2741
Ipsilateral Thalamic Diaschisis in Stroke Patients1University Hospital Zurich, Zurich, Switzerland
Synopsis
Presence of ipsilateral thalamic diaschisis in stroke patients, detected using BOLD-CVR, is characterized by thalamic volume reduction, reduced thalamic blood flow, and worse stroke severity scores at admission as well as 3 months follow-up. This finding suggests that ipsilateral thalamic diaschisis may be an important clinical imaging marker in stroke patients.
INTRODUCTION
Diaschisis, first introduced by the Russian-Swiss neuropathologist Constantin von Monakow in 1914, refers to a brain injury-induced drop in neuronal activity in distant but functionally connected brain regions.1 About 70 years later, the first diaschisis imaging study revealed a reduction in both blood flow and metabolism in the cerebellar hemisphere contralateral to a supratentorial stroke lesion (termed crossed cerebellar diaschisis).2 Thereafter, others have used Positron Emission Tomography (PET) to show the presence of another type of diaschisis, named ipsilateral thalamic diaschisis.3, 4 Although studies have shown that the presence of crossed cerebellar diaschisis in patients after a supratentorial stroke correlates to worse neurological performance, the clinical prognostic value of ipsilateral thalamic diaschisis, however, remains a matter of debate.5 6 In general, diaschisis does not have a direct clear clinical or structural anatomical correlate and therefore remains primarily a functional imaging diagnosis, usually obtained with PET.2, 5, 7-11 Further advancements in multimodal diaschisis imaging include MRI based methods such as arterial spin labeling and blood-oxygenation-level-dependent MRI cerebrovascular reactivity (BOLD-CVR).12-15 To characterize ipsilateral thalamic diaschisis, we investigate the hemodynamic, structural, and prognostic implications. For this we use, blood oxygenation-level dependent cerebrovascular reactivity (BOLD-CVR) and complementary Diamox challenged 15(O)-H2O PET imaging as well as two stroke severity scores. We show that presence of ipsilateral thalamic diaschisis in stroke patients is characterized by thalamic volume reduction, reduced thalamic blood flow whilst preserved blood flow response to a vasoactive stimulus, and worse neurological performance.METHODS
