2737
The optimization of single-shot FLAIR for motion artifact reduction and scan time reduction in stroke imaging: A Comparative Analysis with Conventional FLAIR1Radiology, Chiba university hospital, Chiba city, Japan, 2Radiology, Eastern Chiba Medical Center, Togane city, Japan, 3Division of Health Sciences, Graduate School of Medical Sciences, Kanazawa university, Kanazawa, Japan, 4Philips Japan, Tokyo, Japan, 5Department of Diagnostic Radiology and Radiation Oncology, Chiba University Graduate School of Medicine, Chiba city, Japan
Synopsis
For stroke imaging, motion correction and scan time reduction are essential. We optimized the single-shot FLAIR sequence and implemented it into our stroke MR protocol. 48 patients suspected of stroke were retrospectively involved, and board-certified radiologists evaluated the images of our modified-single-shot FLAIR and conventional FLAIR at the terms of degree of motion artifact, image quality, delineation of hyperintense vessel and contribution for diagnosis. Motion artifact was significantly reduced (P < 0.001) and scan time was decreased by 40% in single-shot FLAIR. Hyperintense vessels were equally detected in both the sequences. Radiologists considered modified-single-shot FLAIR more useful for diagnosis.
INTRODUCTION
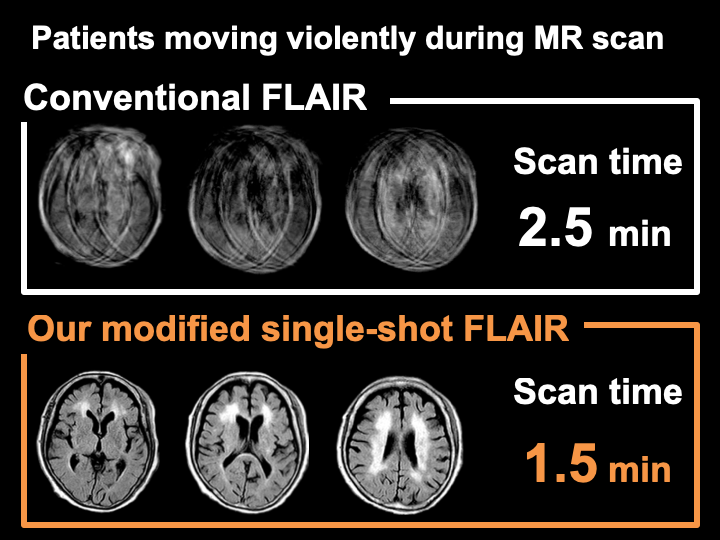
FLAIR imaging, as a key sequence along with DWI in acute MR protocol, has the potential to detect subtle hemorrhage, to describe the intra-arterial clot, to delineate the region of infarction, and to help to estimate, in the combination of DWI, the onset of acute cerebral stroke (especially useful in so-called wake-up stroke). Motion correction of brain MR imaging in moving patients while shortening the scan time is still challenging but potentially necessary for evaluation of patients suspected of acute cerebral infarction. The single-shot FLAIR sequence, as a faster variant of T2-FLAIR sequences, is useful with short scan time and with the potential to be less degraded by motion artifact. However, when patients moving violently, the high signal of CSF artifacts can occur in this sequence. To resolve this problem, we optimized the single-shot FLAIR with wide IR pulse and implemented it into our stroke MR protocol. The aim of our study was to compare our single-shot FLAIR sequence and