2739
Crossed cerebellar diaschisis characterization with BOLD-fMRI cerebrovascular reactivity and T2*-perfusion MRI1University Hospital Zurich, Zurich, Switzerland
Synopsis
Crossed cerebellar diaschisis (CCD) in stroke patients has been associated with worse neurological performance and outcome, but clinical routine CCD imaging is limited. We therefore tested the diagnostic value of blood oxygenation-level dependent cerebrovascular reactivity (BOLD-CVR) and T2* perfusion weighted-MRI in patients with unilateral symptomatic cerebrovascular steno-occlusive disease exhibiting crossed cerebellar diaschisis. Secondly, we assessed the clinical significance of a CCD diagnosis based on BOLD-CVR imaging. BOLD-CVR is a valid clinical diagnostic tool for CCD, whereas perfusion MRI derived parameters were shown to be unsuitable. Furthermore, stroke patients exhibiting CCD showed a worse neurological performance and outcome, unrelated to stroke volume.
INTRODUCTION
Crossed cerebellar diaschisis (CCD) in stroke patients has been associated
with worse neurological performance and outcome, but clinical routine CCD imaging
is limited. We therefore tested the diagnostic value of blood
oxygenation-level dependent cerebrovascular reactivity (BOLD-CVR) and T2* perfusion
weighted-MRI in patients with unilateral symptomatic cerebrovascular
steno-occlusive disease exhibiting crossed cerebellar diaschisis. Secondly, we assessed the clinical
significance of a CCD diagnosis based on BOLD-CVR imaging.METHODS
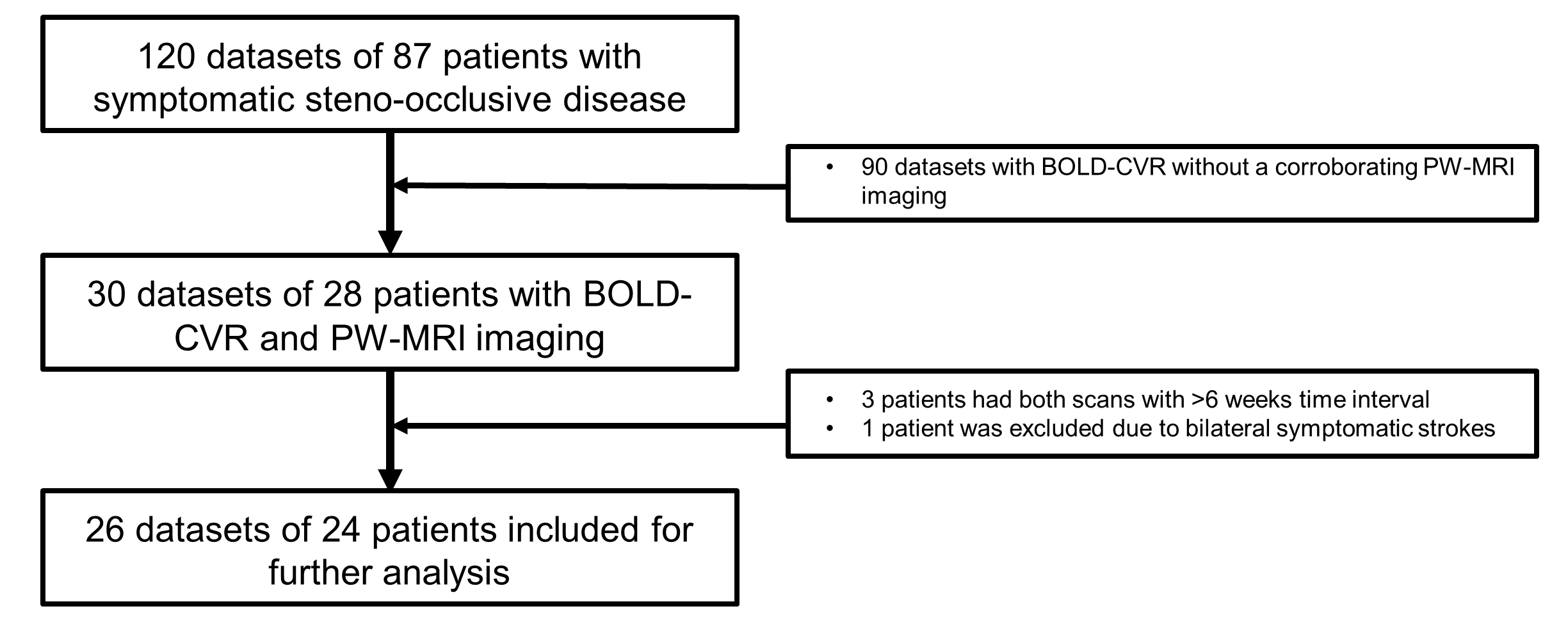
