2736
The value of different plaque indicators in predicting stroke1Department of Radiology, Henan Provincial People's Hospital, Zhengzhou, China, 2Henan Key Laboratory for Medical Imaging of Neurological Diseases, Zhengzhou, China, 3MR Collaboration, Siemens Healthcare Ltd., Beijing, China, 4Cooperative Innovation Center of Internet Healthcare & School of Software and Applied Technology, Zhengzhou University, Zhengzhou, China
Synopsis
Emerging evidence suggests that the characteristics of intracranial plaques detected by high-resolution vessel wall imaging may serve as an important in-vivo biomarker for predicting ischemic stroke. Different indicators have been introduced to depict plaque features, such as remodeling index, contrast enhancement, and stenosis rate. The purpose of this study was to comprehensively assess the diagnostic performance of these indicators by a quantitative comparison between ischemic stroke patients and transient-ischemic-attack patients. Our results indicated that the remodeling index may have a predictive power similar to contrast enhancement while stenosis rate was a poor predictor.
Introduction
Intracranial atherosclerosis disease (ICAD) is the leading cause of ischemic stroke worldwide.1 Increasing evidence shows that plaque characteristics and not the degree of stenosis by itself are important determinants of stroke events.2 Recent studies utilizing 3D high-resolution vessel wall imaging (HRVWI) have depicted intracranial plaque characteristics in-vivo and have concluded that different indicators, such as remodeling index and contrast enhancement are sensitive biomarkers for ischemic stroke. However, few studies have comprehensively evaluated the performance of these indicators. This study aims to assess the diagnostic performance of these indicators by quantitatively comparing plaque and stenosis characteristics between ischemic-stroke patients and transient-ischemic-attack patients.Method
