Manabu Shirakawa1, Li Chen2, Niranjan Balu1, Wenjin Liu1, Dakota Ortega1, Jinmei Chen1, Theodore Trouard3, Diane Bock4, Wei Zhou4, Chun Yuan1, and Thomas S Hatsukami5
1Radiology, University of Washington, Seattle, WA, United States, 2Electrical Engineering, University of Washington, Seattle, WA, United States, 3Biomedical Engineering, University of Arizona, Tuscon, AZ, United States, 4Surgery, University of Arizona, Tuscon, AZ, United States, 5Surgery, University of Washington, Seattle, WA, United States
Synopsis
The aim is to evaluate the change in intracranial
arterial vasculature after carotid revascularization using an intracranial feature
extraction (iCafe) technique for quantitative analysis of intracranial arteries
from 3D time-of-flight magnetic resonance angiography (TOF MRA). Twenty subjects
who received carotid revascularization were enrolled and all patients underwent
MRA scans three times: before, within 3 days after, and six months after revascularization.
The dataset was processed blindly by 4 reviewers using iCafe. Length and volume
of intracranial artery and number of intracranial artery branches increased
after surgery. This result suggested increased cerebral blood flow after
carotid revascularization.
Introduction
Cerebral blood flow increases after carotid
revascularization1,2. In some individuals, persistent hyperperfusion
may lead to headache, seizure, or intracranial hemorrhage, and carries a poor
prognosis. In others, increased perfusion following revascularization may be
associated with improvement in cognitive function3. Further
investigation into the pathophysiology and mechanisms of change in intracranial
vasculature after carotid revascularization is needed to better differentiate
patients with poor prognosis from those who will benefit from intervention. The
paucity of reproducible, quantitative assessment tools is a major barrier to
such studies.
An intraCranial artery feature extraction
(iCafe) technique, which semi-automatically evaluates vessel structure from 3D
TOF MRA images4 could provide quantitative information about changes
in vasculature. A 3D quantitative vasculature map can be generated from iCafe and
morphometry features of intracranial arteries can be
extracted, such as length and radius of arteries.
In this study, we analyzed intracranial artery
structures from a group of patients at three timepoints using iCafe to evaluate
the change of intracranial vasculature after carotid revascularization.Methods
The study followed local IRB guidelines and
informed consent was obtained for all patients prior to enrollment. Twenty subjects
who received carotid revascularization were scanned at three timepoints (pre and
post intervention and 6 months after the procedure). 3D TOF MRA images were acquired
on 3.0T GE scanner. Imaging parameters were as follows: TR/TE = 25/3.5 ms, flip
angle = 20°, in-plane resolution = 0.35mm×0.35 mm, slice thickness = 1.4 mm,
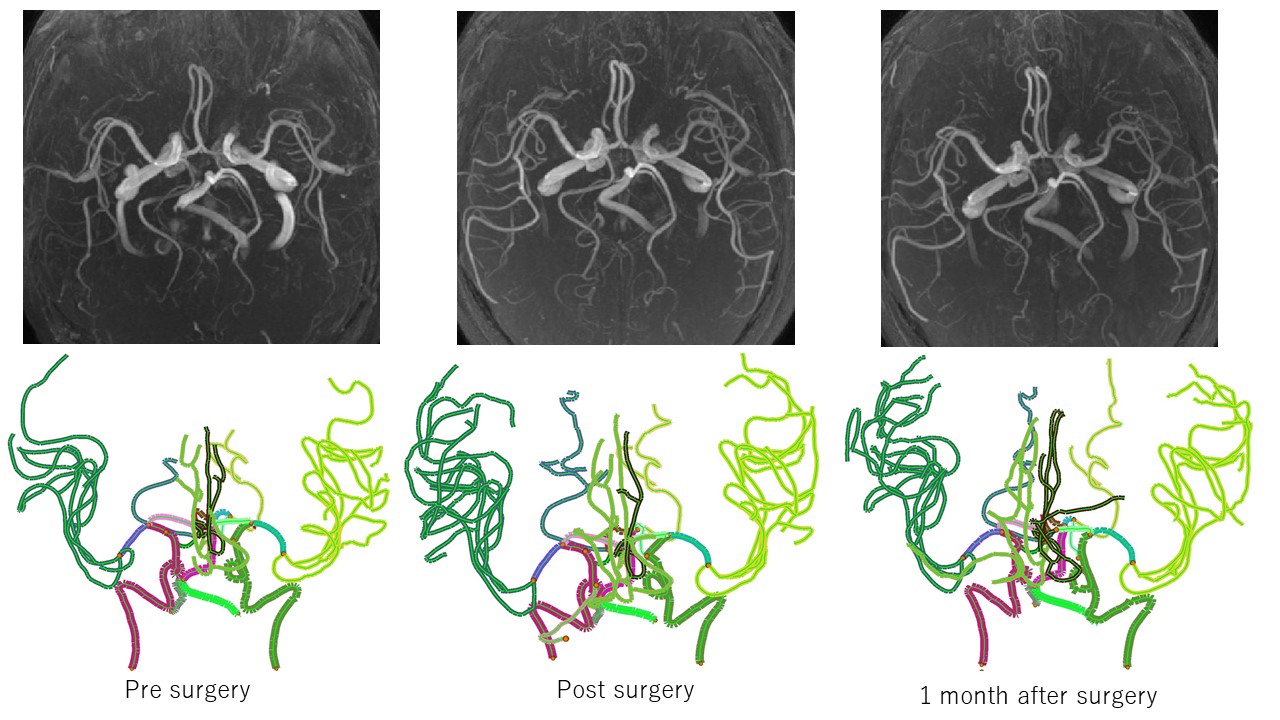
matrix = 376*277. Four readers reviewed the MRA images using iCafe and one examiner
then peer-reviewed their results. Each reviewer conducted processing of
all timepoints of one subject throughout to reduce inter-rater bias. A representative
case is shown in Figure 1. We analyzed length and volume of total arteries,