Twenty-six datasets of subjects with unilateral symptomatic cerebrovascular steno-occlusive disease underwent a BOLD-CVR and perfusion-weighted MR study. Further details on the setup have been described in previous publications1, 2. Iterative temporal decomposition of the BOLD-CVR data was used to avoid transient phases confounds. CCD was deferred from BOLD-CVR using a predetermined cerebellar asymmetry index cut-off value of 6.0. As a comparison CCD was also diagnosed using qualitative prolonged time-to-peak (TTP) on the contralateral cerebellar hemisphere. Initial stroke volume, as well as neurological status at admission and outcome after 3 months were determined with NIHSS and mRS scores.RESULTS
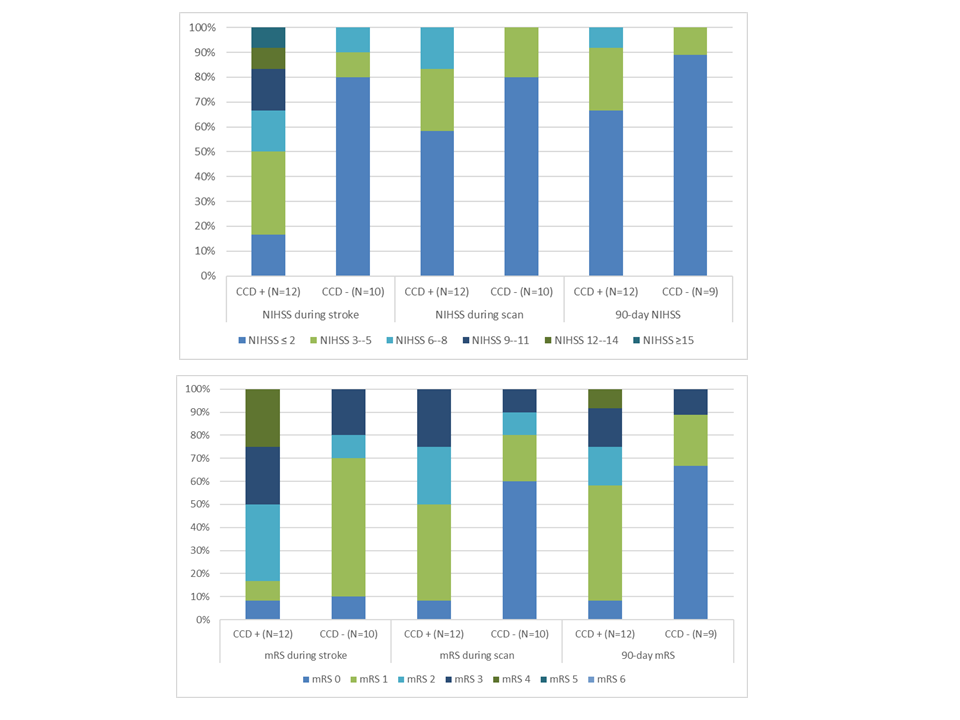
Based on the BOLD-CVR cut-off value, CCD was present in 52% of the study population. No agreement was found between BOLD-CVR and any of the perfusion-weighted MR parameters (i.e. CBF, CBV, MTT, and TTP). BOLD-CVR was strongly associated with poorer clinical performance both at admission as well as after 3 months for CCD subjects (CCD(+) vs. CCD(-): NIHSS: 6 (6) vs. 2 (4), p = 0.002; mRS: 3(2) vs. 1(2), p=0.003). This difference persisted at 3 months follow-up for both scores (NIHSS (2 (4) vs. 0 (2), p = 0.014; mRS 1 (2) vs. 0(1), p=0.006). Using quantitative TTP evaluation, 28% of subjects exhibited CCD. Importantly, diagnosing CCD with TTP did not show any clinical prognostic value.DISCUSSION & CONCLUSION
