2782
Diffusion Tensor Imaging of the Superior Thalamic Radiation and Cerebrospinal Fluid Distribution in Idiopathic Normal Pressure Hydrocephalus1Diagnostic and Interventional Imaging, UThealth, McGovern Medical School, Houston, TX, United States, 2Neurology, UThealth, McGovern Medical School, Houston, TX, United States, 3UThealth, McGovern Medical School, Houston, TX, United States, 4Psychiatry, UThealth, McGovern Medical School, Houston, TX, United States
Synopsis
Ventricular
enlargement in elderly raises a challenging differential diagnosis to
physicians. While Alzheimer`s disease is the most common form of dementia,
idiopathic Normal Pressure Hydrocephalus (iNPH) constitutes a potentially
reversible syndrome. iNPH has a unique
pathophysiology pertaining to cerebrospinal fluid dynamics and periventricular
white matter. We aimed to determine the effects of iNPH on periventricular
white matter bundles and to further characterize its ventricular and sulcal CSF
distribution by using diffusion tensor tractography (DTT) and cerebrospinal
fluid (CSF) volumetrics on high resolution T1-weighted MRI data.
Background, Introduction and Purpose
Ventriculomegaly is a challenging neuroimaging finding neurologists frequently face in the aging population.1 Hydrocephalus is a general term that indicates accumulation of cerebrospinal fluid (CSF) in the ventricular system due to imbalance in the production, drainage, or reabsorption of CSF resulting in dilation of the cerebral ventricles.2 Idiopathic Normal Pressure Hydrocephalus (iNPH) is a form of chronic communicating hydrocephalus that results in a treatable syndrome characterized by the triad of gait impairment, progressive dementia, and urinary incontinence.3,4 iNPH prevalence is estimated to be 21.9/100,000 and increases with age, with an incidence of approximately 5.5/100,000 per year.5 Magnetic resonance imaging (MRI) especially diffusion tensor imaging (DTI) have shown to offer a useful in vivo surrogate biomarkers of white matter changes in Alzheimer’s disease,6,7 ventriculomegaly,8 and iNPH.9,10 Previous studies