2770
Regional Cortical Thickness Changes and Neurocognitive Performance in Perinatally HIV-infected Youth1Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 2Pediatrics, Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, CA, United States, 3School of Nursing, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 4Semel Institute for Neuroscience and Human Behavior, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 5Infectious Disease-Pediatrics, Miller Children’s Hospital of Long Beach, Long Beach, CA, United States, 6Pediatrics, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 7Pediatrics, Children's Hospital Los Angeles, Los Angeles, CA, United States, 8Pediatrics, Keck School of Medicine at University of Southern California, Los Angeles, CA, United States, 9Radiology, Harbor-UCLA Medical Center, Los Angeles, CA, United States, 10Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
Despite effective viral suppression, youth with perinatal HIV (PHIVY) often demonstrate long-term cognitive deficits. We measured grey matter cortical thickness as a measure of brain structural integrity in 11 PHIVY receiving long term cART compared to 16 age-matched controls and assessed neurocognitive performance. The PHIVY group performed significantly worse than controls. Regions of significantly thinner and thicker cortex in PHIVY were observed which may contribute to these deficits in neurocognitive function. Cortical thickness in PHIVY was correlated with current CD4 count and neurocognitive performance. Our findings suggest the potential importance of continued monitoring of PHIVY.
Introduction:
Despite the success of combination antiretroviral therapy (cART), the brain remains a reservoir for latent HIV in perinatal HIV (PHIV)1-5. HIV infection during a critical period of brain development may be particularly harmful to developing brains, with lasting effects in adulthood. Youth with PHIV (PHIVY) often demonstrate long-term cognitive deficits and developmental delay6,7. Though clinically important, our understanding of the pathophysiology of cognitive deficits in this PHIV population remains limited and unclear8. While brain volume loss in various cortical and subcortical regions9,10 of adult HIV patients has been reported11, there is sparse knowledge about these changes in PHIVY. The purpose of this study is to use structural MRI data to characterize grey matter cortical thickness as a measure of brain structural integrity in PHIVY receiving long term cART and to determine how cortical thickness relates to HIV disease severity and cognitive performance.Materials and Methods:
We investigated eleven PHIVY (age 22.50±2.9 years) and sixteen healthy controls (HC) (age 22.45±3.0 years). All MRI studies were performed on a Siemens 3T Prisma MRI scanner using a 16-channel phased-array head ‘receive’ coil. High-resolution T1-weighted images were acquired using a MPRAGE sequence with TR/TE=2200/2.41 ms, inversion time=900 ms, flip angle=9°, matrix size=320×320, FOV=230×256 mm2, slice thickness=0.9 mm, 192 slices. For PHIVY subjects, the following additional data were collected: age at first treatment, HIV viral load, highest viral load, CD4 T-cell counts, lowest CD4, lowest CD4%, current antiretroviral therapy, and presence of HIV encephalopathy. In addition, a comprehensive neuropsychological (NP) assessment battery was also administered to all participants and grouped into 13 cognitive domains. Raw data and Z-scores were transformed into T-scores by utilizing established normative data. Domain T-scores were calculated by averaging the T-score of the individual tests comprising the neurocognitive domain.
Demographic and neurocognitive performance were assessed by independent samples t-tests and MANCOVA (age, sex covariates) respectively. We used the FreeSurfer and MATLAB-based SPM12 software packages for data processing and analysis as described in detail elsewhere12-14. The FreeSurfer processing stream was followed to generate cortical thickness across the brain, except for cerebellar areas using a general linear model with condition (PHIVY/HC) and sex as independent variables. We also assessed correlations of cortical thickness with cognitive domain T-scores and clinical variables. Each hemisphere was analyzed separately, with 10 mm smoothing. We used a threshold of P ≤ 0.05 and the areas of significant difference were overlaid onto the inflated cortical surface.