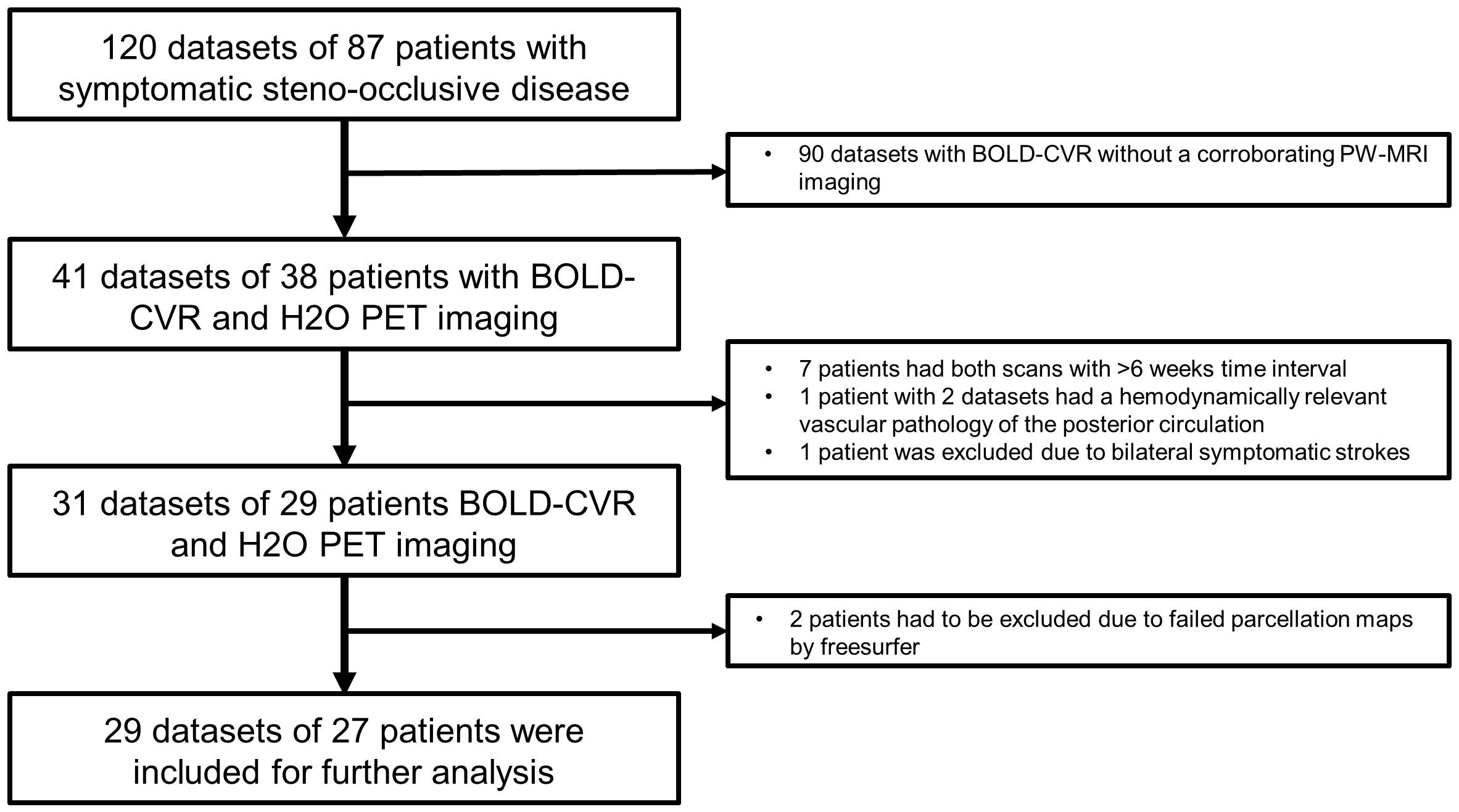
A single-institution prospective cross-sectional study conducted in stroke patients undergoing both BOLD-CVR as well as Diamox-challenged 15(O)-H2O-PET. Further details on the setup have been described in previous publications16. Iterative temporal decomposition of the BOLD-CVR data was used to avoid transient phases confounds.17
Follow-up was at least 3 months. In addition, 15 age-matched healthy subjects were included. ITD was diagnosed based on a BOLD-CVR thalamic asymmetry index (TAI) >+2 standard deviations from healthy subjects. Cerebral blood flow differences was asses using a PET-based TAI before and after Diamox challenge. Thalamic volume masks were determined using Freesurfer. Neurological status at admission and after 3 months were determined with NIHSS and mRS scores.
RESULTS
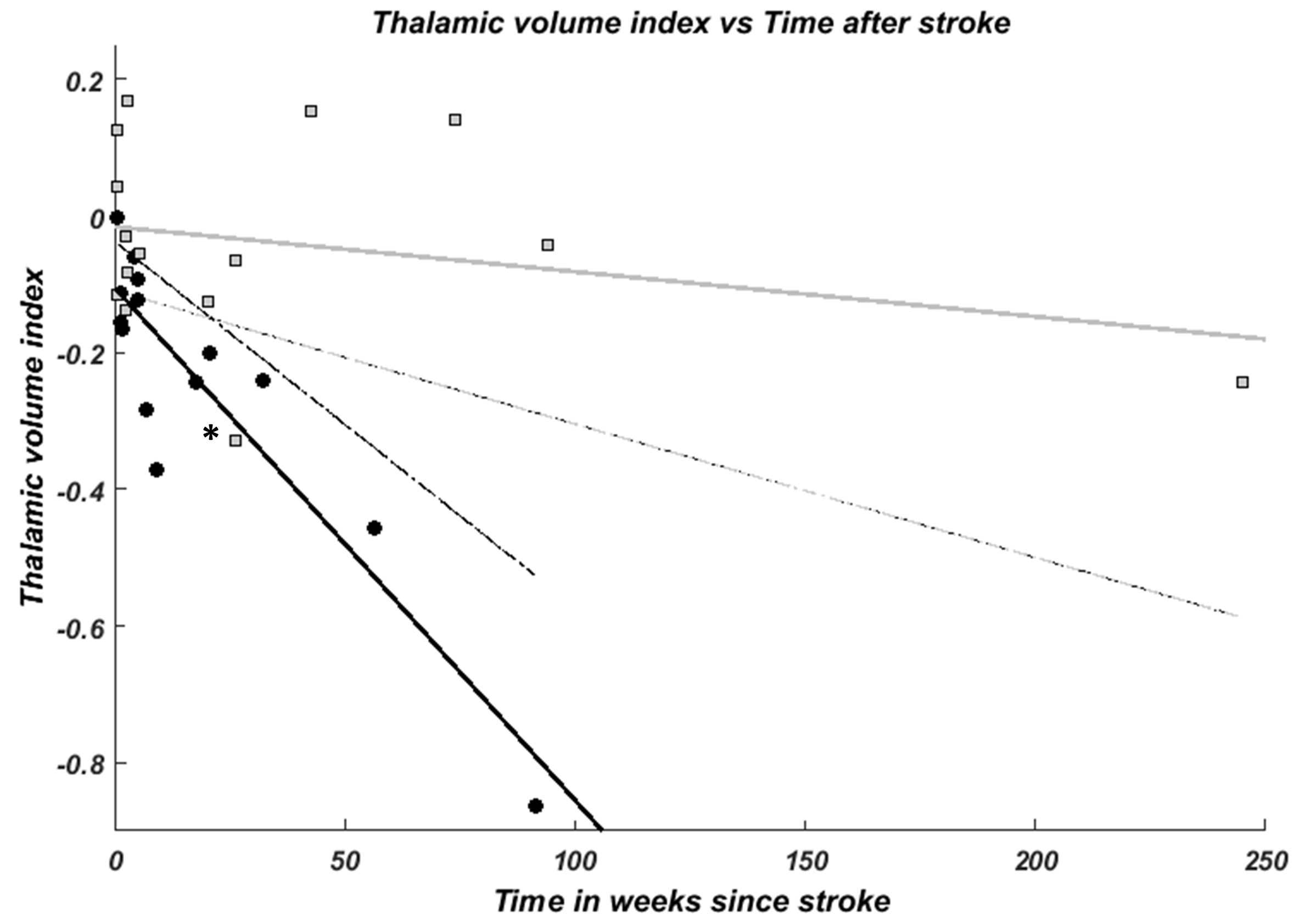
14/29(48%) patients were diagnosed with ITD. PET-TAI before and after Diamox challenge were increased in patients with ITD, indicating an ipsilateral decrease in thalamic blood flow. Patients with ITD exhibited a marked ipsilateral thalamic volume decrease as compared to patients without ITD and healthy subjects. Furthermore, patients with ITD had worse NIHSS and mRS at admission and after 3 months follow-up.DISCUSSION
The presence of ipsilateral thalamic diaschisis strongly correlated with an increased thalamic volume asymmetry (i.e. larger volume difference between the affected and unaffected thalamus) in the absence of structural thalamic lesion, reduced thalamic blood flow, as well as a worse initial neurological status and a worse neurological performance after three months.
Significance of ipsilateral thalamic diaschisis detection
