2702
Robust, Atlas-Free, Automatic Segmentation of Brain MRI in Health and Disease1NINDS, National Institutes of Health, Bethesda, MD, United States, 2NIMH, National Institutes of Health, Bethesda, MD, United States, 3Inati Analytics, Potomac, MD, United States
Synopsis
An atlas-free, brain-segmentation algorithm that uses derivative-based features and logistic regression classifier was optimized and tested on images of healthy volunteers and individuals clinically diagnosed with a variety of neuroimmunological diseases.The algorithm was trained to classify gray and white matter, CSF, globus pallidus, white matter lesions, and “other” tissue classes from all the images routinely acquired at our center. The algorithm achieved highly accurate brain segmentations and outperformed widely used techniques for brain segmentation and lesion detection. The algorithm has been found to be versatile in brain segmentation using images acquired at other collaborator sites.
INTRODUCTION
Brain- and lesion-volumes derived from MRI serve as important imaging markers of disease progression in neurodegenerative diseases and aging. While manual segmentation of these volumes is both tedious and impractical in large cohorts of subjects, automated segmentation methods often fail in accurate segmentation of brains with severe atrophy or high lesion loads. Errors in atlas-based methods are compounded not only by the fact that size and distribution of lesions in the brain vary from one individual to next, but also because the likelihood of a lesion being present in any region varies between neurological diseases. Furthermore, multiple contrasts are routinely acquired in clinical MRI sessions and are heavily relied upon by radiologists in their clinical assessment, but not all these are used in brain segmentation. The purpose of this study was to develop an atlas-free brain Classification using DErivative-based Features (C-DEF), which utilizes all scans acquired at our center during the course of a routine MRI study at any center.METHODS
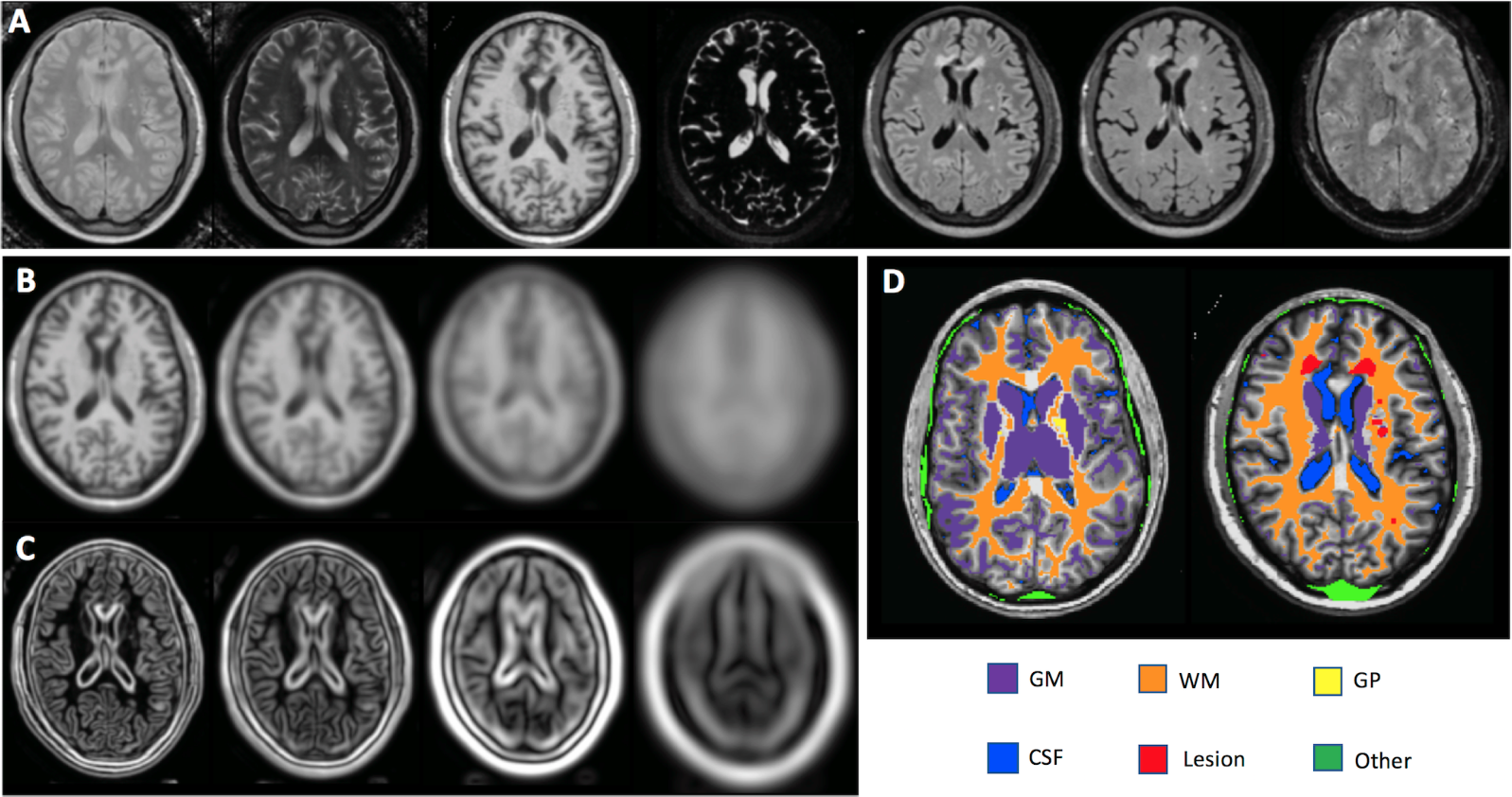
Proton-density, T2-weighted, T1-weighted, brain-free water, 3D FLAIR, 3D T2-weighted, and 3D T2*-weighted images, collected routinely on patients with neuroinflammatory diseases at the NIH, and their derived feature were used to optimize the C-DEF algorithm on healthy volunteers and HIV+ subjects on antiretroviral therapy (cohort 1, Figure 1). Images were