2735
Age Specific Differences in Association Between White Matter Cerebral Blood Flow and Ischemic Lesion Severity1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University School of Medicine, Beijing, China, 2Department of Radiology, University of Washington, Seattle, WA, United States, 3Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 4China National Clinical Research Center for Neurological Diseases, Beijing, China
Synopsis
White matter lesion (WML), one of the sequelae of cerebral hypoperfusion, accumulates with age. This study sought to investigate the relationship between cerebral blood flow (CBF) and WML severity with age in asymptomatic adults. We found that WML scores were strongly associated with WM CBF, suggesting that WM CBF might be an effective indicator for severity of WMLs. We also found that the WM CBF increased with age, consistent with the greater WM cerebrovascular reactivity response in elderly individuals. In addition, our findings of ascending WM CBF cut-off values revealed that the risk of developing WML increases with age.
Introduction
White matter lesion (WML) is a leading cause of cognitive decline and functional loss in the elderly. Although investigators found that WML is one of the sequelae of cerebral hypoperfusion, its underlying physiological mechanism remains unclear. Since aging is an important risk factor for WMLs, the alterations of cerebral blood flow (CBF) with age may play a role in occurrence of white matter (WM) ischemic lesions. This study aims to investigate the relationship between CBF and WML severity with age in asymptomatic adults.Methods
