2753
White matter microstructural changes in schizophrenia: A study using normative-model-based statistical analysis1Institute of Engineering and System Science, National Tsing Hua University, Hsinchu, Taiwan, 2Institute of Medical Device and Image, National Taiwan University College of Medicine, Taipei, Taiwan, 3Department of Psychiatry, National Taiwan University Hospital, Taipei, Taiwan, 4AcroViz Technology Inc., Taipei, Taiwan, 5Molecular Imaging Center, National Taiwan University College of Medicine, Taipei, Taiwan
Synopsis
White matter microstructural changes have been found in schizophrenia but the effects of gender and age on these changes remains entangled. This study aimed to quantify the white matter changes in 158 schizophrenia patients using a novel approach which calculated the z scores based on the normative models built from 524 healthy subjects across lifespan. Our results showed that twelve tracts had significant differences between schizophrenia patients and controls.
Introduction
Schizophrenia is a debilitating and multi-symptom mental disorder that is characterized by disrupted cognitive, social and behavior functions[1]. Previous studies explored white matter integrity in schizophrenia using a region-of-interest approach and group comparison by matching gender and age[2]. Such approach cannot totally eliminate the age effect because the age effect is not linear. Here, we recruited 524 healthy subjects and 158 schizophrenia patients. We explored white matter microstructure using whole-brain tractography-based analysis (TBAA)[3] and calculated the z scores of generalized fractional anisotropy (GFA) by referencing the mean and standard deviation of GFA of respective the healthy population with the same gender and age. By comparing the GFA z scores, we aimed to identify altered white matter tracts that were not confounded by age and gender.Methods
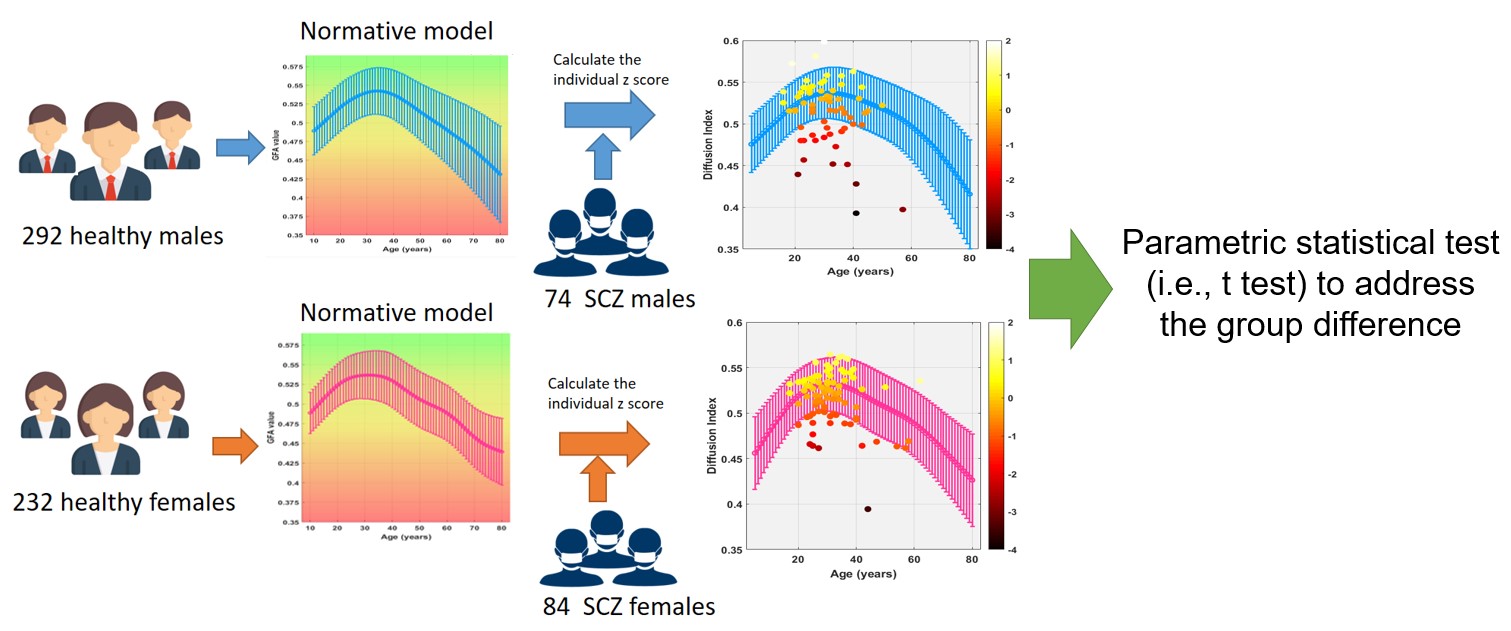
Study design: To investigate white matter microstructure changes in schizophrenia, we established the normative models of GFA based on 524 healthy subjects and the z scores of 158 patients were calculated from the normative models individually. Subjects: 524 healthy controls (HC) (292 males, age: 13-80 years) had no history of schizophrenia, schizoaffective disorder and other psychotic disorders. 158 schizophrenia patients (SCZ) (74 males, mean age: 30.53 years, SD=8.18) were diagnosed according to the DSM-IV-TR criteria and underwent assessment of psychopathology and function by an experienced psychiatrist using the Positive and Negative Syndrome Scale (PANSS). MRI examination: We used a 3T scanner (TIM Trio, Siemens, Germany) to obtain the high-resolution T1-weighted imaging and diffusion spectrum imaging (DSI). T1-weighted images were acquired by using a three-dimensional magnetization-prepared rapid gradient-echo (3D MP-RAGE) pulse sequence with the following parameters: TR/TE = 2000/3 ms, flip angle = 9o, FOV = 256 X 256 mm2, resolution = 1 X 1 X 1 mm3. DSI data were acquired using a pulsed gradient twice-refocused single-shot spin-echo echo-planer imaging (EPI) sequence: TR/TE = 9600/130 ms, FOV = 200 X 200 mm2, matrix size = 80 X 80, slice thickness = 2.5 mm, axial slices with no gap. The diffusion-encoding scheme entailed 102 diffusion gradient directions with the maximum diffusion sensitivity (bmax) of 4000 s/mm2. Data analysis: This study used TBAA[3] to obtain a 2D connectogram for each DSI dataset in healthy controls and schizophrenia patients. The connectogram provided GFA profiles of 76 white matter tract bundles. We estimated the normative models by averaging the mean GFA and calculating the standard deviation on every age of two genders across lifespan. We calculated the individual z score of SCZ by subtracting the mean value of GFA in the respective healthy population, and divided by the standard deviation. One sample t-test was examined to compare the differences in z score of each tract bundle between HC and SCZ. The Bonferroni correction method for false discovery rate control was used to correct for multiple comparisons.Results