using deterministic and probabilistic DTI techniques revealed various profiles of DTI changes in different regions of the periventricular white matter when compared to normal and disease controls.9,10 A consensus is still not established for the most sensitive and specific DTI measurements in distinguishing ventriculomegaly in iNPH from other neurodegenerative diseases. Neuroimaging non-invasive markers for iNPH are a critical need, we propose a new technique to differentiate NPH from healthy and disease controls using novel MRI-DTI targets. In this study, we provide quantitative DTI mapping of main white matter pathways neighboring the lateral ventricular system. We analyzed the effect of iNPH on the superior thalamic radiation (STR) as it courses adjacent to the lateral wall of the lateral ventricle. The cortico-spinal tract (CST) and the dentato-rubro thalamic tract (DRTT) were also traced.11 Moreover, we investigated the volumetric changes of the ventricular and sulcal CSF in AD, iNPH, and healthy-aging subjects across lifespan.Methods
MRI whole brain anatomical isotropic 1mm T1-weighted and ~2mm isotropic, b=0, 1000 s/(mm*mm) diffusion weighted imaging (DWI) data were acquired on three age-matched cohorts: 9 (5F) iNPH (Philips 3T), 13 (7F) AD patients from the ADNI open access Siemens 3T data base (www.adni-info.org) and 20 (11F) healthy controls were selected from the Nathan Kline Institute Siemens 3T data (http://fcon_1000.projects.nitrc.org/indi/pro/nki.html). These twenty NKI subjects were the elderly subset (62-85 years) of 138 that were processed to obtain DTI and volumetric measures across the lifespan (57 males and 81 males, age range 5-85 years). DWI preprocessing, decoding, tensor diagonalization and deterministic tractography were done in DTIstudio (http://cmrm.med.jhmi.edu).12 Validated volumetric segmentation and tissue parcellation were performed using MRIcloud (https://braingps.mricloud.org). The superior thalamic radiation, corticospinal tract and dentato-rubro-thalamic tract were traced and quantified.13,14 Ventricular and sulcal CSF volumes in the three groups were shown and compared.Results