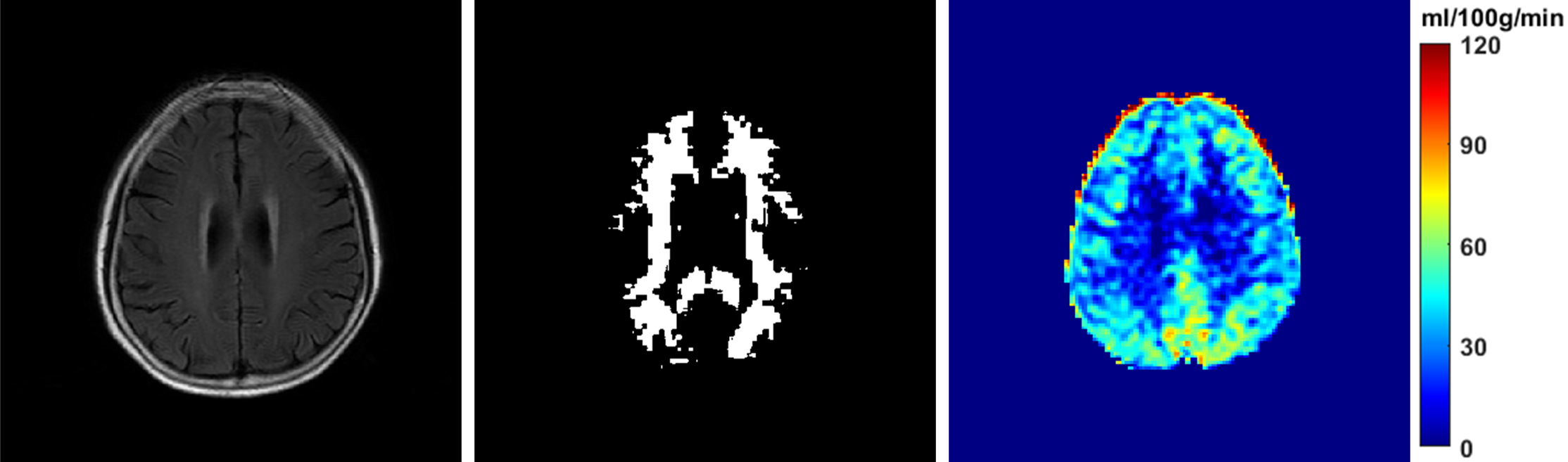
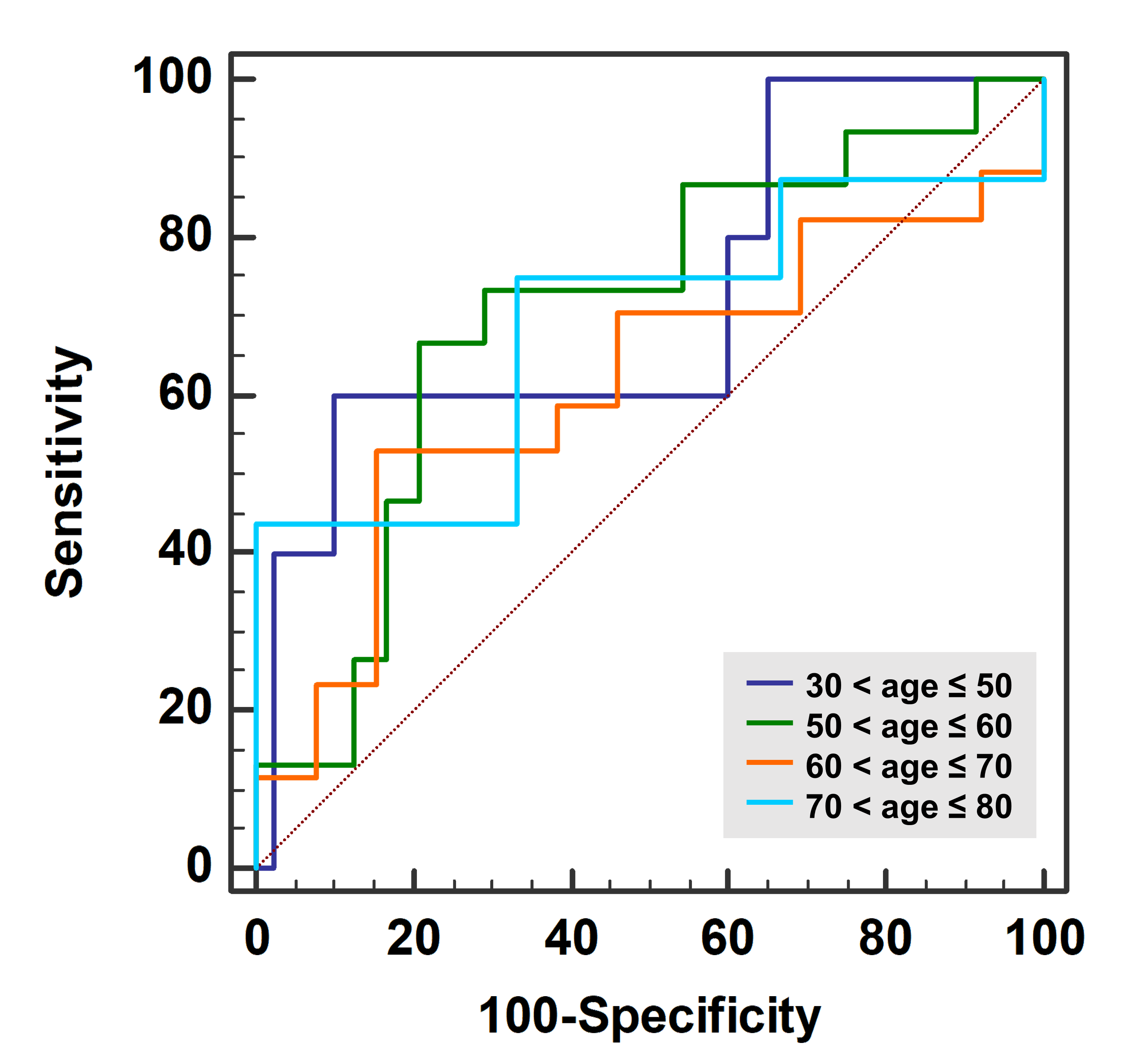
Study sample: A total of 130 subjects (mean age, 55.8±12.8 years; 52 males) were consecutively recruited from an imaging-based community study of CAMERA which aimed to investigate the cerebrovascular disease risk in the asymptomatic adults. MR imaging: After written informed consent was obtained, all recruited subjects aged 30 to 80 years underwent brain imaging on a 3T MR scanner (Achieva TX, Philips Healthcare, Best, The Netherlands) equipped with a 32-channel head coil to acquire the following sequences: pseudo-continuous arterial spin labeling (pCASL): labeling duration 1650 ms, post labeling delay 1575 ms, 2D EPI readout with 90° excitation RF pulse, TR/TE 4016/12 ms, FOV 240×240×132 mm3, spatial resolution 3×3×6 mm3, SENSE acceleration factor 3, number of averages 30, background suppression; and T2-FLAIR: inversion recovery, TR/TI 7000/2200 ms, TE 140 ms, FOV 230×230×133 mm3, spatial resolution 0.9×0.9×5.5 mm3. Image analysis: The CBF was calculated using the pCASL images and proton density-weighted images (M0) with motion correction. Tissue segmentation was performed to derive binary masks representing territorial CBF. The WM binary mask was created from T2-FLAIR and co-registered to CBF maps using the Matlab-based SPM12 toolbox (Wellcome