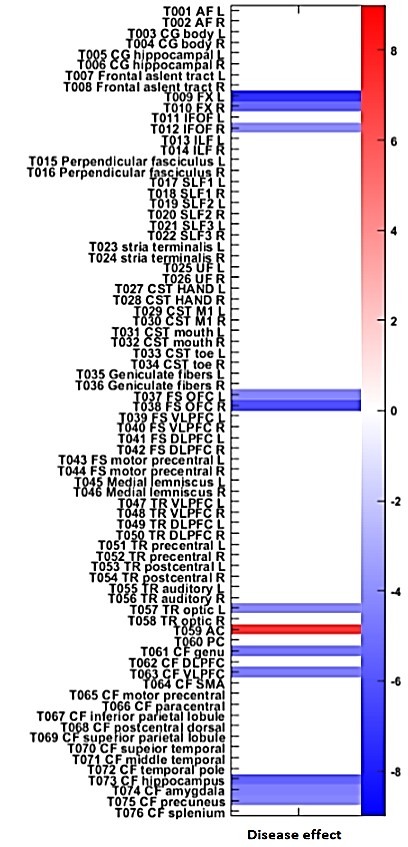
The z scores of GFA revealed 12 tracts showing significant differences between schizophrenia patients and controls. These 12 tracts included bilateral fornices, right inferior frontal occipital fasciculus, bilateral frontal striatum of the orbitofrontal cortex, left thalamic radiation of the optic radiation, anterior commissure, the callosal fiber (CF) of the genu, CF of the ventral lateral prefrontal cortex, CF of the hippocampus, CF of the amygdala and CF of the precuneus.Discussion
In this study, we found 12 tracts that were significantly different between healthy controls and SCZ. Lower GFA in these tracts may disrupt functioning of spatial memory[4] and language streams, producing domain-specific neurocognitive deficits that interfere with higher-order cognitive abilities5. Disruption in the frontal and temporal lobes has been implicated in schizophrenia6. Our results converge with previous findings[2,4,5,6,7] and suggest that the alteration of white matter tract integrity in these 12 tracts may be possible biomarkers of vulnerability for developing schizophrenia.Conclusion
Normative model based statistical analysis is a method which has no assumptions on the linearity of the age effect, and is more sensitive to detect differences of white matter microstructure genuine to disease. By calculating the z scores, we can know the individual differences in SCZ, and the z scores may be a potential index as a reference for diagnosis. The normative model appears to be more reliable to detect disease-specific substrates without gender and age effects.Acknowledgements
No acknowledgement found.References
1. Millan, M. J., Fone, K., Steckler, T., et al. Negative symptoms of schizophrenia: clinical characteristics, pathophysiological substrates, experimental models and prospects for improved treatment. Eur Neuropsychopharmacol.2014; 24(5), 645-692.
2. Bora, E., Fornito, A., Radua, J.,et al. Neuroanatomical abnormalities in schizophrenia: a multimodal voxelwise meta-analysis and meta-regression analysis. Schizophr Res, 2011;127(1-3), 46-57.
3. Chen, Y. J., Lo, Y. C., Tseng, W. Y. ,et al. Automatic whole brain tract-based analysis using predefined tracts in a diffusion spectrum imaging template and an accurate registration strategy. Hum Brain Mapp, 2015; 36(9), 3441-3458.
4. Fitzsimmons, J., Kubicki, M., Smith, K., Bushell, G.,et al. Diffusion tractography of the fornix in schizophrenia. Schizophr Res, 2009; 107(1), 39-46.
5. Epstein, K. A., Cullen, K. R., Mueller, B. A., Robinson, P., Lee, S., & Kumra, S. White matter abnormalities and cognitive impairment in early-onset schizophrenia-spectrum disorders. J Am Acad Child Adolesc Psychiatry, 2014; 53(3), 362-372 e361-362.
6. Millan, M. J., Fone, K., Steckler, T., & Horan, W. P. . Negative symptoms of schizophrenia: clinical characteristics, pathophysiological substrates, experimental models and prospects for improved treatment. Eur Neuropsychopharmacol,2014; 24(5), 645-692.
7. Whitford, T. J., Savadjiev, P., Kubicki, M., O'Donnell,et al. Fiber geometry in the corpus callosum in schizophrenia: evidence for transcallosal misconnection. Schizophr Res,2011; 132(1), 69-74.
Figures