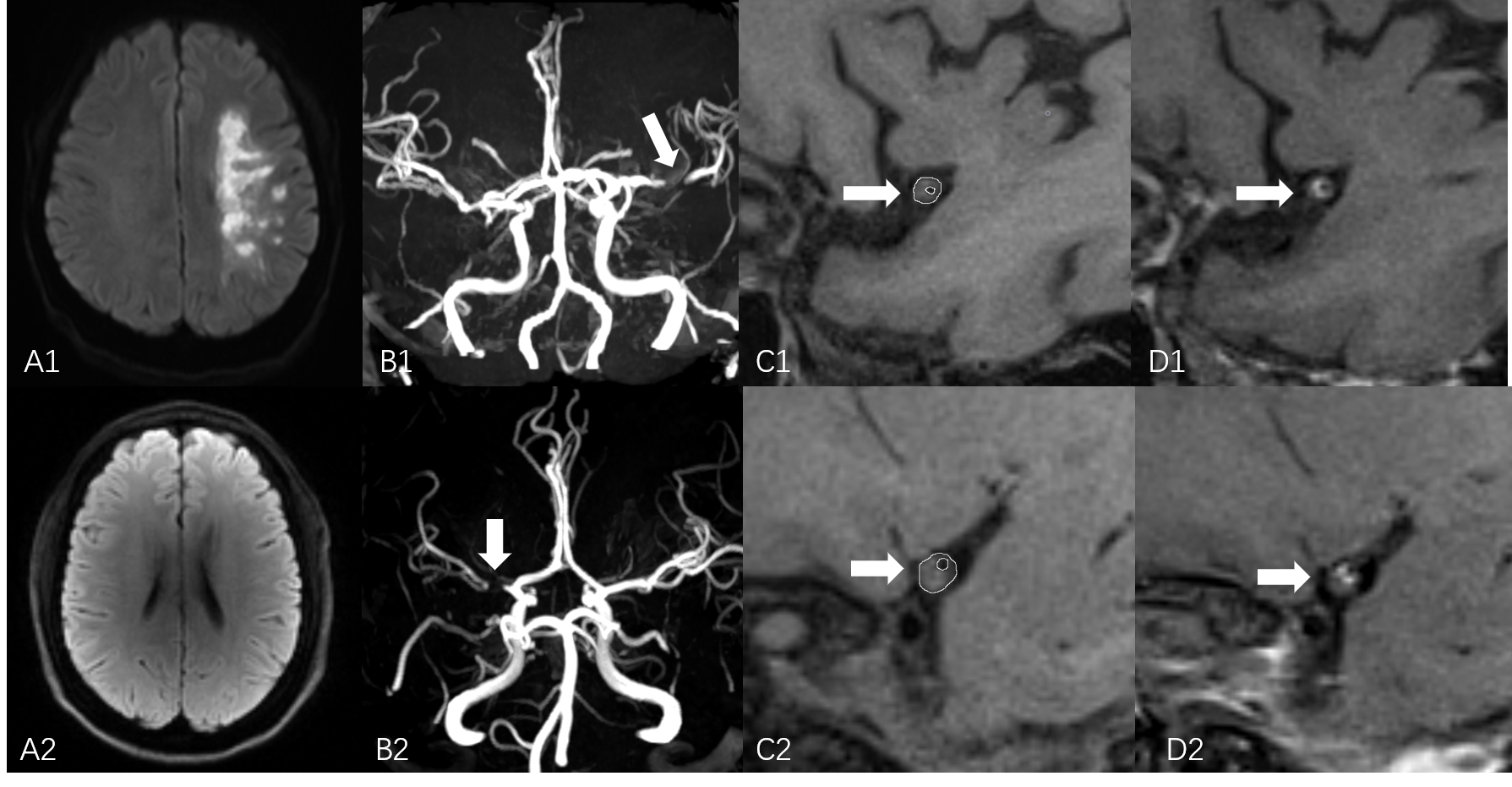
A total of 51 patients with symptomatic middle cerebral artery (MCA) stenosis were enrolled in this study. 20 patients (Age: 51±9 years,14 males) with hyperintense signal on DWI in the territory of the MCA were assigned to the stroke group, and the remaining 31 patients (Age: 48±8 years,21 males) without hyperintense signal on DWI were assigned to the transient ischemic attack (TIA) group.
All patients underwent TOF-MRA imaging as well as pre- and post-contrast vessel wall imaging within 2 weeks after symptom onset on a 3T MAGNETOM Prisma MR scanner (Siemens Healthcare, Erlangen, Germany) with a 64-channel head coil. The 3D vessel wall images were acquired using a 3D SPACE sequence with the following parameters: TR/TE=900ms/14.0ms, slices=224, voxel size=0.53x0.53x0.53mm3, TA=8:29min.
Based on the vessel wall images, stenosis rate, remodeling index and contrast enhancement were calculated by referring to the work of Wang et al. 3 and Qiao et al. 4 .The lesion was defined as the narrowest part of the artery, with distal normal vessel segment adjacent to the lesion as a reference. The stenosis rate (SR) was calculated as: SR= (1 – lesion lumen area/reference lumen area) x100%. The remodeling index (RI) was defined as: RI = lesion vessel area/reference vessel area. The plaque contrast enhancement (CE) was quantified by: CE = (Spost - Spre)/Spre, where Spost is the normalized signal intensity on post-contrast vessel wall images, and Spre is the normalized signal intensity on pre-contrast vessel wall images.
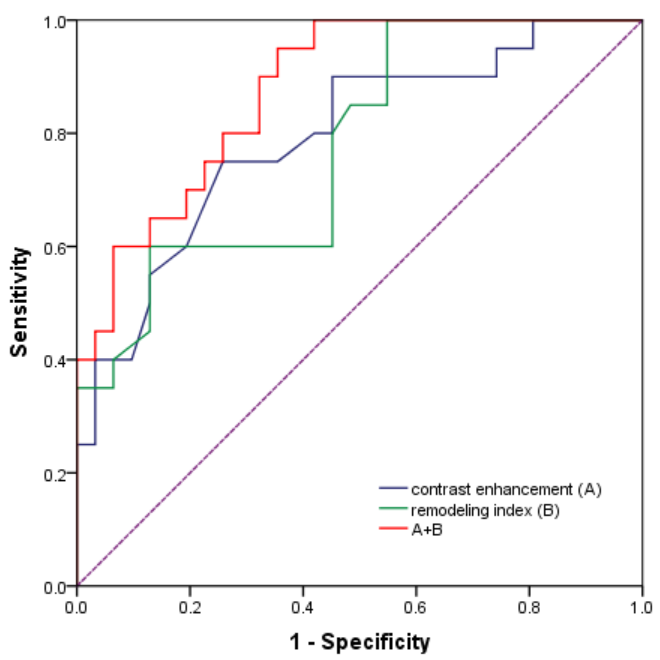
These parameters were compared between the ischemic-stroke group and the TIA group using two sample t-tests. Receiver operating characteristic (ROC) curves were conducted to evaluate the diagnostic performance of each parameter in predicting the occurrence of stroke.