Trust, England). The WML mask was manually edited and modified for segmenting the whole compartments of WML and the normal appearing white matter (NAWM) using CASCADE software (University of Washington, Seattle, USA). The WMLs were scored independently by two experienced raters from 0 for normal to 9 for most severe and were then classified into normal to mild grade (score ≤1) and moderate to severe grade (score ≥2). An example of MR images and binary WM segmentation mask is shown in Fig. 1. Statistical analysis: The Spearman correlation analysis was used to estimate the association between age and WML score. Spearman’s correlations were utilized to determine the associations of the CBF of WM, WMLs and NAWM with WML score in 4 different age groups (≤50 years, 50-60 years, 60-70 years, and >70 years). Receiver–operator curves (ROC) analyses were conducted to calculate the area-under-the-curve (AUC) of WM CBF and the optimal CBF cut-off-value (corresponding to the highest likelihood ratio of ROC curves) in differentiating the severity of WML among different age groups.Results
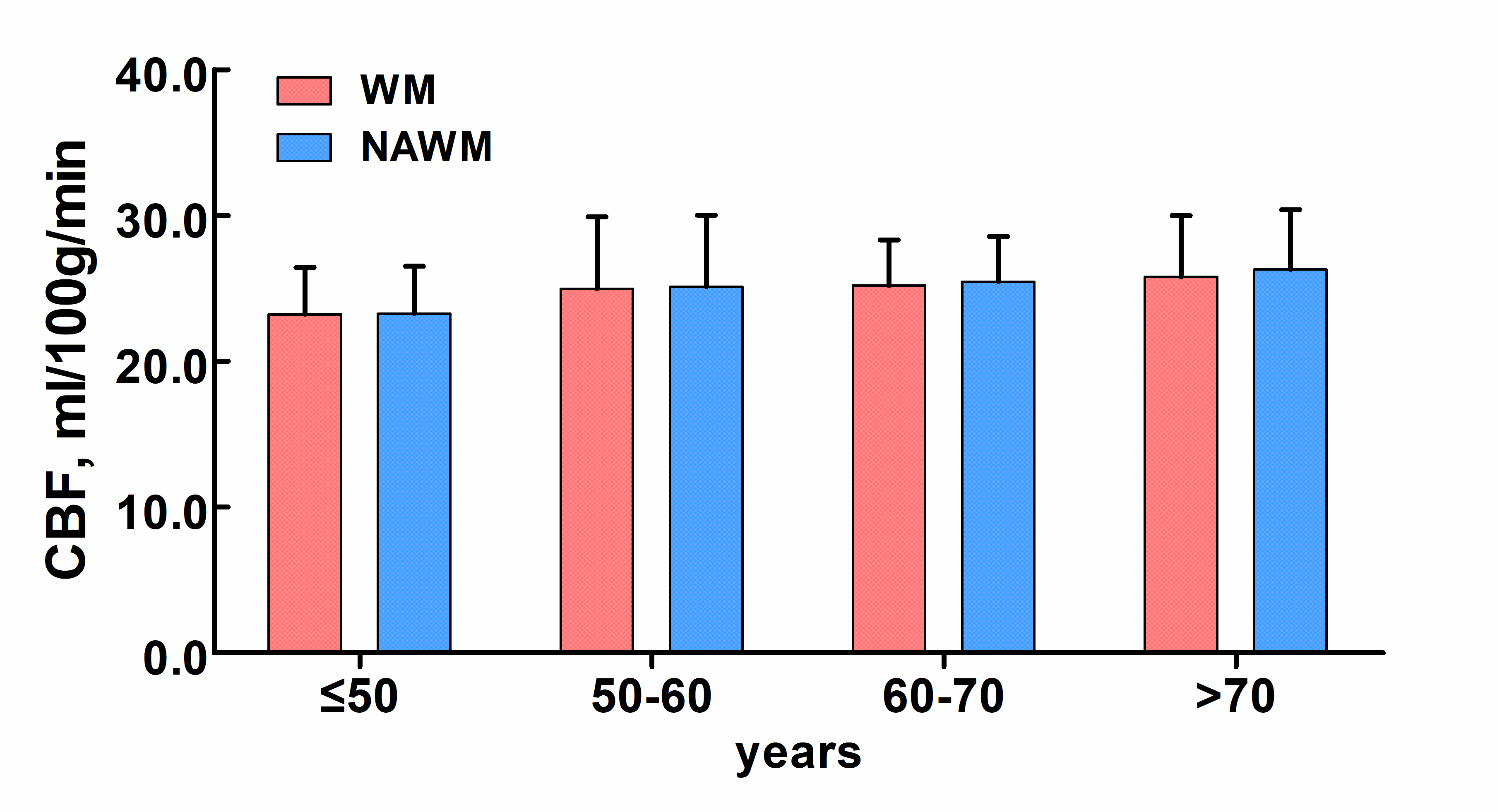
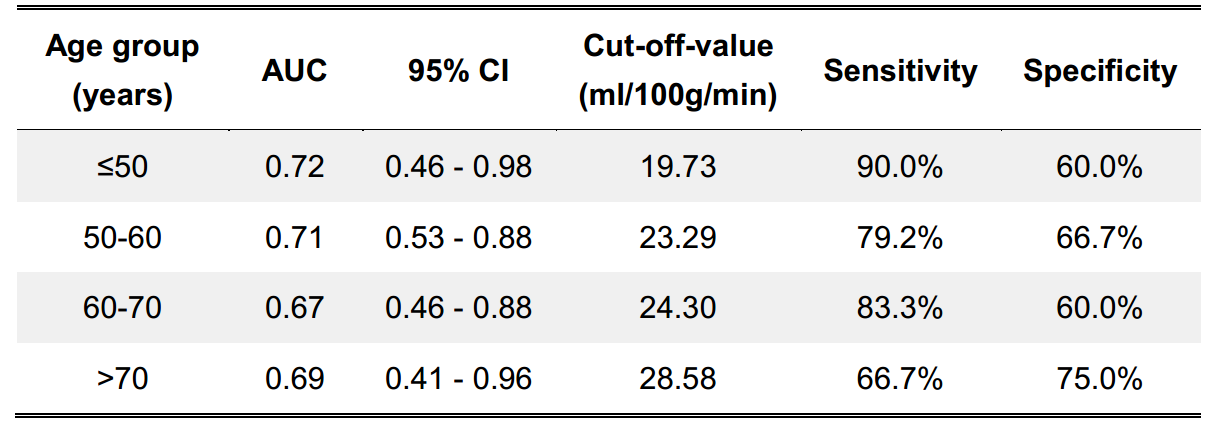
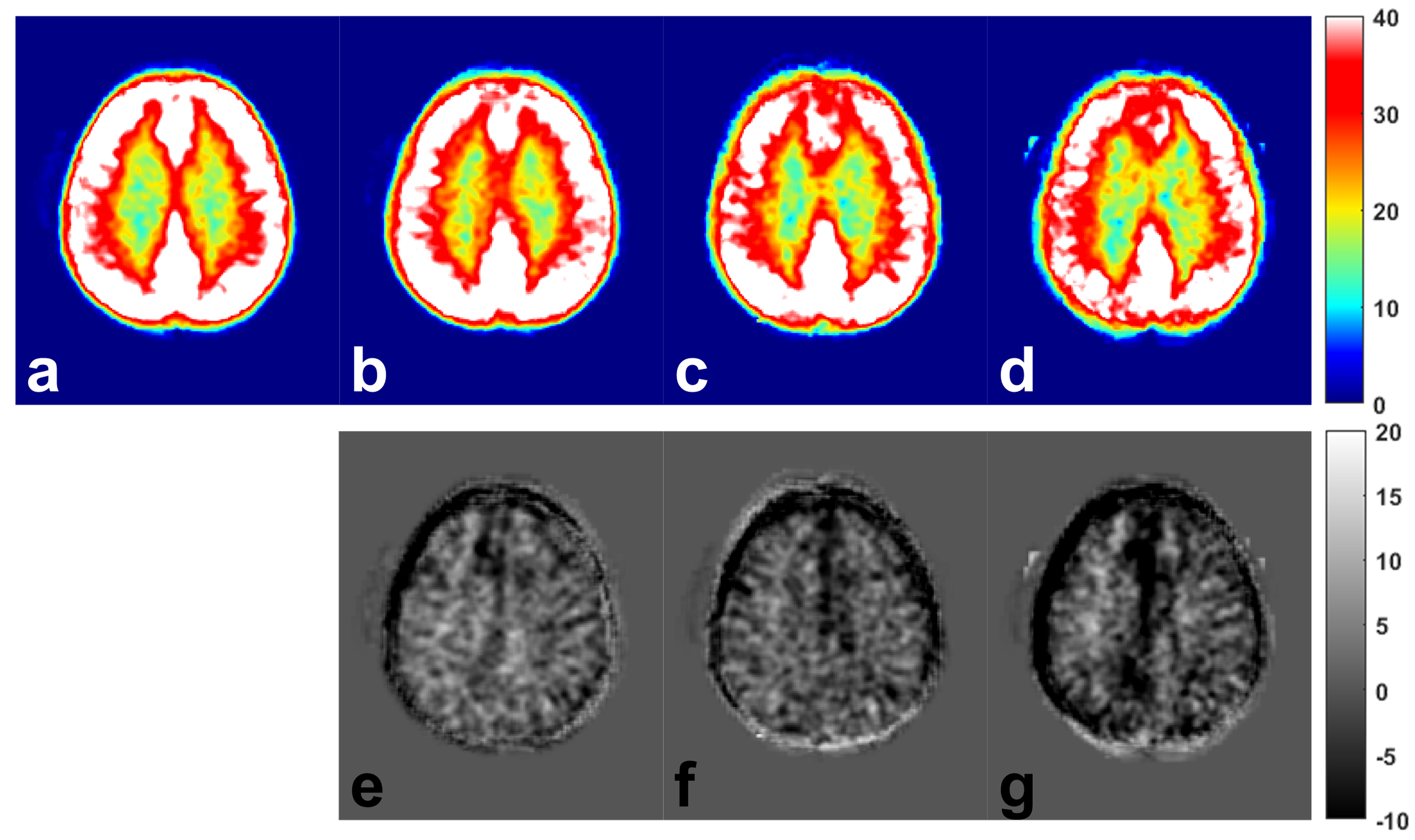
Spearman correlation analysis showed that the WML score was correlated with age (r=0.579, P<0.001). The correlation coefficients between WM CBF and WML score were 0.015 (P=0.920), -0.407 (P=0.010), -0.361 (P=0.064) and -0.454 (P=0.051) for subjects in ≤50 years, 50-60 