2772
Altered white matter microstructure in anorexia nervosa: A voxel-based meta-analysis of diffusion tensor imaging1Huaxi MR Research Center (HMRRC), Department of Radiology, West China Hospital of Sichuan University, Chengdu, China, 2Department of Radiology, West China Hospital of Sichuan University, Chengdu, China
Synopsis
The
neurobiological underpinnings of anorexia nervosa (AN) remain unclear. Altered
white matter microarchitecture has been described, but findings are
inconclusive. To investigate a statistical consensus among published DTI studies
of altered white matter microarchitecture in AN, we conducted a quantitative
voxel-based meta-analysis of fractional anisotropy using Seed-based d Mapping.
The pooled results in AN showed robust reduction fractional anisotropy in the
interhemispheric connections, frontal-subcortical circuitry and limbic association fibers. This study
provides a thorough profile of WM microarchitecture alterations in patients
with AN and these intrinsic alterations may aid in developing effective
treatments in AN.
INTRODUCTION
Anorexia nervosa (AN) is a severe eating disorder. Although relatively rare (prevalence ~0.3%), AN has serious medical consequences (mortality ~10%) and thus poses a major clinical, psychological and societal burden1. In recent years, an increasing number of diffusion tensor imaging studies have reported abnormalities of white matter (WM) in patients with AN. However, the results are inconsistent and controversial. The aim of this paper was to address the most consistent and replicable WM microarchitecture abnormalities in patients with AN. Additionally, we also assess the potential effects of clinical variables on the reported WM abnormalities in patients with AN.METHODS
A systematic search was conducted for relevant studies that used voxel-wise analyses of WM microarchitecture in patients with AN. Seed-based d Mapping (SDM) was applied to analyze fractional anisotropy (FA) differences between AN patients and healthy controls. Meta-regression analysis was used to explore the effects of clinical characteristics on WM integrity in patients with AN.RESULTS
We identified a total of 12 data sets including 266 patients with AN and 282 healthy controls (summarized in Fig. 1. and Table1). The pool results showed significant FA reductions in the corpus callosum (CC), bilateral anterior thalamic radiation (ATR), thalamus, caudate nucleus and the cingulum in patients with AN (Fig. 2 and Table 2). No regions of increased FA were identified. The WM tracts are shown in Fig. 3.Meta-regression analysis revealed that the Mean Age and BMI were not linearly associated with FA changes.DISCUSSION
To the best of our knowledge, this is the first voxel-wise whole-brain meta-analysis investigating the intrinsic alterations of WM microarchitecture in patients with AN.
The most prominent FA reduction region in patients with AN was the CC. As we know, the CC is the principal interhemispheric commissure which integrate motor, perceptual, high-level cognitive and emotional regulatory functions of the brain2. An increasing number of studies now suggested this region involved in taste processing through the connection between the primary gustatory cortices, tactile and somatosensory cortices3. The alterations of WM microarchitecture in CC, as reflected by the decreased FA, might impair the somatosensory integration regarding food and thus contribute to food aversion.
Another intriguing finding of this meta-analysis is that an FA decrease in the bilateral ATR, thalamus and caudate nucleus which are key structures in the frontal-subcortical neural circuits related to behavioral inhibition, motivation and reward4,5. It is worth noting that patients with AN tend to the inability to inhibit weight- and body shape-related thoughts, thus, the repetitive, ritualistic, and highly controlled behaviors such as excessive food restriction and compulsively over-exercise may occur which compensate for their inability to control obsessive thoughts and anxiety5. Besides, patients with AN always gain a sense of pleasure from their punishment behaviors such as self-starvation and excessive excise which implicated the disturbance in rewards processing6. We speculate that the FA reduction in the ATR, thalamus and caudate nucleus may lead to the dysfunction of efficiency in information transfer in the frontal-subcortical neural circuits. Thus, the altered WM integrity in this neural circuity may form the basis of inhibition failure and disturbance in reward processing in AN patients.
Our study also identified significantly decreased FA in the cingulum in patients with AN. As the limbic association fibers, the cingulum is part of a network that integrates behaviors necessary for emotion identification and processing. Thus, Disruption of WM integrity in the cingulum could explain problems with emotion functioning difficulties in patients with AN, especially difficulties in dealing with negative with negative emotions7.