conventional FLAIR sequence with three different approaches: (1) comparing the image contrast by calculating the contrast-ratio in the patients with no motion artifact (motion (-) group), (2) comparing the extent of motion artifact in the patients who moved while data acquisition (motion (+) group) and (3) evaluating the presence and extent of hyperintense vessel, overall image quality and contribution for diagnosis in motion (-) and (+) groups.METHODS
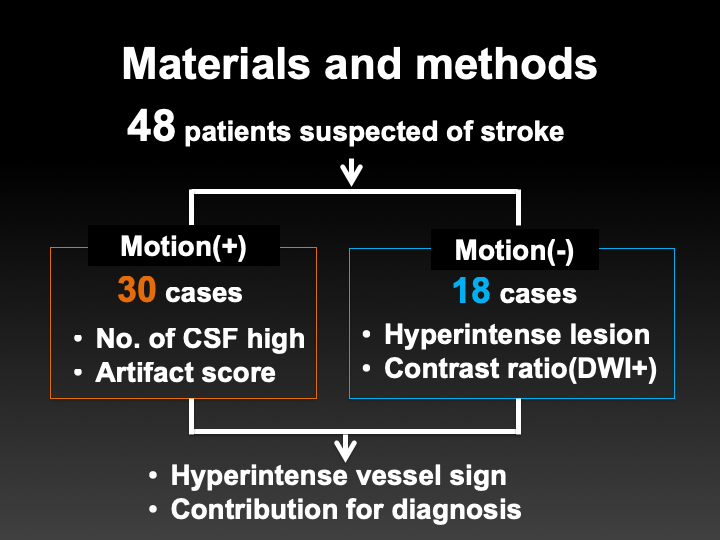
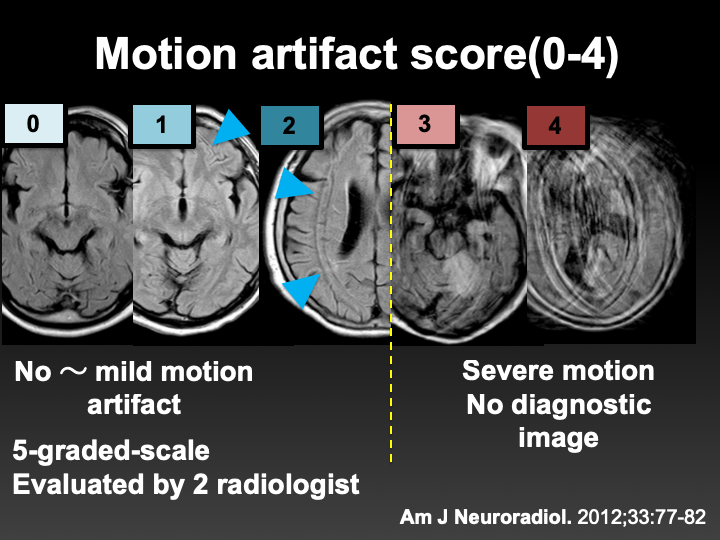
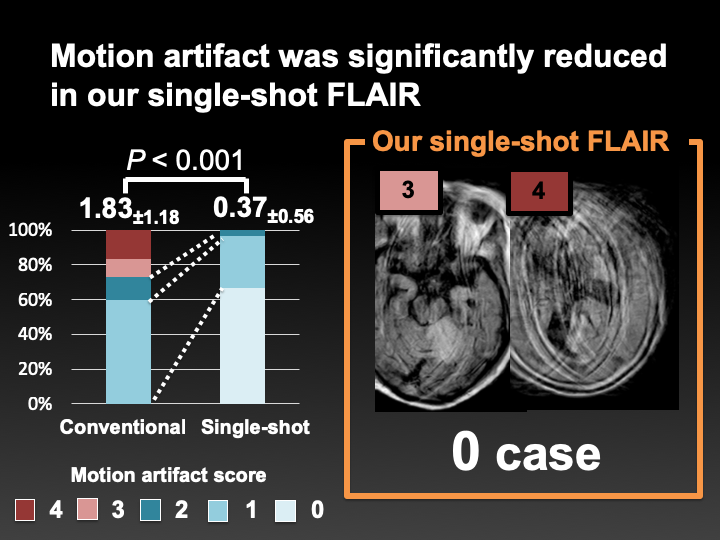
Forty-eight consecutive patients (age, 69.7 ± 19.4 years) considered acute ischemic stroke were involved in this study. Both conventional FLAIR (con-FLAIR; acquisition time, 2.5 minutes) and our modified-single-shot FLAIR (SS-FLAIR; 1.5 minutes) were acquired in all the cases. Motion artifact was assessed using the 5-grade scale: 0, no artifact; 1, mild artifact with mild degradation of the image quality; 2, visible artifact with moderate degradation; 3, visible artifact with severe degradation; 4, visible artifact with no diagnostic value. The number of visible lesions with hyperintensity on FLAIR image was counted on con-FLAIR and SS-FLAIR independently. The existence of high signal artifact in CSF on SS-FLAIR was evaluated. Hyperintense vessels on FLAIR were also assessed. To evaluate the reliability of SS-FLAIR compared with con-FLAIR, contrast ratios of diffusion-restricted lesions were calculated on conventional FLAIR and single-shot FLAIR in cases without motion artifact. Finally, to evaluate diagnosis contribution, two radiologists determined which image set provided more useful information for diagnosis. All image analysis was performed by 2 board-certified radiologists (with 8 and 14 years of experience in neuroimaging). Each MR image was randomly evaluated in an independent fashion. Each reviewer was blinded to the patients’ information and acquisition parameters of images. The Mann-Whitney U test and paired t-test were used for the statistical analysis. A two-sided value of P < 0.05 was considered significant.RESULTS
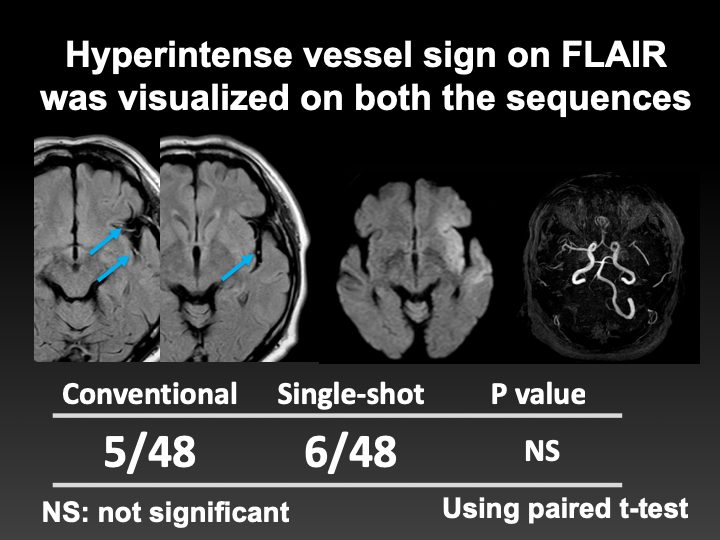