coregistered using AFNI tools,1 bias-field corrected using a local statistic function,2 and normalized to the intensity at the 90th percentile to generate scaled images. Features were then derived using a Gaussian and Gaussian Gradient filter of four different kernel sizes of 1, 2, 4 and 8 voxels. Manually marked lesions and eroded FreeSurfer brain segmentation3,4 masks (compiled into gray and white matter, globus pallidus, CSF labels) were used in training. The optimized C-DEF was applied on a separate cohort HIV+ subjects on antiretroviral therapy (cohort two), and the results were compared with that of FreeSurfer and Lesion-TOADS.5,6 Finally, C-DEF segmentation was evaluated on subjects clinically diagnosed with various other neurological diseases, including multiple sclerosis, haploinsufficiency of the cytotoxic T-lymphocyte-associated protein 4 gene (CTLA4), and HTLV-I-associated myelopathy/tropical spastic paraparesis (HAM/TSP) (cohort three).RESULT
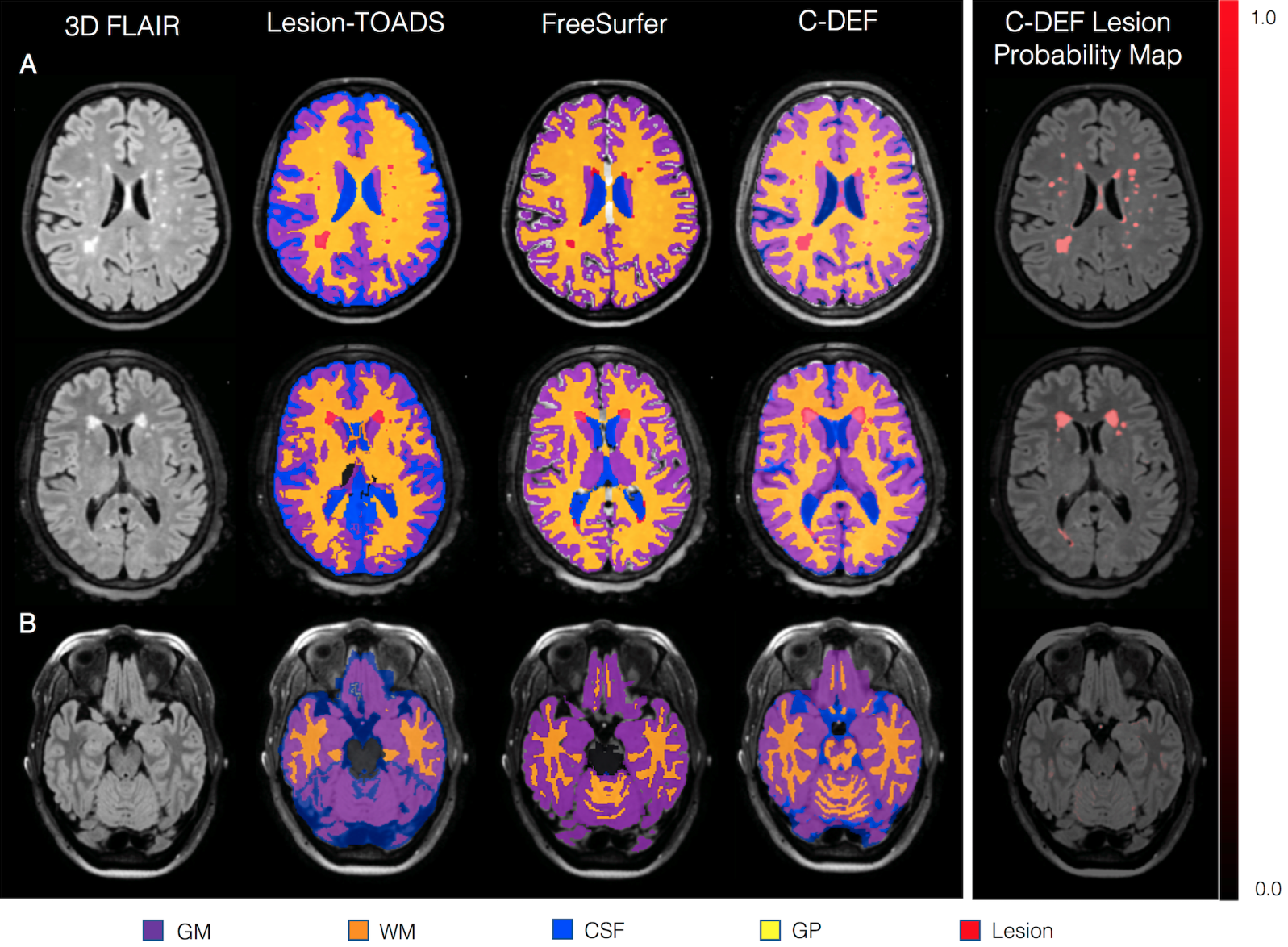
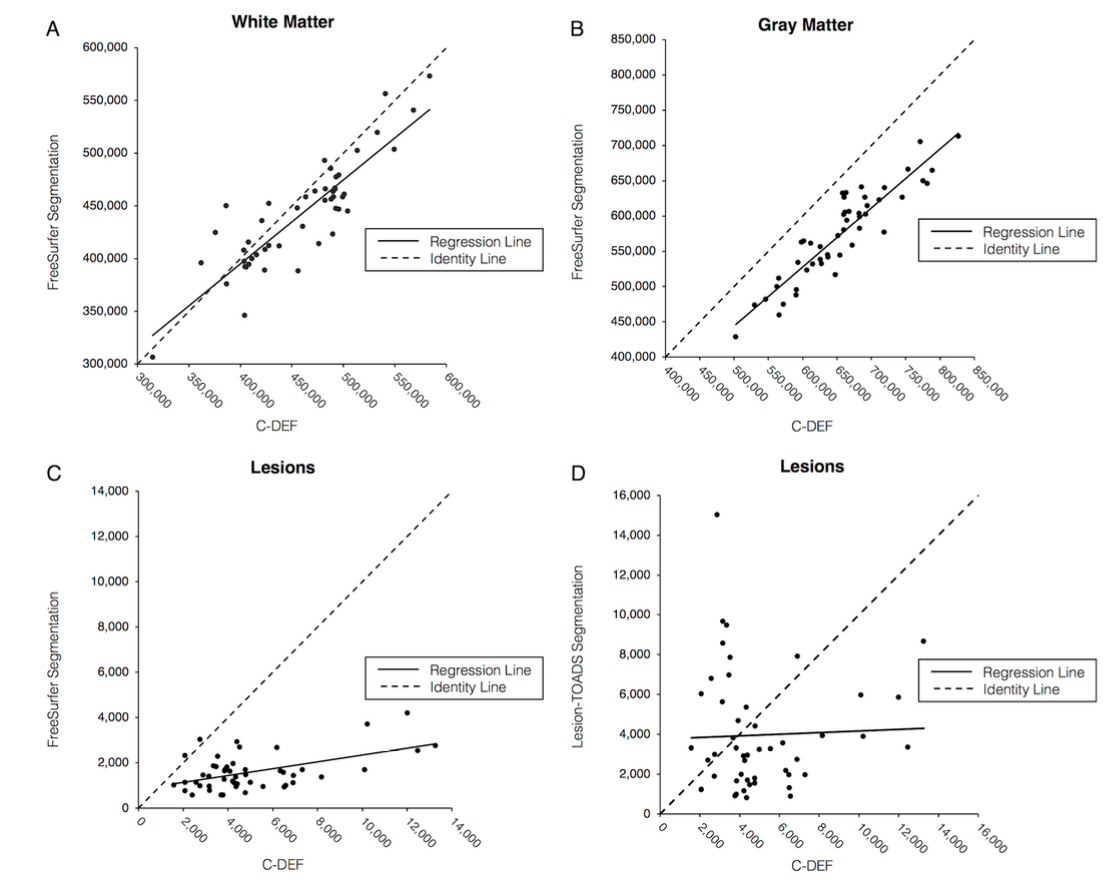
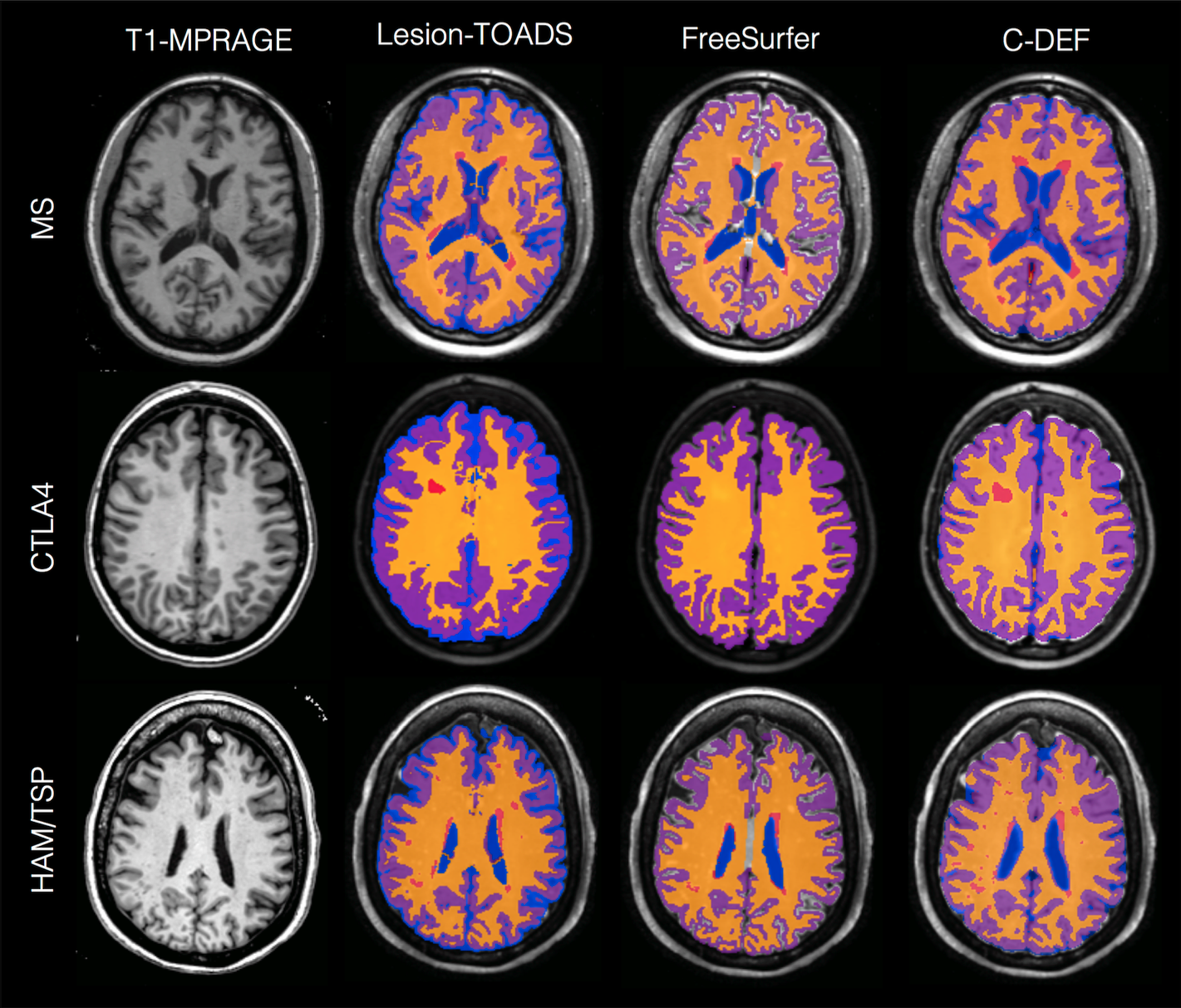
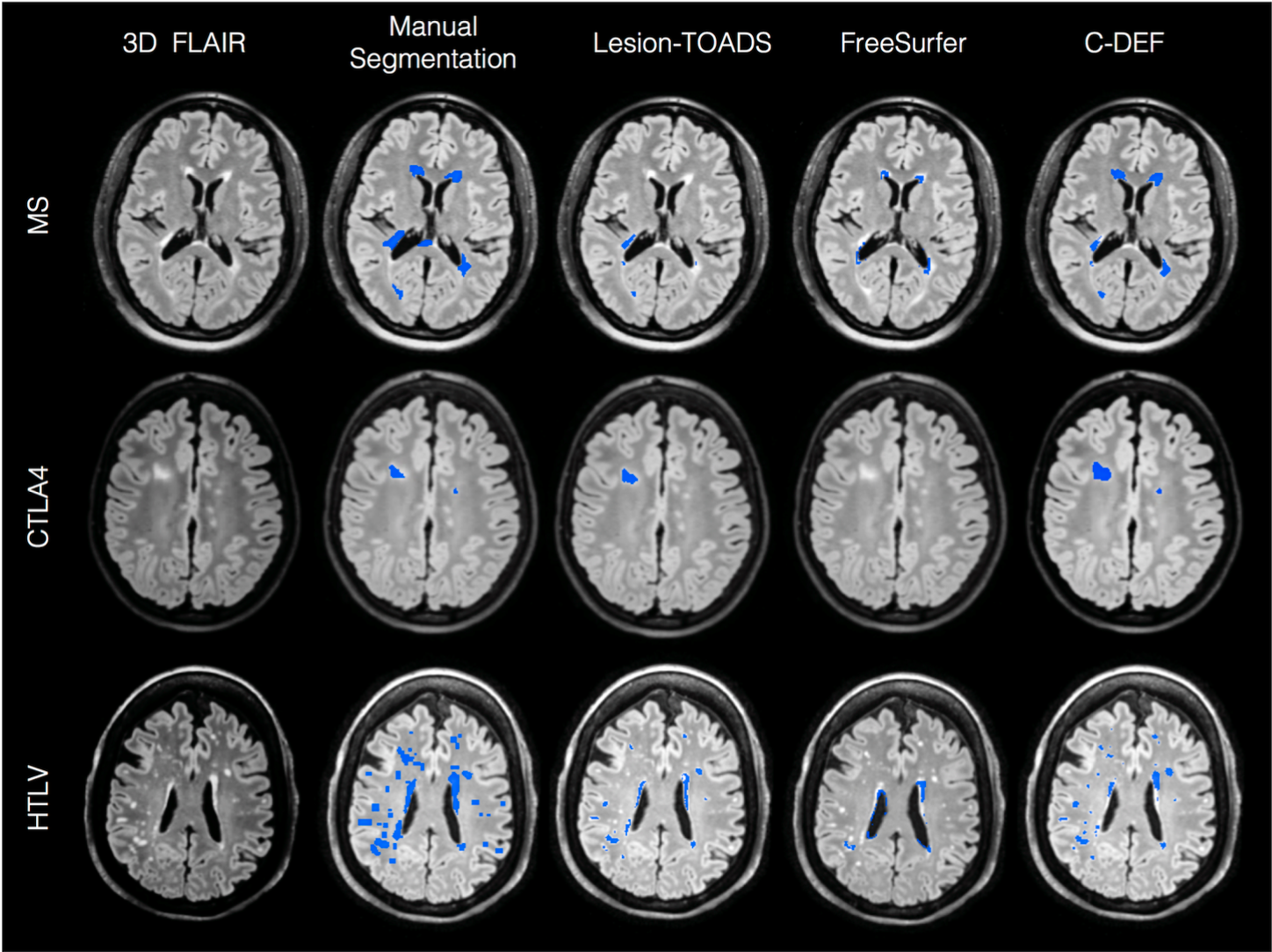