Results:
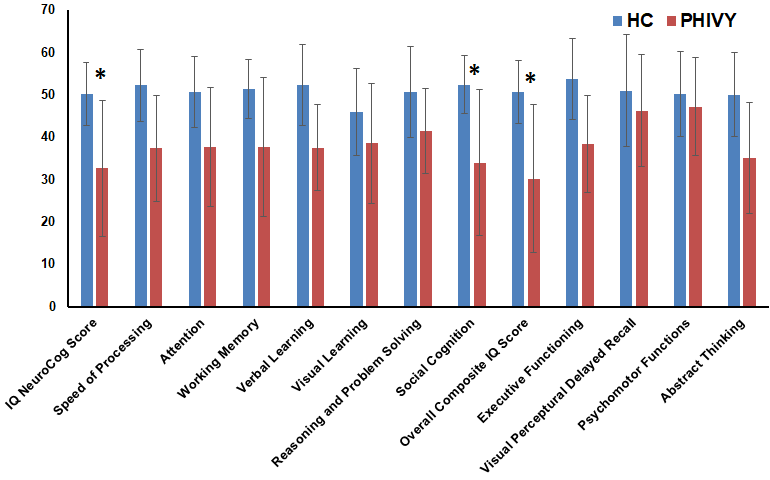
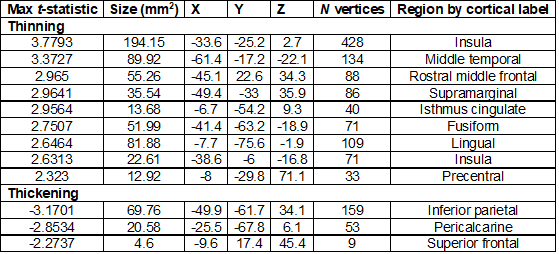
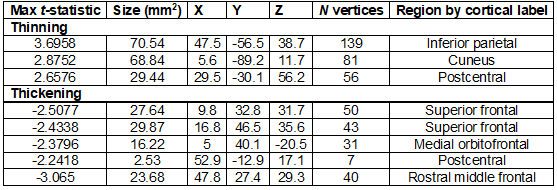
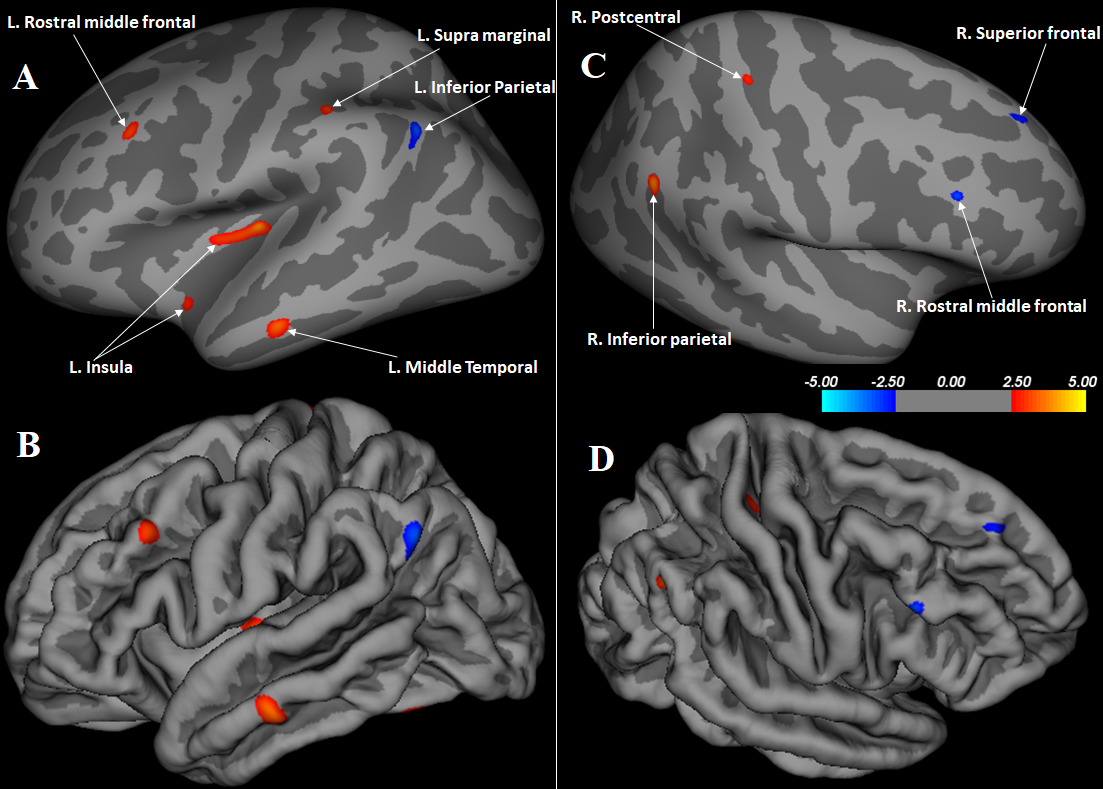
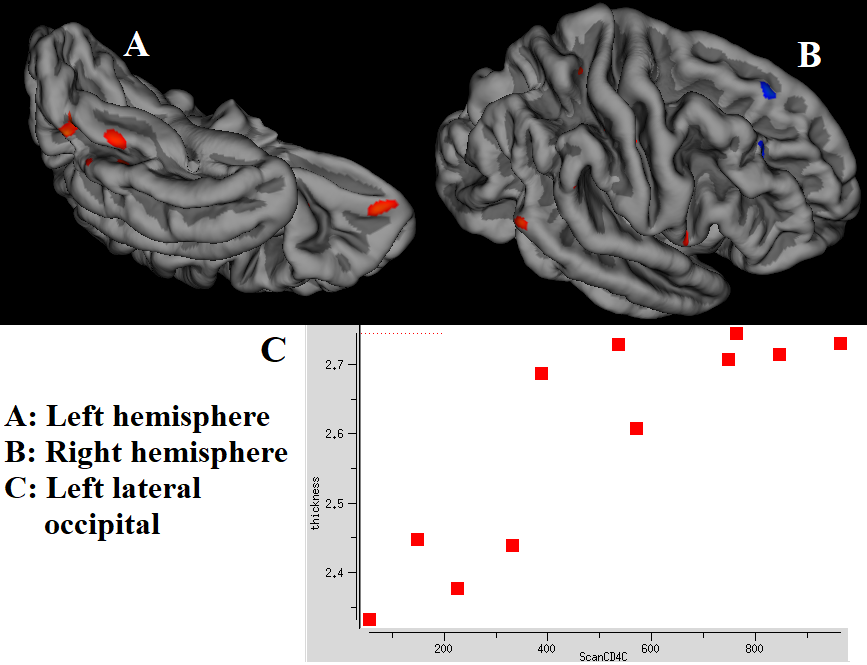
Although the two groups were demographically similar, PHIVY performed significantly worse than HC on neuropsychological testing (Fig.1). Significantly lower cognitive domain scores were found in IQ Neuro Cognitive score, Social Cognition and Overall Composite IQ score in PHIV-infected youth. Regions of significantly thinner or thicker cortex in PHIV are shown in Table 1 (left hemisphere) and Table 2 (right hemisphere). Representations of these cortical thickness differences between PHIVY and HC in the left and right hemispheres are shown in Fig.2 from multiple views overlaid onto the FreeSurfer template pial surface, and a lateral, inflated view. Reductions in cortical thickness in PHIVY were associated with lower CD4 count in 10 regions in the left and 9 in the right hemisphere (Fig.3). Three regions in the right hemisphere showed a negative correlation. Cortical modeling also revealed a strong relationship between poorer neuropsychological performance (IQ Neuro Cognitive score, Social Cognition and Overall Composite IQ) and cortical thickness reductions in several regions.Discussion:
The PHIVY group performed significantly more poorly than HC on neuropsychological tests, adding to the growing body of evidence that suggests HIV-related cognitive impairment remains frequent despite effective treatment and minimal comorbidities15. Our results of altered cortical thickness are consistent with a previous study on younger perinatally HIV-infected pediatric patients16. Cortical thinning observed in PHIVY may be due to cell death or neuronal and glial cell injury resulting from toxicity of HIV viral proteins and a proinflammatory process16,17. The few brain regions showing cortical thickening could be related to stress-induced hypertrophy of medium spiny neurons and is consistent with previous studies showing subcortical hypertrophy in multiple brain sites18. In addition, cortical thickness may also increase due to neuro-inflammation or abnormal neural development in the presence of the HIV and cART. The association between cortical thickness and CD4 count reported here supports the hypothesis that subcortical structures are particularly vulnerable to the HIV virus.Conclusion:
Altered cortical thickness and neurocognitive deficits were observed in PHIVY. Presence of altered cortical thickness may contribute to the observed neurocognitive deficits. Further studies are needed for a better understanding of HIV effects on brain structural changes throughout life under standard ART treatment.Acknowledgements
This research was supported by the NIH grant: 1R21NS090956-01A1.References
1. Lee GM, Gortmaker SL, McIntosh K. Quality of life for children and adolescents: impact of HIV infection and antiretroviral treatment. Pediatrics. 2006;117(2):273-283.