The reduction of thalamic metabolism and cerebral blood flow following a supratentorial stroke in humans was first described in the early 1980. It was first named ipsilateral thalamic diaschisis by de Reuck et al. in 1995 with an incidence (~50%) matching ours. 3 18, 19 More recently, the presence of ipsilateral thalamic diaschisis was determined in patients with acute middle cerebral artery stroke based on visual assessment of signs of hypoperfusion on ≥2 CT-perfusion maps.6 The occurrence of ipsilateral thalamic diaschisis (~20%) in their patient cohort is significantly lower than our incidence. This difference could be explained by the difference in imaging modality with less imaging resolution as well as the fact that their diagnosis of ipsilateral thalamic diaschisis was done by visual inspection and inter-reader agreement. This paper is also currently the only paper investigation prognostic implications of ipsilateral thalamic diaschisis, failing to show any prognostic significance. However, as the previously mentioned methodological differences imply inclusion of a completely different cohort of patients, it can be expected that differences in outcome are found. We find a strong relationship between diagnosis of ipsilateral thalamic diaschisis neurological performance after stroke and three months later. These findings are in concordance with findings in other types of diaschisis.
CONCLUSION
Presence of ipsilateral thalamic diaschisis in stroke patients, detected using BOLD-CVR, is characterized by thalamic volume reduction, reduced thalamic blood flow, and worse stroke severity scores at admission as well as 3 months follow-up. This finding suggests that ipsilateral thalamic diaschisis may be an important clinical imaging marker in stroke patients.Acknowledgements
No acknowledgement found.References
1. Finger S, Koehler PJ, Jagella C. The Monakow Concept of Diaschisis. Archives of neurology. 2004;61.
2. Baron JC, Bousser MG, Comar D, Castaigne P. "Crossed cerebellar diaschisis" in human supratentorial brain infarction. Transactions of the American Neurological Association. 1981;105:459-61.