C-DEF was optimized on five healthy subjects (age 36 ±11 years), and five subjects infected with HIV (age 57 ±2.6 years) in cohort one. The optimized C-DEF outperformed FreeSurfer and Lesion-TOADS segmentation in 49 other subjects infected with HIV (cohort two, age 54 ±6 years) in qualitative (Figure 2) and quantitative (Figure 3) comparisons. Although trained only on HIV brains, sensitivity to detect lesions using C-DEF increased by 45% in HTLV-I-associated myelopathy/tropical spastic paraparesis (n=5; age 58 ±7 years), 33% in multiple sclerosis (n=5; 42 ±9 years old), and 4% in subjects with polymorphism of the cytotoxic T-lymphocyte-associated protein 4 gene (n=5; age 24 ±12 years) compared to Lesion-TOADS. Representative images, showing improvements in brain segmentation and lesion detection, are in Figures 4 and 5.DISCUSSION AND CONCLUSION
C-DEF outperformed other segmentation algorithms in the various neurological diseases explored herein, especially in lesion segmentation. This was attributed not only to its independence from spatial priors or disease-specific atlases, but also to the increased confidence of classification as it uses multiple imaging contrasts. Popular MRI brain segmentation algorithms utilize atlas-based and region-growing techniques. Algorithms such as FreeSurfer, SPM7and