2742
Absolute quantitative dynamic susceptibility contrast cerebral perfusion imaging using the Self-Calibrated EPI sequence in patients with ischemic strokeXiaoyue Ma1,2, Yan Wang1,2, Qiang Li1, Menghuan Zhang1,2, Xianchang Zhang3, Yusong Lin4, and Meiyun Wang1,2
1Department of Radiology, Zhengzhou University People’s Hospital & Henan Provincial People’s Hospital, Zhengzhou, China, 2Henan Key Laboratory for Medical Imaging of Neurological Diseases, Zhengzhou, China, 3MR Collaboration, Siemens Healthcare Ltd., Beijing, China, 4Cooperative Innovation Center of Internet Healthcare & School of Software and Applied Technology, Zhengzhou University, Zhengzhou, China
Synopsis
This study aims to explore the clinical value of the absolute quantitative dynamic susceptibility contrast cerebral perfusion-weighted imaging using Self-Calibrated EPI sequence (SCALE-PWI) in patients with ischemic stroke. SCALE-PWI could provide reliable quantitative measurement of cerebral blood flow (CBF), cerebral blood volume and mean transit time in a quite short scan time of 2:14 mins. Results suggest the CBF values in infarct core are significantly lower than the values in ischemic penumbra. In conclusion, the SCALE-PWI could provide quantitative hemodynamic information in a quite short scan time, thus may serve as a guide for tissue-based decision making and personalized treatment planning in acute stroke.
Introduction
Magnetic resonance (MR) diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI) offer a unique insight into ischemic stroke pathophysiology.1 An absolute quantitative dynamic susceptibility contrast (DSC) cerebral PWI technique has recently been proposed. It is based on the self-calibrated EPI sequence (SCALE-PWI),2 and could provide reliable quantitative measurement of cerebral blood flow (CBF), cerebral blood volume (CBV), and mean transit time (MTT) in a short scan time. This technique may offer the opportunity to make a personalized therapy plan for each patient with ischemic stroke, based on complete quantitative hemodynamic information. The purpose of this study was to investigate the clinical value of SCALE-PWI in detecting salvageable areas in stroke patients.Methods
Eleven patients with ischemic stroke underwent routine MRI (T1WI, T2WI, FLAIR, DWI) and SCALE-PWI scanning in a 3T Magnetom Prisma MR scanner (Siemens Healthcare, Erlangen, Germany) with a 64-channel head coil. The parameters of the prototype SCALE-PWI protocol were as follows: TR/TE = 1600/30 ms, matrix size = 128 × 128, flip angle = 20º, field of view = 220 × 220 mm2, slice thickness = 6 mm, and acquisition time = 2:14 mins. The subjects were scanned with a delay of 46 secs. between consecutive modules of SCALE-PWI. A single dose (0.1 mmol/kg body weight) of Gd-DTPA contrast agent (Magnevist, Berlex, Montville, NJ, USA) was injected during the DSC module of SCALE-PWI, followed by a 20 mL saline flush, at a rate of 4 mL/sec. The quantitative CBV, CBF, and MTT maps were inline processed immediately after the scan. Two radiologists independently drew the region of interest (ROI) of the lesion on each map for the statistical analyses. The ROI1 contained the entire abnormal areas on the CBV, CBF, and MTT images, and the ROI2 contained the lesions that appeared hyperintense on DWI. We subsequently calculated the value of CBVm, CBFm, and MTTm in the DWI/PWI mismatch areas. Paired t-tests were performed to detect differences in the CBV and CBVm, CBF and CBFm, and MTT and MTTm, using SPSS 17.0 (IBM Corp., Armonk/NY, USA). P < 0.05 was considered statistically significant.Results