the right and left side of anterior circulation arteries, radius of the internal
carotid and M1 segment of middle cerebral arteries. Paired Wilcoxson test was used to assess the difference of
features in each timepoint. P<0.05 was considered as statistically
significant without adjustment for the number of comparisons. Jmp 13 was used
for the statistical analysis.Results
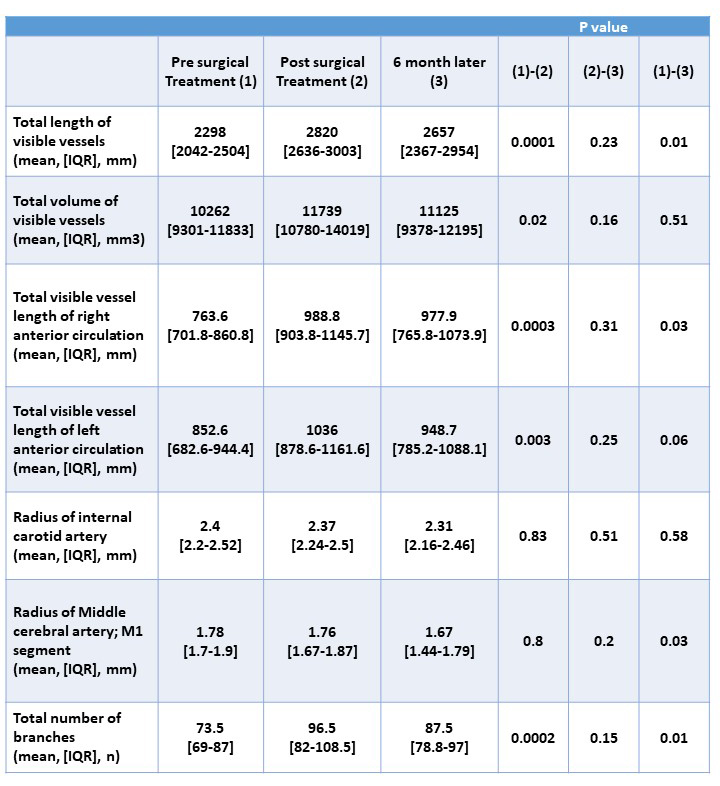
Table 1 shows a summary of our findings. The total
vessel length and volume of intracranial artery increased after the surgical
treatment compared to pre treatment (2298 mm vs. 2820 mm, 10262 mm3 vs.
11739 mm3 p=0.0001, 0.02, respectively). However, the length of
vessels six months after surgical treatment was shorter compared to
post-surgical treatment (2820 mm vs. 2657 mm, p=0.01), although the volume was unchanged
(11739 mm3 vs. 11125 mm3, p=0.51). The length of intracranial arteries in both
left and right sides post treatment was longer than before treatment. (852.6 mm
vs 1036 mm, 763.6 mm vs 988.8 mm, p=0.003, 0.003). The radius of the internal
carotid and middle cerebral arteries was unchanged across the three time points,
while radius of M1 segment decreased six months after treatment (1.78 mm vs.
1.67 mm, p=0.03). The numbers of branches of intracranial arteries increased
post revascularization (73.5 vs. 96.5, 87.5, p=0.0002, 0.01).Discussion
Findings of this study are consistent with
increased intracranial blood flow just after the carotid revascularization in
both ipsilateral and contralateral hemispheres based on the increase of length,
volume and the number of the branches measured with iCafe. This is the first
report that provides quantitative MRA assessment with iCafe for evaluating the
influence of carotid revascularization on intracranial vascular structure. These
findings demonstrate the potential for utilizing conventional, widely utilized
clinical imaging techniques (MRA), and a semi-automated, objective image
analysis tool (iCafe) in studies to examine the association between
intracranial arterial structure, changes with revascularization, and its effect
on cognitive function.Conclusion
We found that there were significant changes in intracranial vessel length and the number of intracranial vessel branches after carotid revascularization using iCafe. This study also demonstrates the potential future application of iCafe for assessing cerebral blood flow changes after vascular reconstruction.Acknowledgements
This research is supported by grants from the National Institutes of Health (R01NS070308).References
1. Waaijer A, van Leeuwen MS, van
Osch MJ, et al. Changes in cerebral perfusion after revascularization of
symptomatic carotid artery stenosis: CT measurement. Radiology 2007;245:541-8.
2. Sadato A, Maeda S, Hayakawa M,
et al. Carotid stenting for unilateral stenosis can increase contralateral
hemispheric cerebral blood flow. J Neurointerv Surg 2018;10:351-4.
3. Galyfos G, Sianou A, Filis K.
Cerebral hyperperfusion syndrome and intracranial hemorrhage after carotid endarterectomy
or carotid stenting: A meta-analysis. J Neurol Sci 2017;381:74-82.
4. Chen L, Mossa-Basha M, Balu N,
et al. Development of a quantitative intracranial vascular features extraction
tool on 3D MRA using semiautomated open-curve active contour vessel tracing.
Magn Reson Med 2018;79:3229-38.