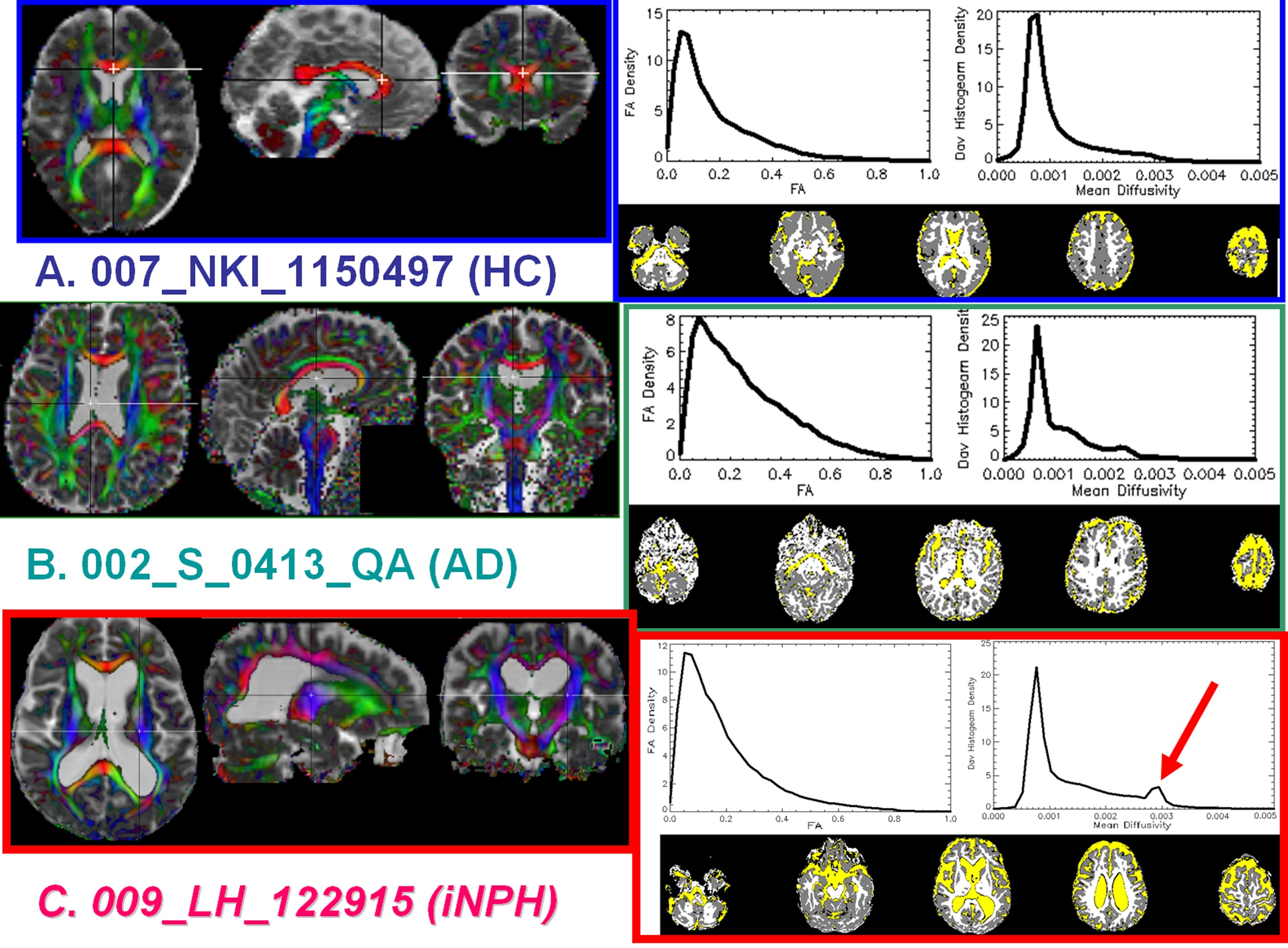
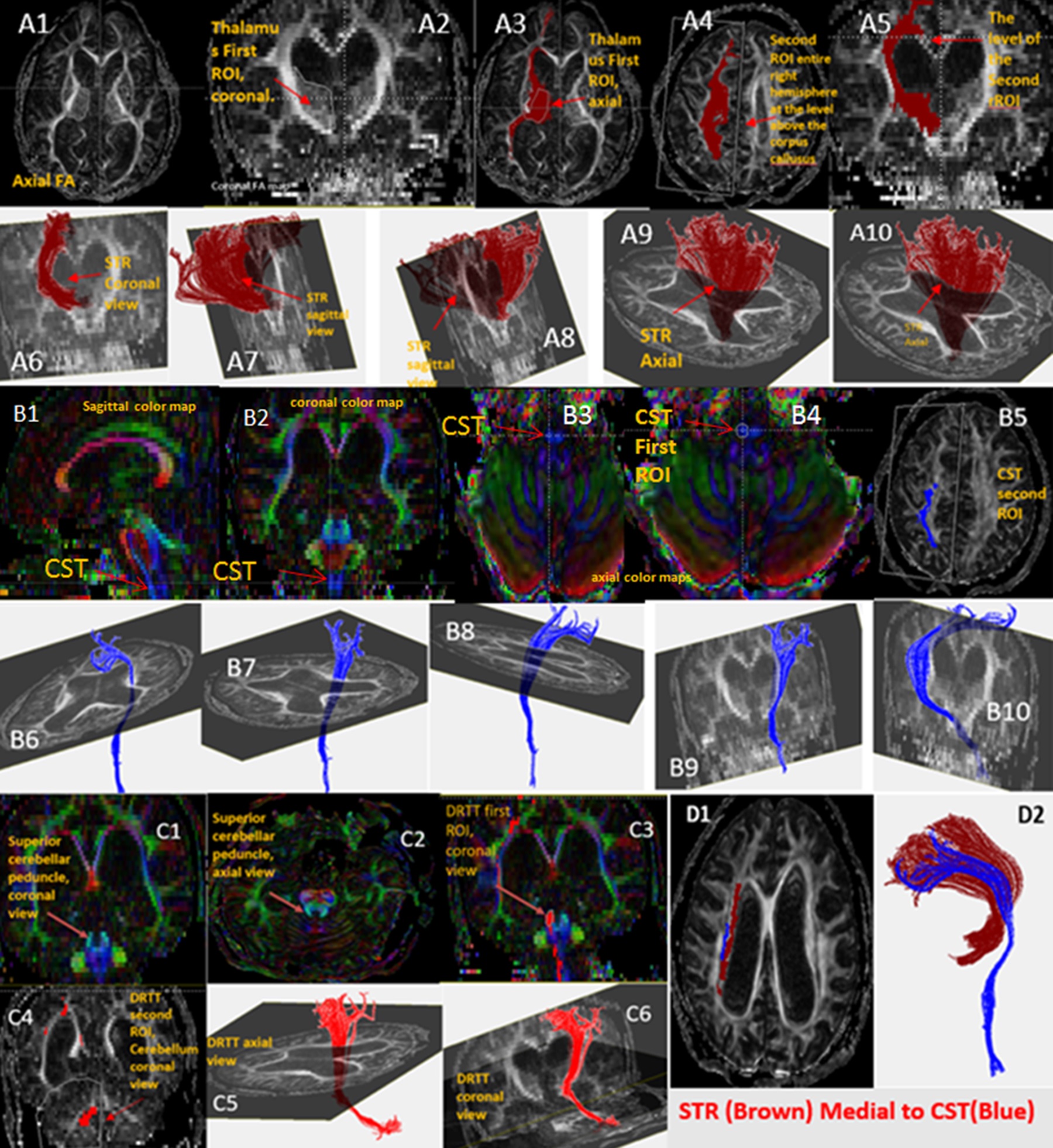
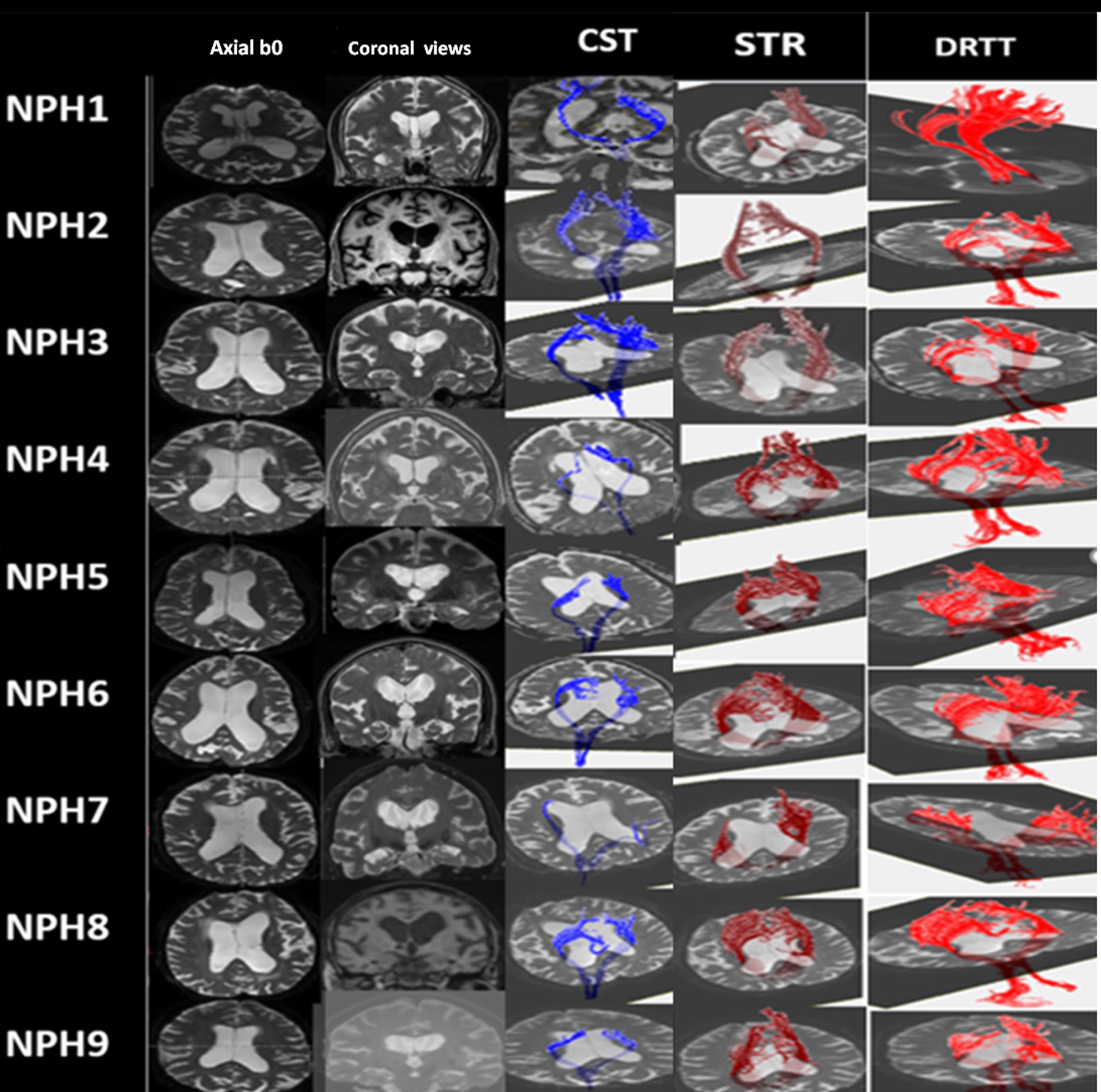
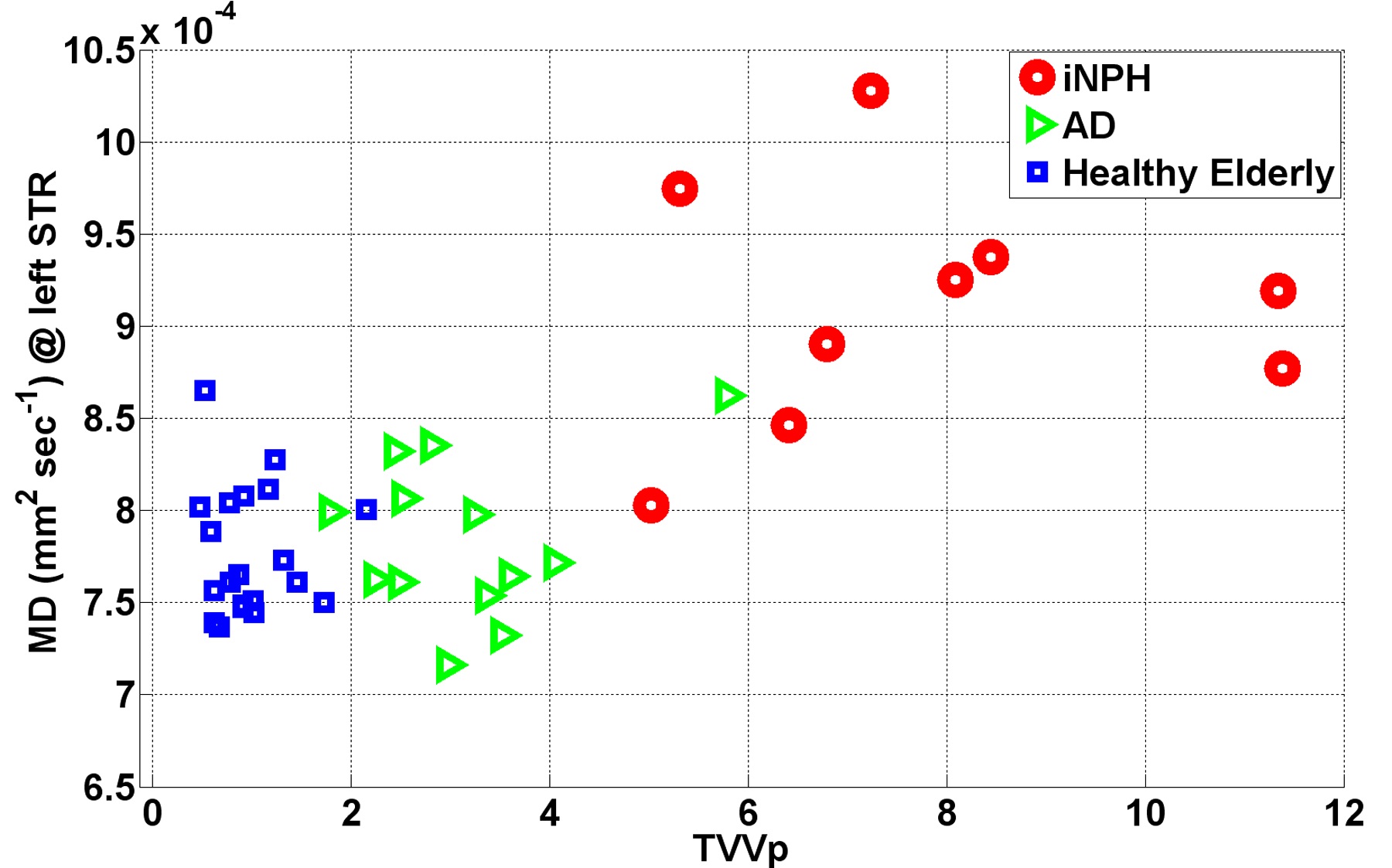
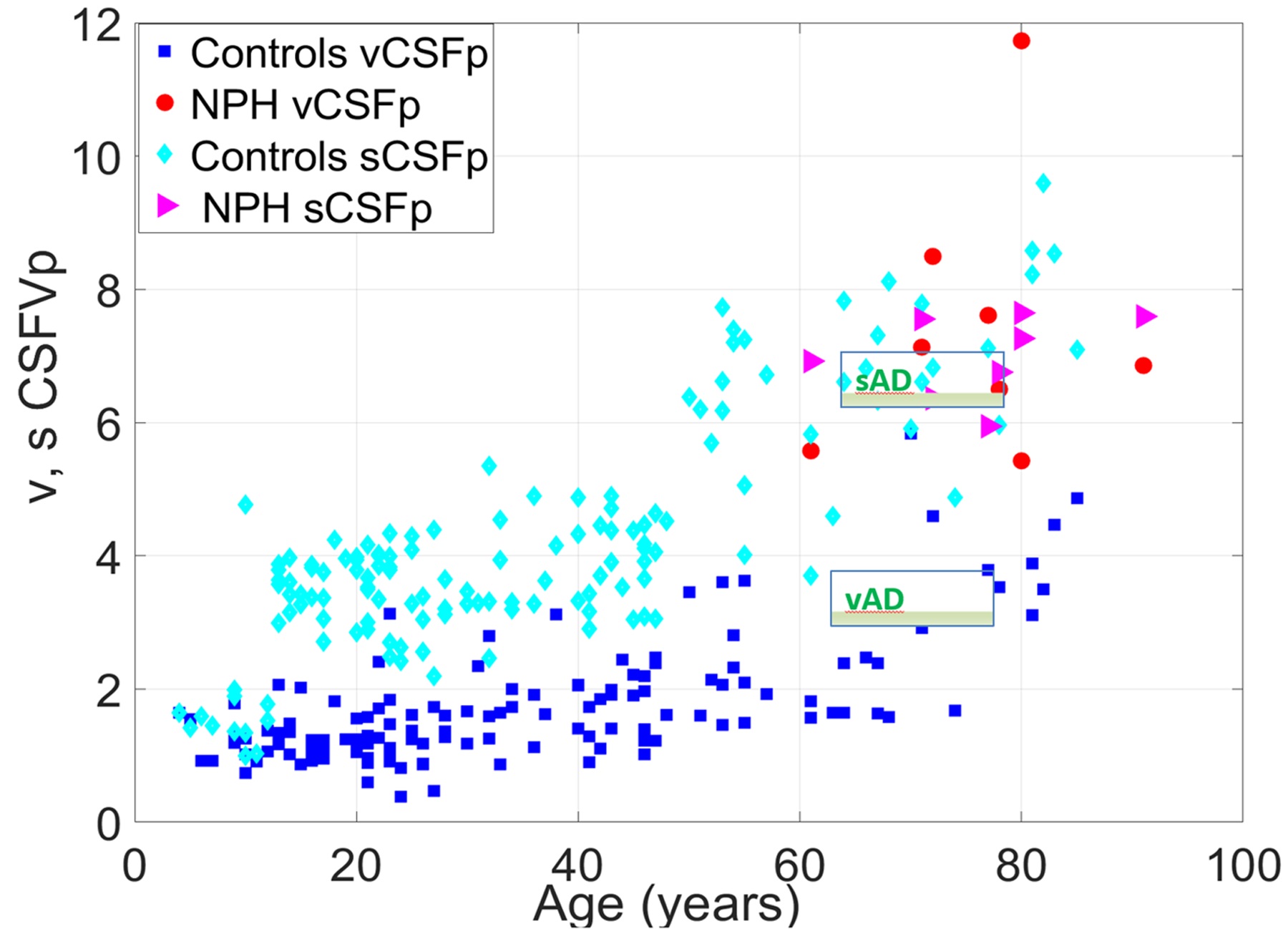
Data quality was deemed acceptable and allowed DTI-based tissue segmentation 15,16,17 on all subjects (Figure 1). The CST and STR are illustrated in Figure 2. Figure 3 shows the CST, STR and DRTT on all iNPH patients. Total ventricular–to-intracranial volume brain percentage is shown vs. the average of left STR mean diffusivity in Figure 4. Figure 5 shows the ventricular and sulcal CSF to intracranial volume percentage as age advances utilizing the entire lifespan cohort. Combining increased mean diffusivity of the superior thalamic radiation with ventricular volume resulted in clear separation of iNPH from the AD and age-matched healthy subject groups. Additionally, ventricular-to-sulcal CSF ratio, utilizing fully automated methods, was significantly greater in the iNPH patients compared to AD and healthy age-matched controls.Discussion
Our study demonstrates the feasibility and utility of deterministic fiber tractography analysis of the periventricular white matter disease in iNPH. The STR forms the most medial part of the superior corona radiata and runs medial to the corticospinal tract.13 We hypothesized that the STR will be affected by iNPH ventriculomegaly given its anatomical proximity to and its pattern of spread around the lateral ventricle wall (Fig. 2). By combining these two measures we demonstrate the feasibility of differentiating the groups of interest based on two-dimensional vector representation of pathology (Fig. 4). Combining both the ventricular volume and superior thalamic radiation mean diffusivity led to group separation of iNPH, AD and healthy elderly. Further details and limitations of our work and plans to extend the work are described elsewhere.18Acknowledgements
DUNN Research Foundation, NIH and the Alzheimer's Disease Neuroimaging Initiative Researchers.References