2. Palella FJ Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338(13):853-860.
3. Tardieu M, Mayaux MJ, Seibel N, et al. Cognitive assessment of school-age children infected with maternally transmitted human immunodeficiency virus type 1. J Pediatr. 1995;126(3):375–379.
4. Patel K, Ming X, Williams PL, et al. International Maternal Pediatric Adolescent AIDS Clinical Trials 219/219C Study Team Impact of HAART and CNS-penetrating antiretroviral regimens on HIV encephalopathy among perinatally infected children and adolescents. AIDS. 2009;23(14):1893–1901.
5. Zhang YL, Ouyang YB, Liu LG, Chen DX. Blood-brain barrier and neuro-AIDS. Eur Rev Med Pharmacol Sci. 2015;19(24):4927-4939.
6. Smith R, Chernoff M, Williams PL, et al. Impact of HIV severity on cognitive and adaptive functioning during childhood and adolescence. Pediatr Infect Dis J. 2012;31(6):592–598.
7. Nagarajan R, Sarma MK, Thomas MA, et al. Neuropsychological function and cerebral metabolites in HIV-infected youth. J. Neuroimmune Pharmacol. 2012;7(4):981-990.
8. Thompson PM, Jahanshad N. Novel Neuroimaging Methods to Understand How HIV Affects the Brain. Curr HIV/AIDS Rep. 2015; 12(2):289–298.
9. Holt JL, Kraft-Terry SD, Chang L. Neuroimaging studies of the aging HIV-1-infected brain. J Neurovirol. 2012;18(4):291–302.
10. Ances BM, Hammoud DA. Neuroimaging of HIV Associated Neurocognitive Disorders (HAND). Curr Opin HIV AIDS. 2014;9(6):545–551.
11. Sanford R, Fernandez Cruz AL, Scott SC, et al. Regionally Specific Brain Volumetric and Cortical Thickness Changes in HIV-Infected Patients in the HAART Era. J Acquir Immune Defic Syndr. 2017;74(5):563-570.
12. Macey PM, Kheirandish-Gozal L, Prasad JP, et al. Altered Regional Brain Cortical Thickness in Pediatric Obstructive Sleep Apnea. Front Neurol. 2018;9:4.
13. Ashburner J, Friston KJ. Unified segmentation. Neuroimage. 2005;26:839–851.
14. Dale AM, Fischl B, Sereno MI. Cortical surface-based analysis. I. Segmentation and surface reconstruction. NeuroImage. 1999;9(2):179–194.
15. Heaton RK, Clifford DB, Franklin DR, et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology. 2010;75(23):2087–2096.
16. Yadav SK, Gupta RK, Garg RK, et al. Altered structural brain changes and neurocognitive performance in pediatric HIV. Neuroimage Clin. 2017;14:316-322.
17. Zhang K, McQuibban GA, Silva C, et al. HIV-induced metalloproteinase processing of the chemokine stromal cell derived factor-1 causes neurodegeneration. Nat Neurosci. 2003;6:1064–1071.
18. Sarma,MK, Nagarajan R, Keller MA, et al. Regional brain gray and white matter changes in perinatally HIV-infected adolescents. Neuroimage Clin. 2014;4:29–34.
Figures