As potential factors may impact on FA value, our study identified no significant correlations between BMI and FA changes. It is possible that the patient characteristics of the included studies were heterogeneous, which may result in the negative results. Alternatively, WM microstructure impairments might be considered not as a direct consequence of malnutrition, but rather as a premorbid symptom of AN that accompanies neuropsychological impairments. However, these preliminary results need confirmation in more longitudinal studies.
CONCLUSION
Our study provides robust evidence that WM impairments in the interhemispheric connections, frontal-subcortical circuitry and limbic association fibers which may play an important role in AN pathogenesis.Acknowledgements
This work was supported by the National Natural Science Foundation (Grant Nos. 81371528, 81761128023,81220108013); Sichuan Provincial Foundation of Science and Technology of China (Grant No. 2013SZ0047). The authors reported no biomedical financial interests or potential conflicts of interest.References
1.Zipfel S, Giel KE, Bulik CM, Hay P, Schmidt U. Anorexia nervosa: aetiology, assessment, and treatment. The lancet Psychiatry 2015; 2(12): 1099-1111.
2.Hofer S, Frahm J. Topography of the human corpus callosum revisited--comprehensive fiber tractography using diffusion tensor magnetic resonance imaging. NeuroImage 2006; 32(3): 989-994.
3.Hayama T, Ogawa H. Callosal connections of the cortical taste area in rats. Brain research 2001; 918(1-2): 171-175
4.Eagle DM, Baunez C. Is there an inhibitory-response-control system in the rat? Evidence from anatomical and pharmacological studies of behavioral inhibition. Neuroscience and biobehavioral reviews 2010; 34(1): 50-72.
5.Marsh R, Maia TV, Peterson BS. Functional disturbances within frontostriatal circuits across multiple childhood psychopathologies. The American journal of psychiatry. 2009;166(6):664-674
6.Keating C. Theoretical perspective on anorexia nervosa: The conflict of reward. Neuroscience & Biobehavioral Reviews 2010; 34(1): 73-79.
7.Harrison A, Tchanturia K, Treasure J. Attentional bias, emotion recognition, and emotion regulation in anorexia: state or trait? Biological psychiatry 2010; 68(8): 755-761.
Figures


Fig. 2 Regions showing decreased fractional anisotropy in AN patients compared with healthy controls.
Abbreviation AN, Anorexia nervosa; B, Bilateral; CC, Corpus callosum; ATR, Anterior thalamic radiation.

Fig. 3 White matter tracts crossing these brain regions which showed decreased FA in patients with AN. Images show the interhemispheric fibers running through CC, the bilateral ATR projecting to the PFC, bilateral thalamus and caudate nucleus as well as the cingulum bundle.
Abbreviation : AN, Anorexia nervosa; FA, fractional anisotropy; B, Bilateral; CC, Corpus callosum; ATR, Anterior thalamic radiation. PFC, prefrontal cortex.
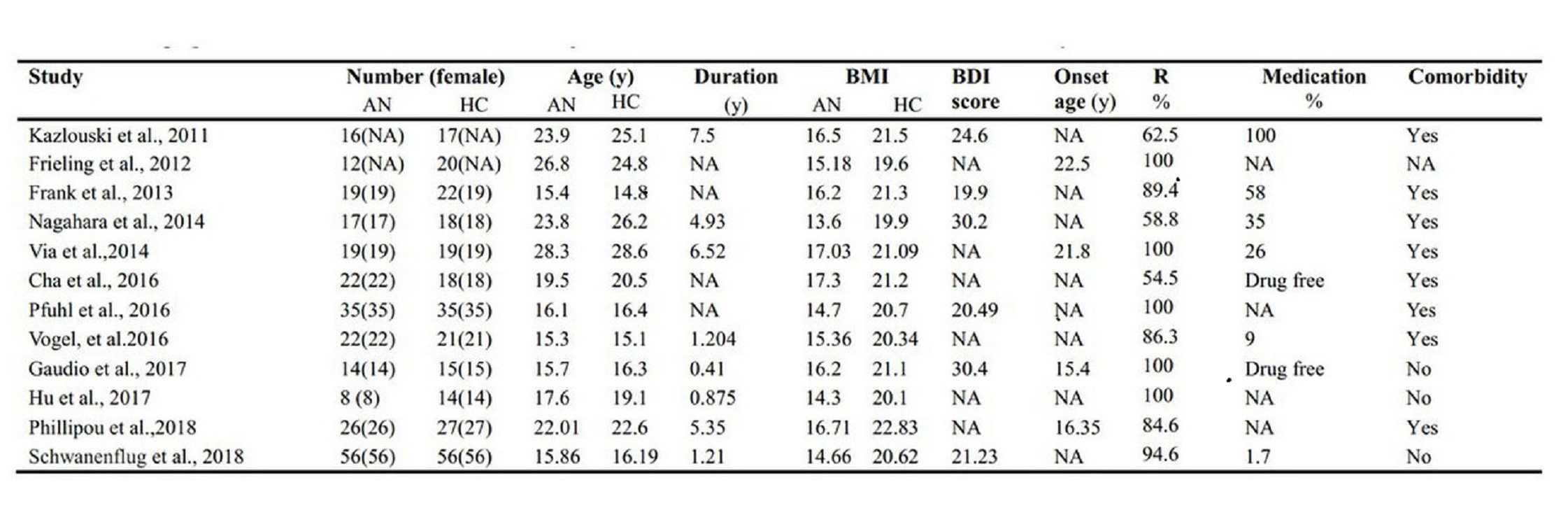
Table 1 Demographic and clinical characteristics of subjects in the 12 data sets included in the meta-analysis.
