2786
Associations Between Dual Task Cost and Striatal Functional Connectivity in Parkinson’s Disease with Mild Cognitive Impairment1Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, United States, 2University of California, San Diego, La Jolla, CA, United States, 3Stanford University, Stanford, CA, United States
Synopsis
This study investigated striatal functional connectivity correlates of dual-tasking in Parkinson’s disease with and without mild cognitive impairment using resting state fMRI. Increased caudate functional connectivity with frontotemporal, insular and subcortical regions were associated with increased dual task cost in Parkinson’s disease with mild cognitive impairment, whereas correlations were only seen in increased putamen and supplementary motor area functional connectivity and increased dual task cost in PD participants. These results reveal that dual tasking is associated with different striatal functional connectivity patterns in PD participants, with and without, cognitive impairment suggesting compensatory mechanisms in Parkinson’s disease with mild cognitive impairment.
Introduction
Attention and executive functions play a key role in gait in Parkinson’s disease (PD) 1. Gait impairment in PD differs between patients with and without mild cognitive impairment (MCI). In particular, gait parameters with high sensitivity to dual task were shown to be associated with PD-MCI 2. In PD, while striatal activity was observed during dual tasking, no striatal activity was observed during cognitive or motor tasks 3. This region was also not recruited by healthy controls during dual tasking. Therefore, we aimed to investigate the neural correlates of dual tasking in PD-MCI and PD with normal cognition (PD-NC) focusing on striatal functional connectivity (FC) as different FC patterns may be associated with dual tasking in PD-MCI due to cognitive deficits.Methods
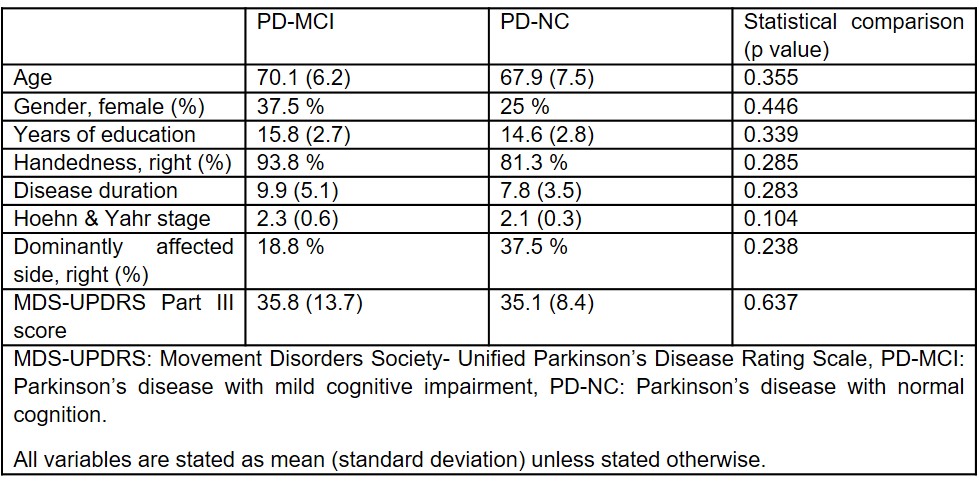
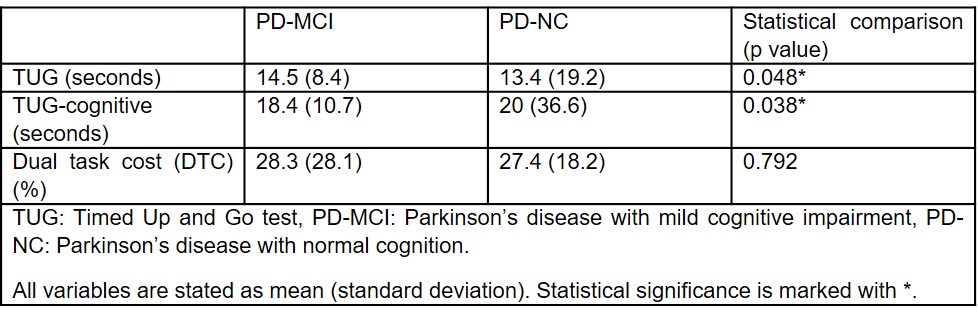
Sixteen PD-MCI 4 and 16 PD-NC from the Center for Neurodegeneration and Translational Neuroscience at Cleveland Clinic Lou Ruvo Center for Brain Health were included. To eliminate the medication effect, all testing and scanning were performed during levodopa off (>12 hours after the last levodopa dose). Demographics and disease parameters are shown in Table 1. Dual Task Timed Up and GO (TUG) was used to assess dual task interference. For the single task condition (TUG), participants are required to stand up from a chair, walk three meters, turn, walk back and sit down. In the dual task condition (TUG-cognitive), participants are required to complete the same test while counting backwards by threes from a randomly selected number. The outcome measure is the time a participant takes to perform each test. Dual task cost (DTC) (%) was calculated to normalize for single task performance as: (dual task – single task)/single task *100 5. Increased DTC is indicated with a higher percentage. All participants underwent resting state functional magnetic resonance imaging with a 3 T scanner. After standard preprocessing, mean time series were obtained from 38 regions-of-interest (ROIs) likely to be involved in dual tasking based on Vervoort et al. 6. The subcortical ROIs were; putamen, caudate, substantia nigra pars compacta, subthalamic nucleus, globus pallidus, thalamus and pedunculopontine nucleus. The cortical ROIs were; primary motor cortex, premotor cortex, supplementary motor area, presupplementary motor area, dorsolateral prefrontal cortex, medial frontal gyrus, inferior parietal lobule, superior temporal gyrus, precuneus, posterior cingulate, anterior cingulate and insula. The connectivity between two ROIs was estimated using Pearson’s correlation between their averaged time-series, and subsequently a connectivity matrix (38 x 38) was obtained for each subject. Two groups were compared for TUG performances and DTC using Mann Whitney U test. Correlation analyses between striatal FC values and DTC were computed separately for each group using Spearman’s correlation.Results
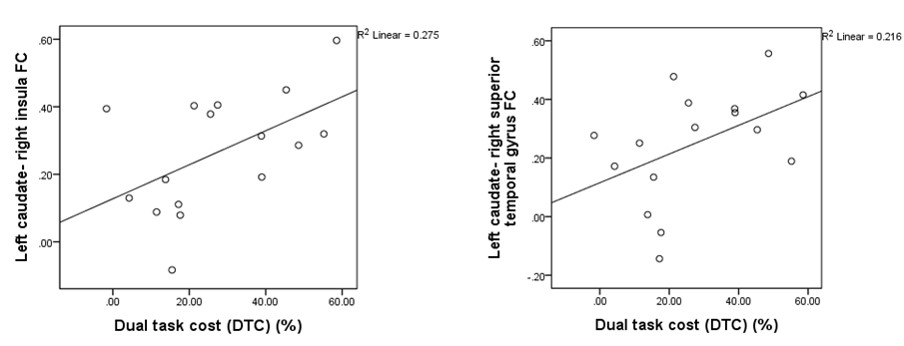
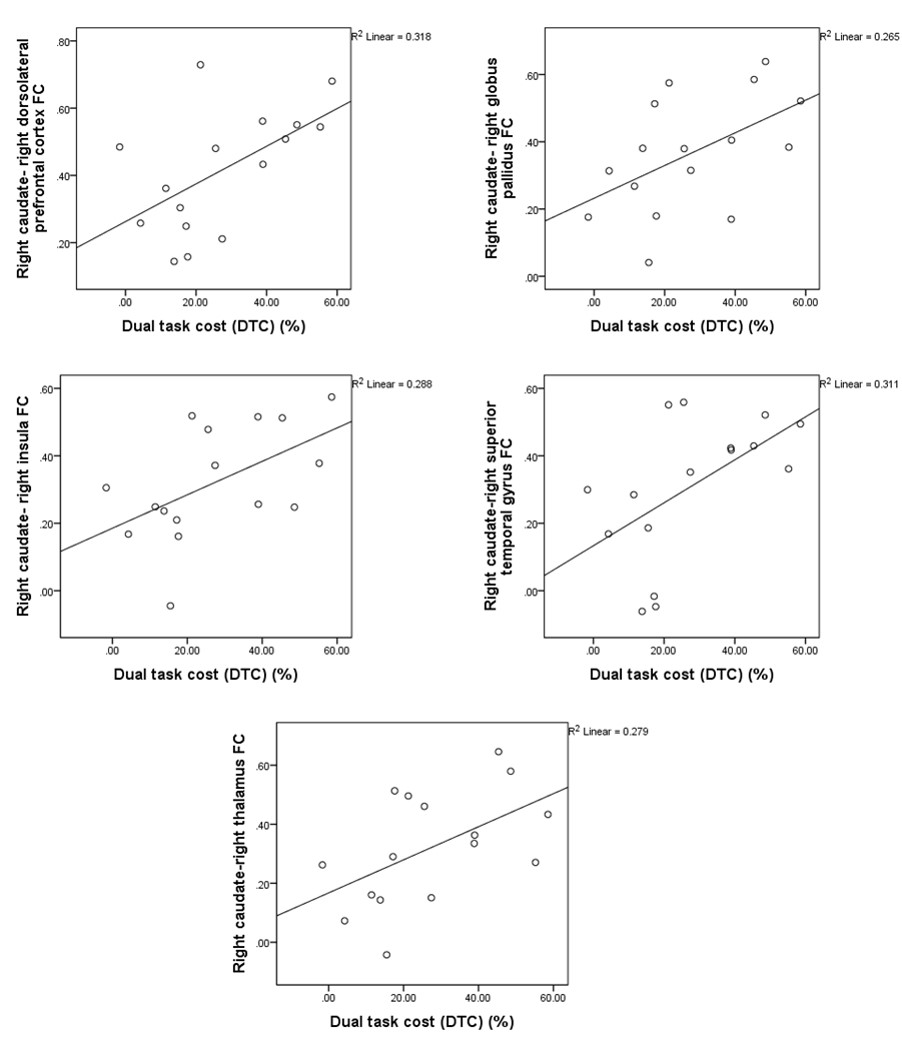
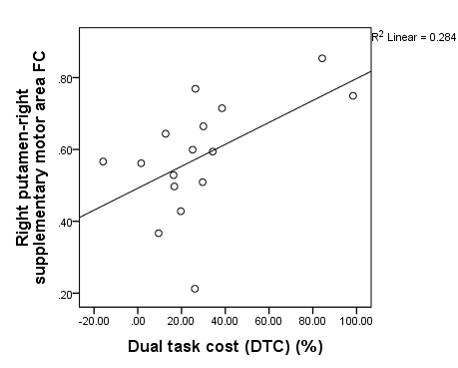
Age, gender, years of education, disease severity assessed by Hoehn and Yahr stage, and motor impairment assessed by Movement Disorders Society- Unified Parkinson’s Disease Rating Scale Part III did not differ between groups (Table 1). TUG and TUG-cognitive performances were different between groups, with no significant DTC difference (Table 2). The PD-MCI group was significantly slower than PD-NC during both TUG and TUG-cognitive tasks. For the PD-MCI, DTC was positively correlated with FC between left caudate-right insula (r=.532, p=0.034) and right superior temporal gyrus (r=.562, p=.024) (Figure 1); right caudate- right dorsolateral prefrontal cortex (r=.562, p=.024), right globus pallidus (r=.588, p=.017), right insula (r=.574, p=.020), right superior temporal gyrus (r=.641, p=.007), right thalamus (r=.594, p=.015) (Figure 2). For the PD-NC, DTC was positively correlated with only right putamen and right supplementary motor area FC (r=.565, p=.023) (Figure 3).Discussion