1. Staffaroni A, Elahi FM, McDermott D, et al. Neuroimaging in dementia. Semin Neurol 2017;37:510-37.
2. Mori E, Ishikawa M, Kato T, et al. Guidelines for management of idiopathic normal pressure hydrocephalus: second edition. Neurol Med Chir 2012;52:775–809.
3. Hakim S, Adams RD. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure observations on cerebrospinal fluid hydrodynamics. J Neurol Sci 1965;2:307–27.
4. Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus: INPH Guidelines, part II. Neurosurgery 2005;57:4-16.
5. Hashimoto M, Ishikawa M, Mori E, Kuwana N. Study of INPH on neurological improvement (SINPHONI). Diagnosis of idiopathic normal pressure hydrocephalus is supported by MRI-based scheme: a prospective cohort study. Cerebrospinal Fluid Res Dec 2010;7:18.
6. Acosta-Cabronero J and Nestor PJ. Diffusion tensor imaging in Alzheimer`s disease: insights into the limbic-diencephalic network and methodological considerations. Front Aging Neurosci 2014;6:266.
7. Nestor SM, Rupsingh R Borrie B, et al. Ventricular enlargement as a possible measure of Alzheimer’s disease progression validated using the Alzheimer’s disease neuroimaging initiative database. Brain 2008; 131:2443-54.
8. Osuka S, Matsuhita A, Yamamoto T, et al. Evaluation of ventriculomegaly using diffusion tensor imaging: correlation with chronic hydrocephalus and atrophy. J Neurosurg 2010;112:832-9.
9. Hoza D, Vlasák A, Hořínek D, et al. DTI-MRI biomarkers in the search for normal pressure hydrocephalus aetiology: a review. Neurosurg Rev 2015;38:239-44.
10. Siasios I, Kapsalaki EZ, Fountas KN, et al. The role of diffusion tensor imaging and fractional anisotropy in the evaluation of patients with idiopathic normal pressure hydrocephalus: a literature review. Neurosurg Focus 2016;41:12.
11. Haines DE. Neuroanatomy: An Atlas of Structures, Sections, and Systems 8th edition. Baltimore, MD: Williams & Wilkins; 2008:178-87.
12. Mori S, Wu D, Ceritoglu C, et al. MRICloud: delivering high-throughput MRI neuroinformatics as cloud-based software as a service. Comput Sci Engin 2016;18:21-35.
13. Wakana S, Caprihan A, Panzenboeck MM, et al. Reproducibility of quantitative tractography methods applied to cerebral white matter. Neuroimage 2007;36:630-44.
14. Keser Z, Hasan KM, Mwangi BI, et al. Diffusion tensor imaging of the human cerebellar pathways and their interplay with cerebral macrostructure. Front neuroanat 2015;9:1-13.
15. Hasan KM, Halphen C, Sankar A, et al. Diffusion tensor imaging-based tissue segmentation: validation and application to the developing child and adolescent brain. Neuroimage. 2007;34(4):1497-505.
16. Hasan KM. A framework for quality control and parameter optimization in diffusion tensor imaging: theoretical analysis and validation. Magn Reson Imaging. 2007;25(8):1196-202.
17. Hasan KM, Walimuni IS, Abid H, Hahn KR. A review of diffusion tensor magnetic resonance imaging computational methods and software tools. Comput Biol Med 2011;41:1062-72.
18. Younes K, Hasan KM, Kamali A, et al. Diffusion Tensor Imaging of the Superior Thalamic Radiation and Cerebrospinal Fluid Distribution in Idiopathic Normal Pressure Hydrocephalus. J of Neuroimaging 2019 (DOI: 10.1111/jon.12581).
Figures