Abbreviations: BMI, body mass index; AN, anorexia nervosa; HC, health control; BDI, Beck Depression Inventory; R, restrictive subtype of anorexianervosa; NA, not available.
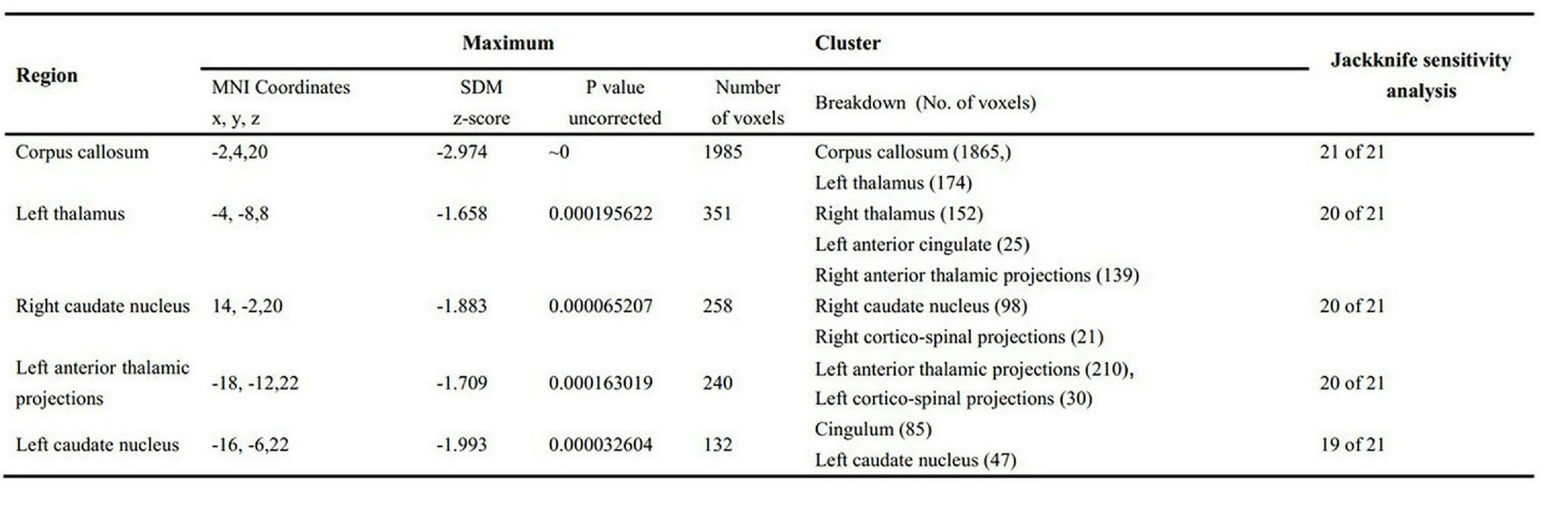
Table 2 The regions of decreased fractional anisotropy in AN patients compared with HC identified by the main meta-analyses .
Abbreviations: BA, Brodmann area; FA, Fractional anisotropy; MNI, Montreal Neurological Institute Space; L, left; R, right; SDM, Seed-based dMapping.