2781
The Splenial Angle: A Novel Index in Idiopathic Normal Pressure Hydrocephalus1Diagnostic Radiology, Singapore General Hospital, Singapore, Singapore, 2Duke-NUS Medical School, Singapore, Singapore, 3Health Services Research Unit, Singapore General Hospital, Singapore, Singapore, 4Neuroradiology, National Neuroscience Institute, Singapore, Singapore, 5Neurosurgery, National Neuroscience Institute, Singapore, Singapore
Synopsis
The callosal angle (CA) is a useful tool in idiopathic normal pressure hydrocephalus (iNPH) for diagnosis and patient selection for shunt surgery. We evaluated for (1) differences in a novel splenial angle (SA) in iNPH compared to healthy controls (HC), and (2) temporal changes in SA, CA and Evan’s index in shunted and non-shunted iNPH patients. Significant differences (p<0.0001) existed in the EI, CA and SA between iNPH and HC. Amongst iNPH patients with or without shunting, significant temporal changes were also found in in all indices on follow-up MRI scans compared to baseline measurements.
Introduction
Idiopathic normal pressure hydrocephalus (iNPH) is characterized by the classic triad of gait apraxia, dementia, and urinary incontinence (1). The Evans' index (EI) is a gross marker of ventriculomegaly. The callosal angle (CA) is a useful tool in the diagnosis of iNPH and patient selection for shunt surgery (2). The CA is measured on coronal images through the posterior commissure, perpendicular to the antero-posterior commissural plane. Measurements of CA can be highly variable on slight right-left tilting of the coronal plane and also off-centering from the PC in untrained hands. We proposed a novel splenial angle (SA), measured on axial sections on the color FA map of a diffusion tensor MR image, which is easy to measure and train in. The objective of this study is to (1) evaluate the ease of training and reproducibility of SA measurements in a case control iNPH cohort, and compare (2) SA measurements with EI and CA in iNPH versus HC and (3) differences in SA, EI and CA measurements pre and post-shunting in iNPH.Methods
The institutional ethics committee approved this prospective study. Patients clinically diagnosed with iNPH were recruited based on key clinical and neuroimaging features and after confirmation with CSF lumbar tap tests over 3 consecutive days and neuropsycholoical testing, as well as exclusion of secondary causes. All patients, with or without ventricular shunting, underwent brain MRI on a 3T scanner at baseline, 6-month and 1-year follow-up. Age-matched healthy controls (HC) were also recruited for brain MRI. The MR protocol included the following sequences: axial FLAIR, DTI (TR/TE/FA 10025/97/90; 22x22cm FOV; 128x128 matrix; 2mm slices) and 3D sagittal MPRAGE (TR/TE/TI/FA 1900/2.48/900/9; 23x18.7cm FOV; 256x253 matrix; 0.9mm slices) & SPACE (TR/TE/FA 1000/131/120; 16x16cm FOV; 320x317 matrix; 0.5mm slices).
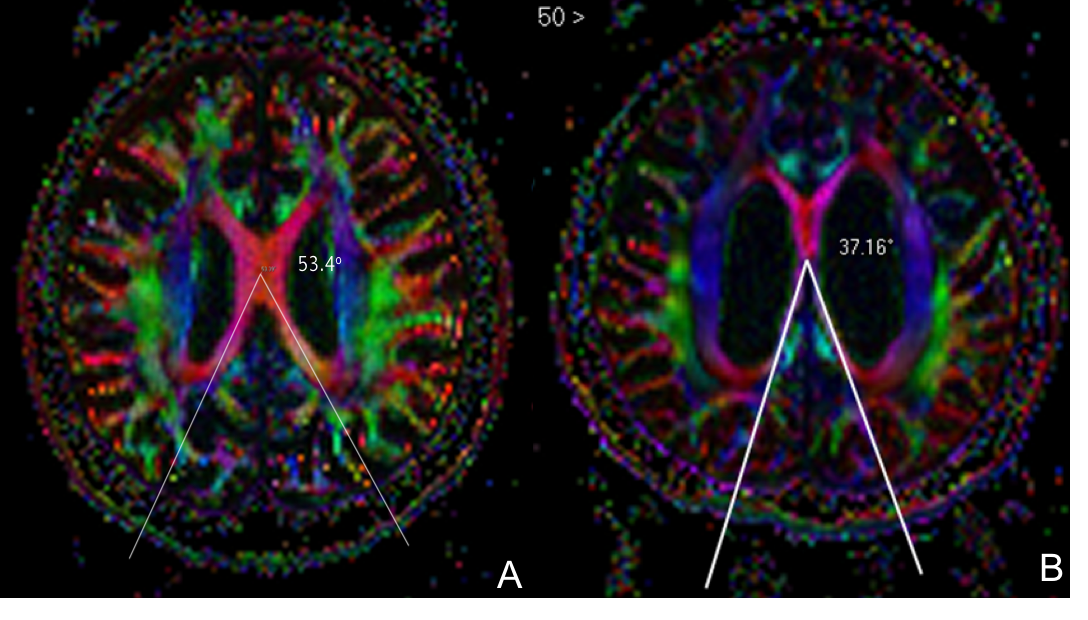
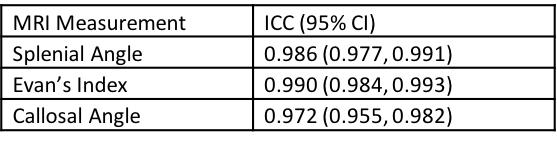
EI, CA and SA measurements were made by 2 independent raters: a neuroradiologist with more than 20 years of experience and a research assistant after 1 month of intensive training in handling 3D MPR images. The EI was measured on the axial FLAIR images. The CA was measured on the reconstructed coronal images through the posterior commissure, perpendicular to the antero-posterior commissural plane as determined on the sagittal view. The novel SA is an angular measurement of the angle subtended by the red fibers of the forceps major centered at the callosal body and measured on axial sections on the color FA map of a diffusion tensor MR image, where the callosal red fibers fuse in the midline (Figure1). Inter-rater reliability was assessed by Intraclass Correlation Coefficients (ICC) for all measurements. Student’s t-tests were carried out to compare differences in EI, CA and SA measurements between iNPH and HC groups.