Result
Images of two representative subjects are shown in Figure 1.
The remodeling index (Mean ± Std) and contrast enhancement (Mean ± Std) of the ischemic-stroke group were significantly higher than those in the TIA group (RI: 0.960±0.164 vs. 0.754±0.186, P=0.000; CE: 134±46 vs. 91±37, P=0.001). However, no significant difference was found regarding stenosis rate (Mean ± Std) (70.3%±11.6% vs. 72.2%±15.7%, P=0.646) between these two groups.
The AUC (95% CI) for determining the occurrence of stroke was 0.777 for the remodeling index and 0.794 for contrast enhancement (Figure 2). There was no significant difference in AUC between remodeling index and contrast enhancement (P=0.866). The AUC for combination of remodeling index and contrast enhancement was 0.877.
Discussion
Due to endothelial permeability and increased neovascularization, the degree of enhancement is thought to reflect the level of inflammatory activity in patients with intracranial atherosclerosis.5 Thus, contrast enhancement has always been considered to be the most sensitive indicator for the occurrence of cerebral ischemic events, and our study does not dispute this concept.
However, our results indicate that the remodeling index may be as effective as contrast enhancement in predicting cerebral infarction, as demonstrated by the above ROC analyses and comparable significant differences in CE and RI between the stroke group and TIA group. Our finding regarding RI is in line with previous studies that have shown that a high remodeling index can reduce the stability of a plaque, meaning it is more bioactive and prone to rupture.6 The clinical importance of being able to use RI to accurately predict strokes lies in the fact that RI can be calculated from non-contrast MRI unlike CE, allowing for a less risky diagnostic technique of assessing stroke risk in patients with renal dysfunction.
Conclusion
Based on 3D HRVWI, plaque features can be quantitatively and accurately characterized by both the remodeling index and contrast enhancement, consequently providing effective risk assessment and timely treatment for patients with middle cerebral artery atherosclerosis.Acknowledgements
This research was supported by the NNSFC (81720108021, 81772009,81601466,81641168, 31470047), National Key R&D Program of China (YS2017YFGH000397), Scientific and Technological Research Project of Henan Province (182102310162) and the Key Project of Henan Medical Science and Technology Project (201501011).References
- De Silva DA, Woon FP, et al. South Asian patients with ischemic stroke: intracranial large arteries are the predominant site of disease. Stroke. 2007;38(9):2592-2594.
- Wong KS, Li H, Lam WW, et al. Progression of Middle Cerebral Artery Occlusive Disease and Its Relationship With Further Vascular Events After Stroke. Stroke; a journal of cerebral circulation. 2002;33(2):532-536.
- Wang M, Fang W, Yang Y, et al. Quantitative assessment of symptomatic intracranial atherosclerosis and lenticulostriate arteries in recent stroke patients using whole-brain high-resolution cardiovascular magnetic resonance imaging. Journal of Cardiovascular Magnetic Resonance. 2018;20(1):35.
- Qiao Y, Zeiler S R, Mirbagheri S, et al. Intracranial plaque enhancement in patients with cerebrovascular events on high-spatial-resolution MR images. Radiology. 2014;271(2):534-542.
- Qiao Y, Etesami M, Astor B C, et al. Carotid plaque neovascularization and hemorrhage detected by MR imaging are associated with recent cerebrovascular ischemic events. Ajnr American Journal of Neuroradiology. 2012;33(4):755-760.
- Schoenhagen P, Ziada K M, Kapadia S R, et al. Extent and direction of arterial remodeling in stable versus unstable coronary syndromes : an intravascular ultrasound study. Circulation. 2000;101(6):598-603.
Figures