3. De Reuck J, Decoo D, Lemahieu I, Strijckmans K, Goethals P, Van Maele G. Ipsilateral thalamic diaschisis after middle cerebral artery infarction. Journal of the neurological sciences. 1995 Dec;134(1-2):130-5.
4. Sakashita Y, Matsuda H, Kakuda K, Takamori M. Hypoperfusion and vasoreactivity in the thalamus and cerebellum after stroke. Stroke; a journal of cerebral circulation. 1993 Jan;24(1):84-7.
5. Sobesky J, Thiel A, Ghaemi M, et al. Crossed cerebellar diaschisis in acute human stroke: a PET study of serial changes and response to supratentorial reperfusion. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2005 Dec;25(12):1685-91.
6. Reidler P, Thierfelder KM, Fabritius MP, et al. Thalamic Diaschisis in Acute Ischemic Stroke: Occurrence, Perfusion Characteristics, and Impact on Outcome. Stroke; a journal of cerebral circulation. 2018 Apr;49(4):931-7.
7. De Reuck J, Decoo D, Lemahieu I, Strijckmans K, Goethals P, Van Maele G. Crossed cerebellar diaschisis after middle cerebral artery infarction. Clinical neurology and neurosurgery. 1997 Feb;99(1):11-6.
8. Kim SE, Choi CW, Yoon BW, et al. Crossed-cerebellar diaschisis in cerebral infarction: technetium-99m-HMPAO SPECT and MRI. Journal of nuclear medicine : official publication, Society of Nuclear Medicine. 1997 Jan;38(1):14-9.
9. Kamouchi M, Fujishima M, Saku Y, Ibayashi S, Iida M. Crossed cerebellar hypoperfusion in hyperacute ischemic stroke. Journal of the neurological sciences. 2004 Oct 15;225(1-2):65-9.
10. Komaba Y, Mishina M, Utsumi K, Katayama Y, Kobayashi S, Mori O. Crossed cerebellar diaschisis in patients with cortical infarction: logistic regression analysis to control for confounding effects. Stroke. 2004 Feb;35(2):472-6.
11. Liu Y, Karonen JO, Nuutinen J, Vanninen E, Kuikka JT, Vanninen RL. Crossed cerebellar diaschisis in acute ischemic stroke: a study with serial SPECT and MRI. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2007 Oct;27(10):1724-32.
12. Strother MK, Anderson MD, Singer RJ, et al. Cerebrovascular collaterals correlate with disease severity in adult North American patients with Moyamoya disease. AJNR American journal of neuroradiology. 2014 Jul;35(7):1318-24.
13. Chalela JA, Alsop DC, Gonzalez-Atavales JB, Maldjian JA, Kasner SE, Detre JA. Magnetic resonance perfusion imaging in acute ischemic stroke using continuous arterial spin labeling. Stroke. 2000 Mar;31(3):680-7.
14. Kang KM, Sohn CH, Choi SH, et al. Detection of crossed cerebellar diaschisis in hyperacute ischemic stroke using arterial spin-labeled MR imaging. PloS one. 2017;12(3):e0173971.
15. Sebök M, Van Niftrik CHB, Piccirelli M, et al. BOLD cerebrovascular reactivity as a novel marker for crossed cerebellar diaschisis. Neurology. 2018(91):1-10.
16. van Niftrik CH, Piccirelli M, Bozinov O, et al. Fine tuning breath-hold-based cerebrovascular reactivity analysis models. Brain Behav. 2016 Feb;6(2):e00426.
17. van Niftrik CHB, Piccirelli M, Bozinov O, et al. Iterative analysis of cerebrovascular reactivity dynamic response by temporal decomposition. Brain Behav. 2017 Sep;7(9):e00705.
18. Kuhl DE, Phelps ME, Kowell AP, Metter EJ, Selin C, Winter J. Effects of stroke on local cerebral metabolism and perfusion: mapping by emission computed tomography of 18FDG and 13NH3. Ann Neurol. 1980 Jul;8(1):47-60.
19. Wise RJ, Bernardi S, Frackowiak RS, Legg NJ, Jones T. Serial observations on the pathophysiology of acute stroke. The transition from ischaemia to infarction as reflected in regional oxygen extraction. Brain : a journal of neurology. 1983 Mar;106 (Pt 1):197-222.