Our results revealed that performance on dual tasking, incorporating both gait and cognitive performance, correlates with different striatal FC patterns in PD-MCI. Higher DTC was associated with increases in different striatal connections in these two groups. In PD-MCI, DTC was associated with caudate FC with frontotemporal, insular and subcortical regions; whereas in PD-NC the only correlation between DTC and FC was seen in putamen and supplementary motor area. Different correlates within these two groups point to compensatory mechanisms in PD-MCI, as DTC between the groups were not different. As significant correlations were scarce, dual-tasking is likely associated with other regions in addition to striatum.Conclusion
Striatal FC correlates of dual-tasking are different between PD-MCI and PD-NC. As underlying mechanisms differ, these two groups may respond differently to therapies targeting gait impairment and cognition. Future studies should determine the effects of common therapies on dual-tasking in PD-MCI and PD-NC. On the other hand, future studies investigating associations between connectivity of other cortical and subcortical regions not included in our study can help elucidate the neural correlates of dual-tasking in PD-MCI.Acknowledgements
This work was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number 5P20GM109025, and private grant funds from Peter and Angela Dal Pezzo.References
- Yogev G, Giladi N, Peretz C, Springer S, Simon ES, Hausdorff JM. Dual tasking, gait rhythmicity, and Parkinson’s disease: Which aspects of gait are attention demanding? Eur J Neurosci. 2005. doi:10.1111/j.1460-9568.2005.04298.x.
- Amboni M, Barone P, Iuppariello L, et al. Gait Patterns in Parkinsonian Patients With or Without Mild Cognitive Impairment. doi:10.1002/mds.25165.
- Nieuwhof F, Bloem BR, Reelick MF, et al. Impaired dual tasking in Parkinson’s disease is associated with reduced focusing of cortico-striatal activity. Brain. 2017;140(5):1384-1398. doi:10.1093/brain/awx042.
- Litvan I, Goldman JG, Tröster AI, et al. Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force guidelines. Mov Disord. 2012;27(3):349-356. doi:10.1002/mds.24893.
- McDowd JM. The effects of age and extended practice on divided attention performance. J Gerontol. 1986;41(6):764-769. http://www.ncbi.nlm.nih.gov/pubmed/3772053. Accessed November 4, 2018.
- Vervoort G, Leunissen I, Firbank M, et al. Structural brain alterations in motor subtypes of Parkinson’s disease: Evidence from probabilistic tractography and shape analysis. PLoS One. 2016;11(6). doi:10.1371/journal.pone.0157743.
Figures