BOLD-CVR is a valid clinical diagnostic tool for crossed cerebellar diaschisis in subjects with unilateral symptomatic steno-occlusive disease, whereas perfusion MRI derived parameters were shown to be unsuitable. Furthermore, stroke patients exhibiting CCD showed a worse neurological performance and outcome, unrelated to stroke volume. Interestingly, the BOLD signal changes found in patients with CCD is an encouraging finding for future studies on neuronal metabolism, activity and blood flow control.Acknowledgements
No acknowledgement found.References
1. van Niftrik CHB, Piccirelli M, Bozinov O, Pangalu A, Fisher JA, Valavanis A, et al. Iterative analysis of cerebrovascular reactivity dynamic response by temporal decomposition. Brain Behav. 2017;7:e00705
2. van Niftrik CH, Piccirelli M, Bozinov O, Pangalu A, Valavanis A, Regli L, et al. Fine tuning breath-hold-based cerebrovascular reactivity analysis models. Brain Behav. 2016;6:e00426
Figures
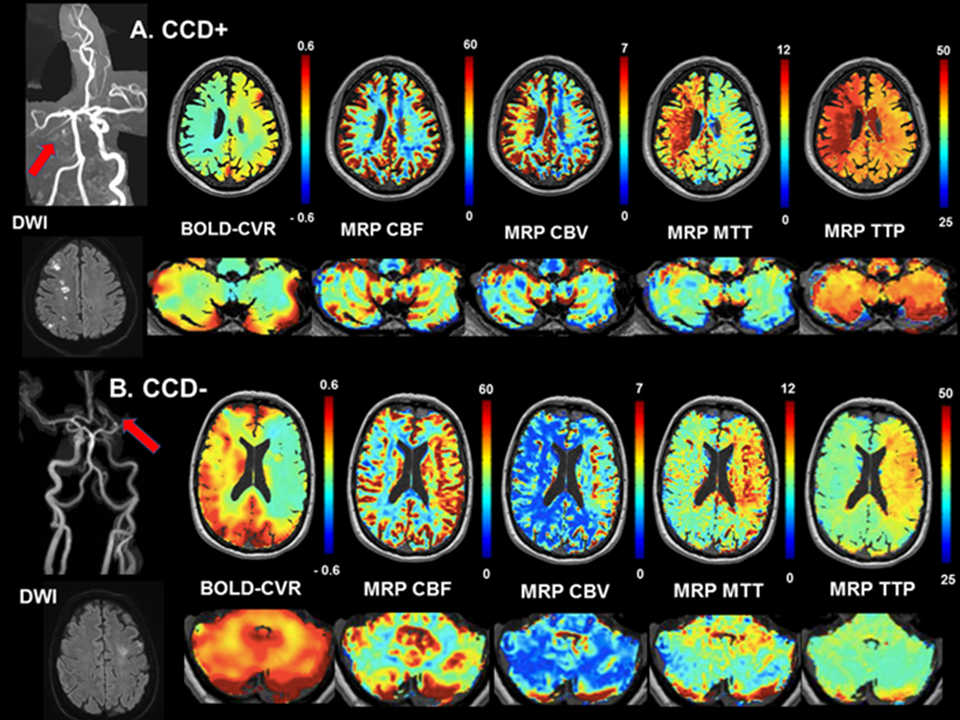
A: Subject, with left ICA occlusion (red arrow), presented with right-sided hemiparesis and ataxia (NIHSS 4/42, mRS 2). On BOLD-CVR and PW-MRI imaging, clear supratentorial hemodynamic impairment and cerebellar asymmetric BOLD-CVR is seen (white triangle) i.e. crossed cerebellar diaschisis. After three months, his hemiparesis improved (NIHSS 2/42, mRS 1).
B: Subject, with left MCA occlusion (red arrow), presented with a right sided facial asymmetry (NIHSS 1/42, mRS 2), which resolved quickly and had no neurological symptoms after three months (NIHSS 0/42, mRS 0). PW-MRI as well as BOLD-CVR show supratentorial hemodynamic impairment (white triangle), whereas no crossed cerebellar diaschisis is observed.