The images and quantitative results for one representative subject are shown in Fig. 1. All the values are shown in the form of mean ± standard deviation. The CBF values of the infarct core (ROI2) were significantly lower than the CBFm values of the DWI/PWI mismatch areas [(25.53 ± 16.57) ml/100g/min vs. (33.90 ± 17.65) ml/100g/min, P = 0.03] in patients with ischemic stroke (Fig. 2). The CBV values were: (1.56 ± 0.75) ml/100g, and the CBVm values were: (2.23 ± 1.39) ml/100g. The MTT values were: (4.19 ± 1.21) secs, and the MTTm values were: (9.43 ± 17.00) secs. However, no significant differences were observed between the CBV and CBVm, or MTT and MTTm (P = 0.08 and 0.25, respectively).Discussion
The research on ischemic stroke has focused not only on the early detection of lesions but also on the goal of tissue-based decision-making and personalized acute stroke treatment1, which are associated with the differentiation of infarcted and salvageable areas. This project found that the CBF values in DWI/PWI mismatch areas (traditionally considered to be salvageable areas) were significantly higher than the CBF values in the infarct core, suggesting that the quantitative CBF value obtained by the SCALE-PWI technique may be a promising indicator for distinguishing the salvageable area. Our findings show that the tissues whose CBF values are higher than 52.7 ml/100g/min could be salvageable, which is useful information for deducing tissue-based treatment. Different from the previous semi-quantitative method, the SCALE-PWI technique could provide complete quantitative information in a relatively short scan time (only 2:14 mins). The values of the CBVm and CBFm were similar to previous findings in the ischemic penumbra, showing hypoperfusion.3 But no significant difference was observed between the CBV and CBVm, or the MTT and MTTm. We speculate that it may be caused by recanalization therapy, collateral circulation, or a small sample size. The value of SCALE-PWI in acute ischemic stroke needs to be further investigated in the future.Conclusion
SCALE-PWI could provide useful quantitative hemodynamic information to detect the ischemic penumbra in a relatively short scan time, and thus may serve as a guide for tissue-based decision-making and personalized treatment planning in acute stroke.Acknowledgements
This research was supported by the NNSFC (81720108021, 81772009, 81601466, 81641168, 31470047), National Key R&D Program of China (YS2017YFGH000397), Scientific and Technological Research Project of Henan Province (182102310162) and the Key Project of Henan Medical Science and Technology Project (201501011).References
- Bateman M, Slater LA, Leslie-Mazwi T, et al. Diffusion and Perfusion MR Imaging in Acute Stroke: Clinical Utility and Potential Limitations for Treatment Selection. Top Magn Reson Imaging. 2017;26(2):77-82.
- Srour JM, Shin W, Shah S, et al. SCALE-PWI: A pulse sequence for absolute quantitative cerebral perfusion imaging. J Cereb Blood Flow Metab. 2011;31(5):1272-1282.
- Sparacia G, Iaia A, Assadi B, et al. Perfusion CT in acute stroke: predictive value of perfusion parameters in assessing tissue viability versus infarction. Radiol Med, 2007. 112(1):113-22.
Figures
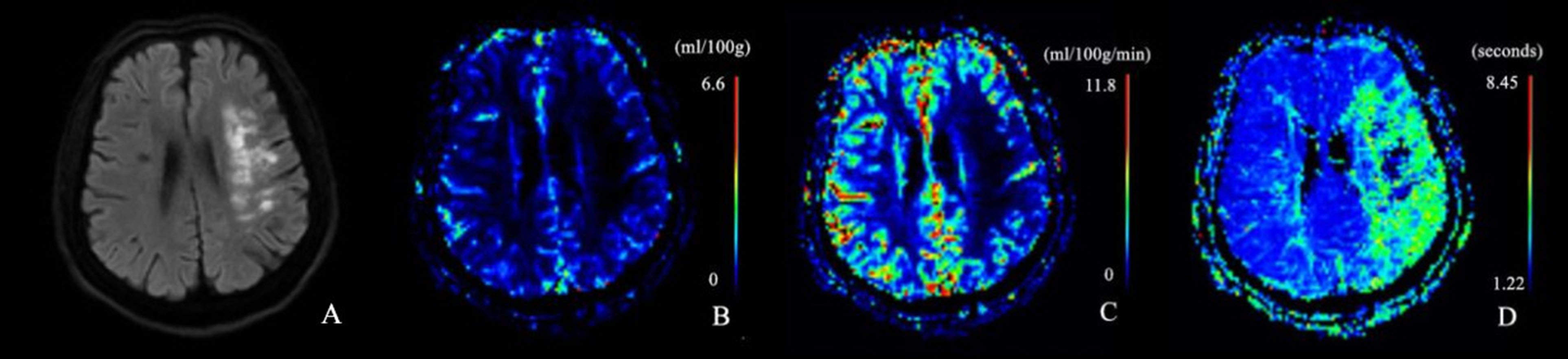
Figure 1.
