2727
Intrinsic vulnerability of low blood flow watershed to white matter hyperintensities in cerebral small vessel disease1Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, MO, United States, 2Department of Neurology, Washington University School of Medicine, St. Louis, MO, United States
Synopsis
White matter hyperintensities (WMH), a major neuroradiological feature of cerebral small vessel disease (CSVD), have a characteristic spatial distribution in the deep white matter and periventricular regions. In this study, we demonstrated a striking spatial overlap between WMH lesion hot spots and the watershed region, defined by a nadir in CBF within the white matter, suggesting that watershed is a region with intrinsic vulnerability to CSVD-related injury.
Introduction
White matter hyperintensities (WMH) are known as a major structural endpoint of cerebral small vessel disease (CSVD). WMH have a characteristic spatial distribution--located in the deep white matter and periventricular regions--which reflects regional vulnerability.1,2 In this study, we hypothesized that the region with high WMH probability coincides with the watershed, characterized by a nadir in cerebral blood flow (CBF). The watershed or border zone regions are at the junction between two main arterial territories, which are at the distal regions of the major arterial supply. These regions are thought to have low CBF and are most vulnerable to hemodynamic impairments. To test this hypothesis, we first defined watershed region as low flow regions using resting CBF from a young healthy adult cohort. We then examined whether there is a spatial overlap between the watershed and high WMH burden regions obtained from another cohort with CSVD.Methods
A prospective MRI study enrolled two cohorts: (1) healthy young adults (N = 38, 25 females, age: 49.5 [31, 54] (Median [IQR])) and (2) older adults with CSVD risk factors and WMH (N = 55, 28 females, age: 69 [61, 77] (Median [IQR])). T1 MPRAGE and FLAIR images were acquired. CBF maps were obtained using 2-D pseudo-continuous arterial spin labelling (pCASL).3 WMH lesions were manually segmented by a board-certified vascular neurologist on FLAIR images using the Medical Image Processing, Analysis, and Visualization (MIPAV) software to create FLAIR lesion masks. T1, FLAIR, FLAIR lesion masks and CBF maps were then aligned to the symmetric International Consortium of Brain Mapping (ICBM) brain atlas through a series of linear and nonlinear image registration. An average CBF map was created from the healthy adult cohort. Within the white matter mask, regions with CBF ranging from 0-100 percentiles were separated into 20 tiers with an increment of 5th percentile. Moreover, a FLAIR WMH lesion density map was created from the CSVD cohort. Mean WMH lesion density and mean CBF in each region were calculated after mapping the CBF percentile tiers onto WMH density map and average CBF map, respectively.Results