Figures
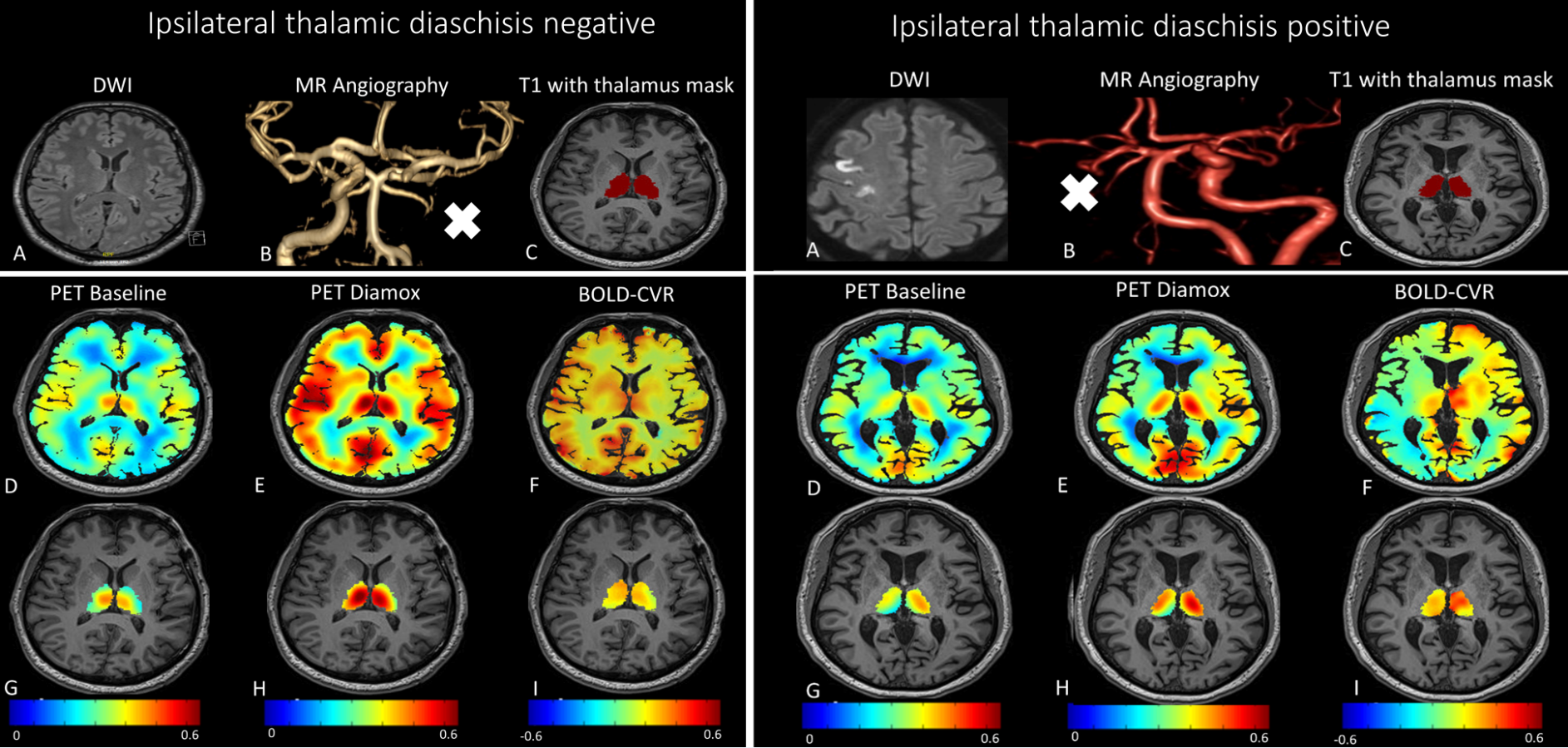
Patient without ipsilateral thalamic diaschisis versus patient with ipsilateral thalamic diaschisis
ITD-negative: Patient with ICA occlusion (white cross) had none lasting symptoms. On PET and BOLD-CVR imaging, signs of left-sided supratentorial hemodynamic impairment is seen in MCA territory. (Figure A-G, A-H and A-I) no ITD can be appreciated for all imaging modalities.
ITD-positive: Patient with right ICA occlusion (white cross) presented left-sided hemiparesis (NIHSS 6/42, mRS 3). Three months later, he experienced neurological improvement (NIHSS 2/42, mRS 1). For all imaging modalities, ITD can be appreciated with a decrease in both BOLD-CVR and PET-CBF on the left side.