Lesion-TOADS rely on registration to a standard atlas to determine the likelihood that a voxel at particular location belongs to a particular tissue type. While this approach has been successful in healthy populations, errors tend to arise when the subject’s anatomy deviates significantly from the atlas, as is evident in subjects with neurological diseases.
The results reported herein use all routine images acquired at the NIH on patients with neuroinflammatory diseases. However, the algorithm can be easily trained and optimized for any set of contrasts and protocols for wider application. We are currently evaluating a larger cohort of patients with other neurological diseases. In addition, we have trained and are testing C-DEF on a completely different set of images acquired at a collaborator’s site (University of Edinburgh) to segment brains in patients with MS and small vessel disease. Further improvements to C-DEF using disease-specific training and improved feature sets are also being explored. Improving the accuracy of brain segmentation methodology will help better understand the relationship of imaging abnormalities to clinical and neuropsychological markers in disease.
Acknowledgements
Funded by the Intramural Research Program and the office of AIDS research at the NIH.References
1 Cox, R. W. AFNI: software for analysis and visualization of functional magnetic resonance neuroimages. Comput Biomed Res29, 162-173 (1996).
2 Vovk, A., Cox, R. W., Stare, J., Suput, D. & Saad, Z. S. Segmentation priors from local image properties: without using bias field correction, location-based templates, or registration. Neuroimage55, 142-152, doi:10.1016/j.neuroimage.2010.11.082 (2011).
3 Fischl, B. FreeSurfer. Neuroimage62, 774-781, doi:10.1016/j.neuroimage.2012.01.021 (2012).
4 Fischl, B.et al.Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron33, 341-355 (2002).
5 Shiee, N.et al.A topology-preserving approach to the segmentation of brain images with multiple sclerosis lesions. Neuroimage49, 1524-1535, doi:10.1016/j.neuroimage.2009.09.005 (2010).
6 Shiee, N., Bazin, P. L., Cuzzocreo, J. L., Blitz, A. & Pham, D. L. Segmentation of brain images using adaptive atlases with application to ventriculomegaly. Inf Process Med Imaging22, 1-12 (2011).
7 Ashburner, J. & Friston, K. Multimodal image coregistration and partitioning--a unified framework. Neuroimage6, 209-217, doi:10.1006/nimg.1997.0290 (1997).
Figures