Results
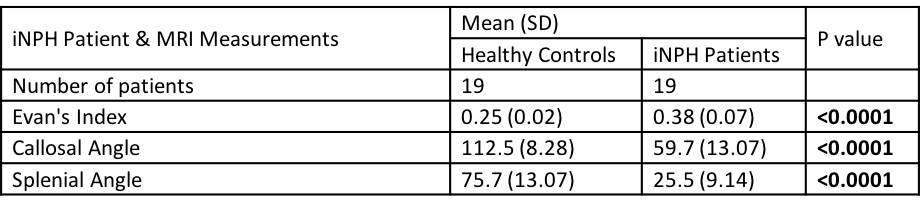
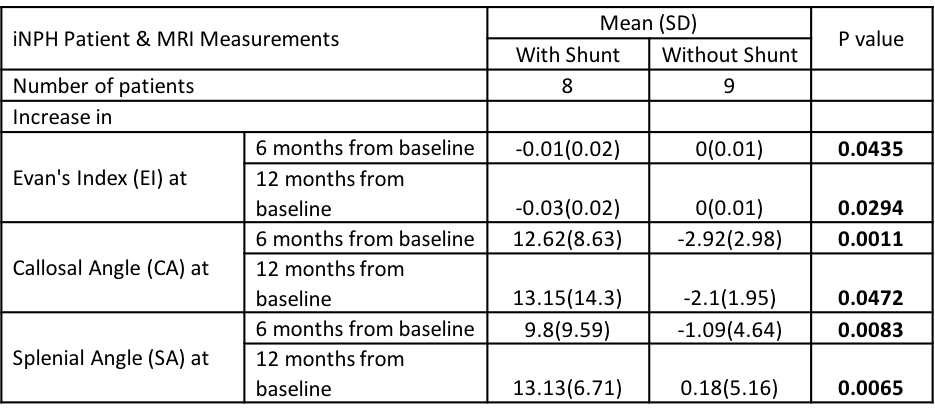
Nineteen iNPH patients (mean age 71.4 years) and 19 HC (mean age 72 years) were included in this study; 2 patients did not complete all follow-up MRIs. The mean ICC for all measurements was excellent at >0.95 (Table 1). All measurement showed significant differences between the iNPH and HC groups (Table 2). There was significant improvement in the EI (decrease), CA (increase) and SA (increase) measurements at both 6-month and 12-month follow-up MRI compared to baseline measurements in patients who were shunted compared to those who were not, who showed reverse trends in measurements.Discussion
Radiological measures such as Evan’s index (EI), callosal angle (CA) play a role in the diagnostic workup of iNPH. Additionally, EI and CA measurements are being used in combination with clinical assessments to evaluate the effectiveness of ventricular shunt treatment. Nevertheless, EI is nonspecific with respect to different causes of ventriculomegaly compared to CA measurements. However, the CA is clinically challenging to measure, and requires long training to reproduce a symmetric coronal plane for measurement. In comparison, the SA was easy to measure and training for measurement was short in our experience.
Similar to that reported in the literature, all baseline EI and CA measurements in iNPH patients were increased and narrowed respectively. SA measurements mirrored those of CA. In addition, EI, CA and SA were all sensitive to morphological changes pre and post-shunting in iNPH patients.
Conclusion
The splenial angle (SA) is a novel angle that is readily measured due to ease of identification of the angle subtended on the posterior red callosal fibers on color FA maps. It shows sensitivity and performance equal to that of the conventional EI and CA in differentiating iNPH patients from HC with perceptible radiological ventricular changes in patients with and without ventricular shunting. Further work needs to be done to assess the performance of the SA in differentiating iNPH from patients with ex vacuo ventriculomegaly from neurodegenerative atrophy, compared to EI and CA.Acknowledgements
We wish to thank the NMRC our funding agency, and the excellent team of MR radiographers & physicists for their kind assistance & support in this study.References
1. Williams MA, Relkin NR. Diagnosis and management of idiopathic normal-pressure hydrocephalus. Neurol Clin Pract. 2013 Oct;3(5):375-385
2. Ishii K, Kanda T, Harada A, Miyamoto N, Kawaguchi T, Shimada K, Ohkawa S, Uemura T, Yoshikawa T, Mori E. Clinical impact of the callosal angle in the diagnosis of idiopathic normal pressure hydrocephalus. Eur Radiol. 2008 Nov;18(11):2678-83.
3. Virhammar J, Laurell K, Cesarini KG, Larsson EM. The callosal angle measured on MRI as a predictor of outcome in idiopathic normal-pressure hydrocephalus. J Neurosurg. 2014 Jan;120(1):178-84.
Figures