SS-FLAIR reduced motion artifact significantly (P < 0.001) and revealed more lesion than con-FLAIR (P = 0.001). In 6 and 5 of 48 patients, hyperintense vessels due to arterial occlusion were visualized on our single-shot FLAIR and conventional FLAIR, respectively. The high signals of CSF were not detected in our single-shot FLAIR. Although signal contrasts of the DWI hyperintense lesions were significantly decreased (P = 0.005), two radiologists considered single-shot FLAIR more useful for diagnosis in 9 cases with consensus. The residual 38 cases were scored as equivalent.DISCUSSION
Although the contrast ratio was decreased on single-shot FLAIR, the degradation of the image quality was small and had a small influence on diagnosis. The motion artifact was dramatically reduced and the acquisition time was significantly reduced. CSF artifact was not seen in our single-shot FLAIR. Therefore, our single-shot FLAIR with potential scan time reduction provided more useful information to diagnose acute ischemic stroke than conventional-FLAIR. Several motion correction techniques are available now. However, PROPELLER, the scheme for modified radial acquisition in k-space based on the multishot TSE sequence, tends to extend total data acquisition time, and the limitation of motion correction still exists. An echo-planar fluid-attenuated inversion recovery (EPI-FLAIR) sequence is useful to shorten the scan time but leads to distorting the images. Our new technique of SS-FLAIR with wide IR pulse has a potential to resolve these weak points.CONCLUSION
Our modified single-shot fluid-attenuated inversion recovery (FLAIR) was feasible with comparable qualitative and quantitative results to conventional FLAIR. Our sequence reduced scan time and motion artifact dramatically and provided more useful information for diagnosing acute ischemic stroke.Acknowledgements
No acknowledgement found.References
1.Thomalla G, Rossbach P, Rosenkranz M, et al. Negative fluid-attenuated inversion recovery imaging identifies acute ischemic stroke at 3 hours or less. Ann Neurol. 2009;65(6):724-32.
2.Meshksar A, Villablanca JP, Khan R, et al. Role of EPI-FLAIR in patients with acute stroke: a comparative analysis with FLAIR. AJNR Am J Neuroradiol. 2014;35(5):878-83.
3.Nyberg E, Sandhu GS, Jesberger J,et al. Comparison of brain MR images at 1.5T using BLADE and rectilinear techniques for patients who move during data acquisition. AJNR Am J Neuroradiol. 2012;33(1):77-82.
Figures