years, 60-70 years, and >70 years’ groups, respectively. There was significant difference in CBF between NAWM and WMLs (24.7±4.0 ml/100g/min vs. 18.5±3.6 ml/100g/min, P<0.001). Significant increasing trends were found in age with CBF of WM (P=0.049), NAWM (P=0.018) and WMLs (P=0.029) (Fig. 2). The optimal cut-off values and the corresponding AUCs of WM CBF in discriminating moderate to severe WMLs (score ≥2) among different age groups were presented in Fig. 3 and Table 1. Fig.4 showed the normalized CBF maps by averaging the CBF of subjects in 4 age groups (a: ≤50 years, b: 50-60 years, c: 60-70 years, d: >70 years). The bottom row represents the deviations of CBF (CBF of subjects in 50-60 years (e), 60-70 years (f), >70 years (g) minus CBF of subjects in ≤50 years).Discussion and Conclusions
In this study population, we found that there was association between WM CBF and WML score, suggesting that the reduction of WM CBF might be an effective indicator for severity of WMLs. Interestingly, we found that the WM CBF increased with age. Our finding is consistent with the previous report of greater WM cerebrovascular reactivity (CVR) response in elderly individuals. This phenomenon may be due to the loss of demyelination and axon which frequently happens in the elderly, then WM becomes less densely packed so as to less hindrance for blood to penetrate in WM microvasculature. We also found that when WM CBF decreased below a certain threshold, it would result in WMLs. The ascending cut-off values with age revealed that the risk of developing WMLs increases with age in asymptomatic adults, even though the cerebral perfusion drops very little.Acknowledgements
