure (higher median MD: p=0.028) (see Figure 2). These results were independent of cardiovascular risk factors.Discussion
This study provided a cross-sectional investigation of differences in brain structure and function (cognitive function and psychological status) between COPD patients and non-COPD smoker controls whilst controlling for demographic and cardiovascular risk factors. Additionally, clinical relationships and group interactions with brain structure were tested to determine whether the same neuropathological processes are active in both COPD and non-COPD smokers. Previous cross-sectional MRI studies have reported greater severity of SVD markers in COPD compared to controls.6-8,10,13 Those results could not be replicated in this study suggesting that they were driven by group-differences in smoking history and cardiovascular risk. However, this study found that COPD patients had lower normalised grey matter volume, cognitive function and psychological status, and associations between reduced lung function and increased white matter damage that were independent of cardiovascular risk factors. This suggests that additional neuropathological processes are occurring in COPD. The relationship between worse psychological status and markers of white matter microstructure found in this study are consistent with results from the ageing and SVD literature 20-22 and suggest that anxiety and depression may have a structural basis in COPD.Conclusions
COPD is associated with a specific pattern of structural and functional brain abnormalities that cannot be explained by measures of cardiovascular risk, central arterial stiffness or smoking history alone. In COPD, worse lung function was associated with deterioration in white matter macro- and microstructure, and lower psychological status with deterioration in white matter microstructure. This suggests that the brain changes in COPD do not exclusively result from increased cardiovascular risk and smoking. COPD-related anxiety and depression may occur secondary to white matter damage. These findings have important implications for the prevention and management of neuropsychiatric co-morbidities in COPD.Acknowledgements
No acknowledgement found.References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017;195:557–582 doi: 10.1164/rccm.201701-0218PP.
2. Corsonello A, Antonelli Incalzi R, Pistelli R, Pedone C, Bustacchini S, Lattanzio F. Comorbidities of chronic obstructive pulmonary disease. Curr. Opin. Pulm. Med. 2011;17 Suppl 1:S21–28 doi: 10.1097/01.mcp.0000410744.75216.d0.
3. Laforest L, Roche N, Devouassoux G, et al. Frequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: A population-based cohort study. Respir. Med. 2016;117:33–39 doi: 10.1016/j.rmed.2016.05.019.
4. Dodd JW, Getov SV, Jones PW. Cognitive function in COPD. Eur. Respir. J. 2010;35:913–922 doi: 10.1183/09031936.00125109.
5. Miller J, Edwards LD, Agustí A, et al. Comorbidity, systemic inflammation and outcomes in the ECLIPSE cohort. Respir. Med. 2013;107:1376–1384 doi: 10.1016/j.rmed.2013.05.001.
6. Dodd JW, Chung AW, van den Broek MD, Barrick TR, Charlton RA, Jones PW. Brain Structure and Function in Chronic Obstructive Pulmonary Disease: A Multimodal Cranial Magnetic Resonance Imaging Study. Am. J. Respir. Crit. Care Med. 2012;186:240–245 doi: 10.1164/rccm.201202-0355OC.
7. van Dijk EJ. Arterial oxygen saturation, COPD, and cerebral small vessel disease. J. Neurol. Neurosurg. Psychiatry 2004;75:733–736 doi: 10.1136/jnnp.2003.022012.
8. Lahousse L, Vernooij MW, Darweesh SKL, et al. Chronic obstructive pulmonary disease and cerebral microbleeds. The Rotterdam study. Am. J. Respir. Crit. Care Med. 2013;188:783–788 doi: 10.1164/rccm.201303-0455OC.
9. Li J, Fei G-H. The unique alterations of hippocampus and cognitive impairment in chronic obstructive pulmonary disease. Respir. Res. 2013;14:1–9.
10. Zhang H, Wang X, Lin J, et al. Grey and white matter abnormalities in chronic obstructive pulmonary disease: a case-control study. BMJ Open 2012;2:e000844–e000844 doi: 10.1136/bmjopen-2012-000844.
11. Esser RW, Stoeckel MC, Kirsten A, et al. Structural Brain Changes in Patients With COPD. Chest 2016;149:426–434 doi: 10.1378/chest.15-0027.
12. Wang C, Ding Y, Shen B, et al. Altered Gray Matter Volume in Stable Chronic Obstructive Pulmonary Disease with Subclinical Cognitive Impairment: an Exploratory Study. Neurotox. Res. 2017;31:453–463 doi: 10.1007/s12640-016-9690-9.
13. Spilling CA, Jones PW, Dodd JW, Barrick TR. White matter lesions characterise brain involvement in moderate to severe chronic obstructive pulmonary disease, but cerebral atrophy does not. BMC Pulm. Med. 2017;17 doi: 10.1186/s12890-017-0435-1.
14. Liao D, Higgins M, Bryan NR, et al. Lower pulmonary function and cerebral subclinical abnormalities detected by MRI: the Atherosclerosis Risk in Communities study. Chest 1999;116:150–156.
15. Taki Y, Kinomura S, Ebihara S, et al. Correlation between pulmonary function and brain volume in healthy elderly subjects. Neuroradiology 2013;55:689–695 doi: 10.1007/s00234-013-1157-6.
16. Sachdev PS, Anstey KJ, Parslow RA, et al. Pulmonary Function, Cognitive Impairment and Brain Atrophy in a Middle-Aged Community Sample. Dement. Geriatr. Cogn. Disord. 2006;21:300–308 doi: 10.1159/000091438.
17. Murray AD, Staff RT, Shenkin SD, Deary IJ, Starr JM, Whalley LJ. Brain white matter hyperintensities: relative importance of vascular risk factors in nondemented elderly people. Radiology 2005;237:251–257 doi: 10.1148/radiol.2371041496.
18. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12:822–838 doi: 10.1016/S1474-4422(13)70124-8.
19. Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010;9:689–701 doi: 10.1016/S1474-4422(10)70104-6.
20. Alexopoulos GS, Kiosses DN, Choi SJ, Murphy CF, Lim KO. Frontal white matter microstructure and treatment response of late-life depression: a preliminary study. Am. J. Psychiatry 2002;159:1929–1932 doi: 10.1176/appi.ajp.159.11.1929.
21. Teodorczuk A, Firbank MJ, Pantoni L, et al. Relationship between baseline white-matter changes and development of late-life depressive symptoms: 3-year results from the LADIS study. Psychol. Med. 2010;40:603–610 doi: 10.1017/S0033291709990857.
22. Emsell L, Adamson C, De Winter F-L, et al. Corpus callosum macro and microstructure in late-life depression. J. Affect. Disord. 2017;222:63–70 doi: 10.1016/j.jad.2017.06.063.
Figures