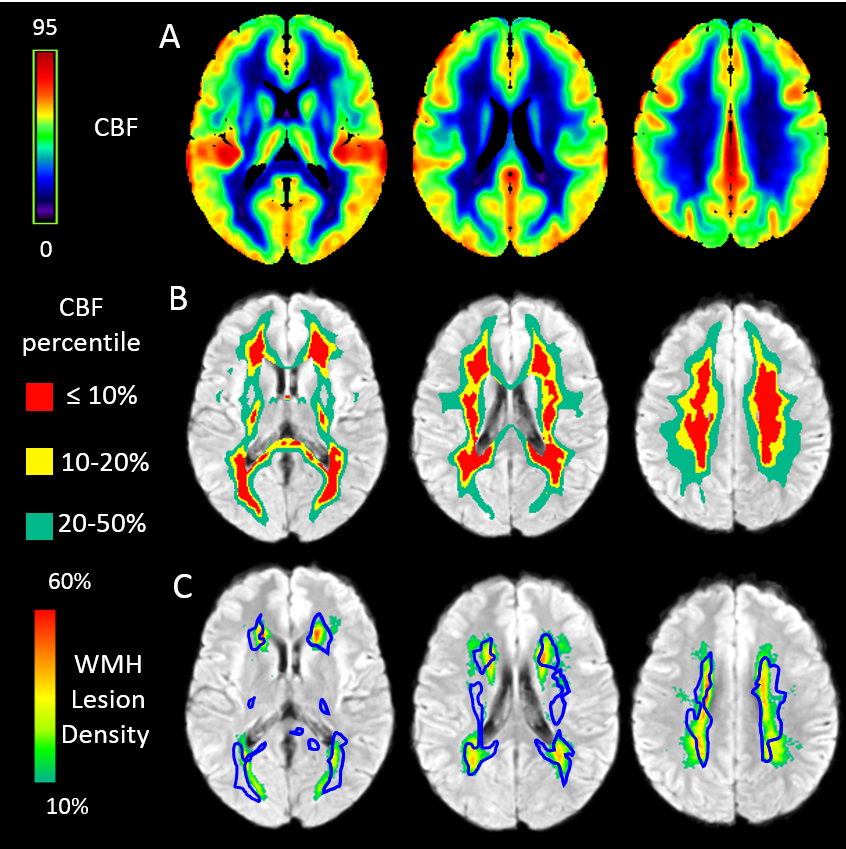
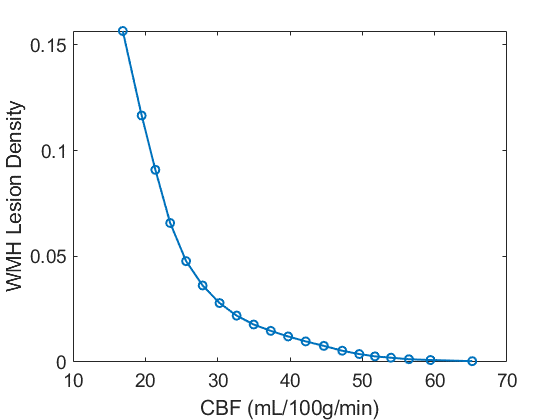
Figure 1A shows the average CBF map of the young healthy cohort. There is a high level spatial heterogeneities in CBF in healthy brains. Figure 1B illustrates the spatial distribution of regions with different white matter CBF percentiles. The 10th percentile CBF is outlined and overlaid onto the WMH lesion density map (Figure 1C). The WMH lesion density map reveals high WMH burden near the periventricular and deep white matter regions as expected. A striking spatial overlap between watershed ROI and WMH lesion hot spots was observed. Figure 2 shows the relationship between mean WMH lesion density and mean CBF in each white matter CBF tier. The mean WMH lesion density increases monotonically with a decrease in CBF. Moreover, the WMH burden rises drastically in regions with low CBF.Discussion
The Leukoaraiosis and Disability Study (LADIS) study demonstrated that WMH exhibit a characteristic spatial distribution within the subjects in periventricular and deep white matter from 605 patients.1,2 We have observed a similar spatial distribution of regions with high WMH burden in 55 CSVD patients. Moreover, we are the first to demonstrate that CBF nadir regions from young healthy subjects overlap with these high WMH burden regions in CSVD, suggesting an intrinsic regional vulnerability. The watershed is defined in the region within the 10th percentile CBF from a healthy young cohort, as it closely resembles WMH lesion hotspots.Conclusion
The low blood flow watershed defined under normal physiology represents regions with an intrinsic vulnerability to CSVD impairments. Watershed ROI defined in regions within the lowest 10th percentile in CBF can be used to investigate biomarkers associated with CSVD onset and progression in the future.Acknowledgements
This study was supported by grant from the National Institute of Health NIH 1R01NS082561, R01HL129241References
1. Rostrup, Egill, et al. "The spatial distribution of age-related white matter changes as a function of vascular risk factors—results from the LADIS study." Neuroimage 60.3 (2012): 1597-1607.
2. Pantoni, Leonardo, et al. "Impact of cerebral white matter changes on functionality in older adults: an overview of the LADIS study results and future directions." Geriatrics & gerontology international 15 (2015): 10-16.
3. Floyd, Thomas F., et al. "Precision of the CASL‐perfusion MRI technique for the measurement of cerebral blood flow in whole brain and vascular territories." Journal of Magnetic Resonance Imaging 18.6 (2003): 649-655.
Figures