This study is funded by the grants of Beijing Municipal Commission of Health and Family Planning (2016-1-2041), National Natural Science Foundation of China (81771825), Beijing Municipal Science and Technology Commission (D17110003017002, D17110003017003), Ministry of Science and Technology of China (2017YFC1307904, 2017YFC1307702, 2016YFC0901001) and Philips Healthcare.References
1. de Groot J, de Leeuw F, Oudkerk M, et al. Cerebral white matter lesions and cognitive function: the Rotterdam Scan Study. Ann Neurol. 2000;47(2):145-151.
2. van der Veen P, Muller M, Vincken K, et al. Longitudinal relationship between cerebral small-vessel disease and cerebral blood flow: the second manifestations of arterial disease-magnetic resonance study. Stroke. 2015;46(5):1233-1238.
3. Alsop D, Detre J, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73(1):102-116.
4. Liao D, Cooper L, Cai J, et al. Presence and severity of cerebral white matter lesions and hypertension, its treatment, and its control. The ARIC Study. Atherosclerosis Risk in Communities Study. Stroke. 1996;27(12):2262-2270.
5. Thomas B, Liu P, Park D, et al. Cerebrovascular reactivity in the brain white matter: magnitude, temporal characteristics, and age effects. J Cereb Blood Flow Metab. 2014;34(2):242-247.
Figures