Axial MR DWI (A), and SCALE-PWI maps for CBV (B), CBF (C), and MTT (D) in a 62-year-old male patient with
cerebral ischemic stroke in the left periventricular white matter.
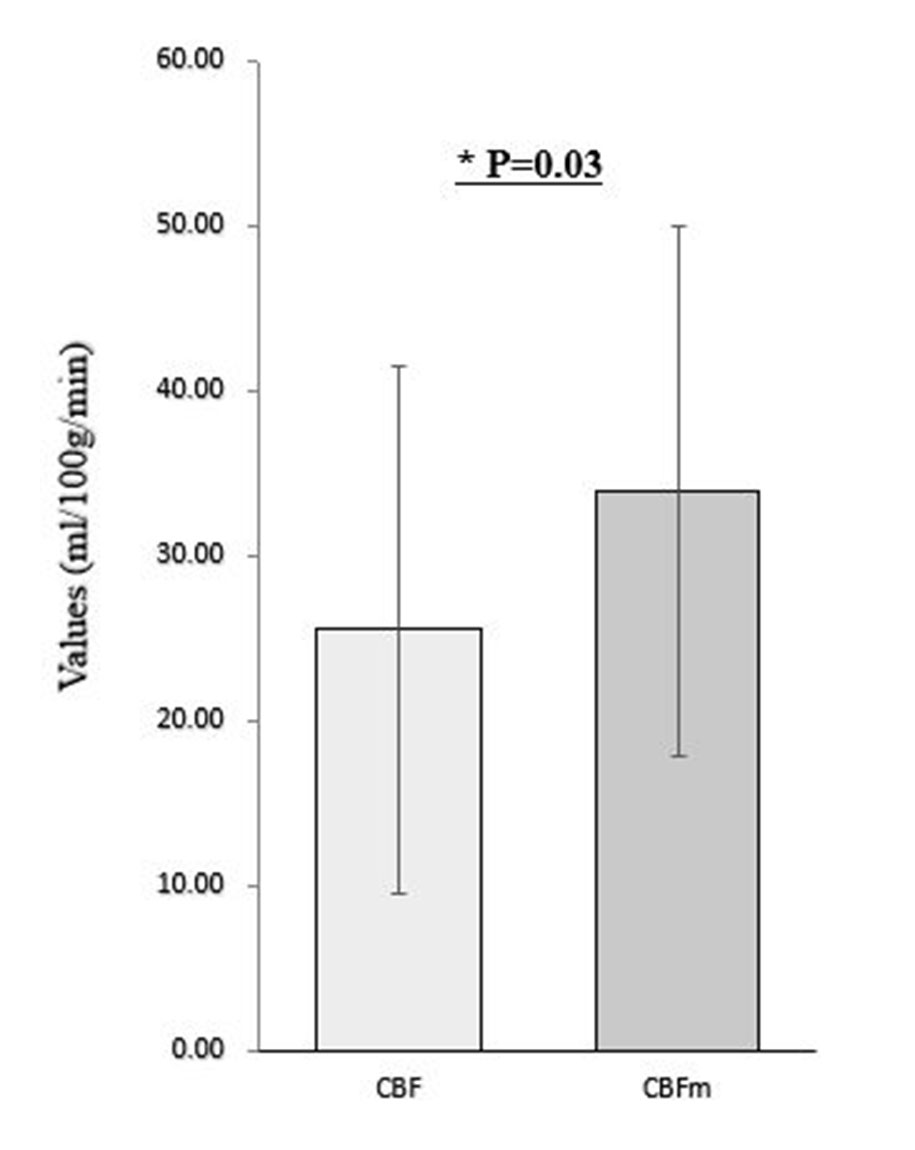
Figure 2. The paired t-test showed that the CBF in the infarct
core was significantly lower than the CBF in the ischemic penumbra (P = 0.03).
CBF: the values of cerebral blood flow in the infarct core. CBFm:
the values of cerebral blood flow in the ischemic penumbra.