2678
Anomalous functional connectivity in subregional amygdala networks in major depressive disorder1Huaxi Magnetic Resonance Research Center (HMRRC), Chengdu, China
Synopsis
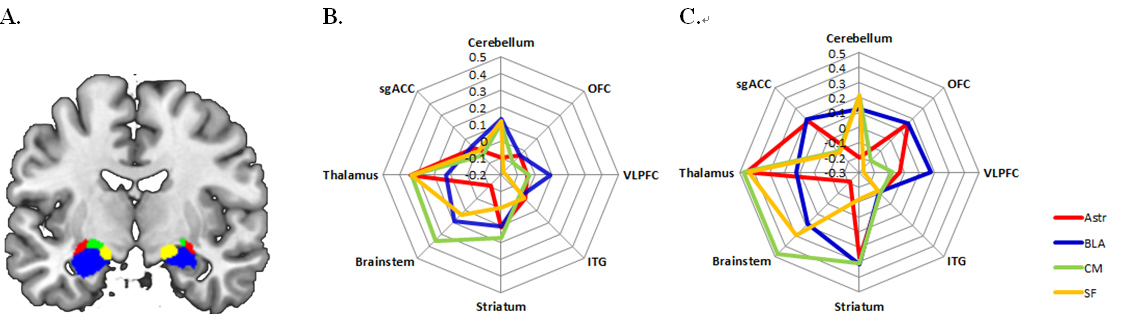
The LB, CM, SF and Astr are four main subregions of the amygdala. In this study, we use seed-based functional connectivity method to determine amygdala network dysfunction in MDD. Compared with HC, patients with major depressive disorder showed hypoconncetivity in AStr/LB- OFC circuits, in CM /SF-brainstem/cerebellum circuits and in AStr/CM/SF-thalamus/striatum circuits. These dysfunction in amygdala networks may modulate different emotional and cognitive function in derpession.
Purpose
The amygdala is a core structure of the brain’s emotion circuitry and amygdala-based network dysfunction has been found to be centrally implicated in major depressive disorder (MDD). It has four main subregions, including basolateral (LB) centromedial (CM), superficial (SF) nucleus and the amygdalostriatal transition area (Astr), and each modulates distinct affective and cognitive functions via their unique connectivity patterns with cortical and subcortical regions1. Nevertheless, how those subtle networks dysfunction were involved in MDD has never been explored. So, in the current study, we aim to examine alteration of subregional amygdala networks in adult medication-free patients with MDD to determine how those different sub-networks could contribute to the neuropathology of depression. In addition, we will also examine the amygdala structure to determine if the functional aberrancies are accompanied with anatomical change.Materials & Methods
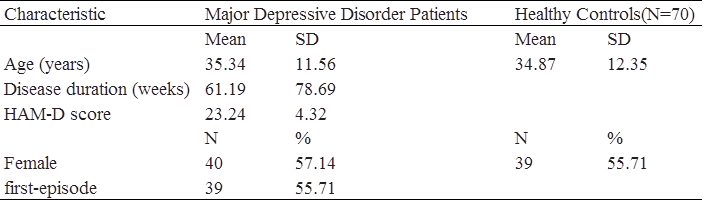
A total of 140 subjects (70 MDD patients and 70 healthy individuals(HC)) were recruited in this study. Among the patients, 39 individuals have never received any medication treatment, and 31 participants were medication-free for a minimum of 14 days prior to the scan. Imaging was conducted on GE Signa EXCITE 3-T MR system (GE Healthcare, Milwaukee) with an 8-channel phased array head coil. First, the masks of amygdala and its four subregions AStr, LB, CM and SF were acquired with cytoarchitectonically-defined probabilistic maps2, which were defined as regions-of-interests (ROIs). Then, voxel-wise functional connectivity analysis was conduct to assess amygdala networks. Preprocessing of the resting-state functional images includes excluding the first 10 time points, slice timing, realignment, spatial normalization, smooth, regressing out six nuisance signals and filtering. In order to frame amygdala networks, we use seed-based functional connectivity analysis with up-mentioned ROIs as seeds. We then extracted averaged time course of each seed region, and calculated Pearson correlation coefficients between the seed’s time course and the rest voxels of the brain. Fisher’s r-to-z transformation was further performed on the coefficients map to improve normality. Subsequently, voxel-based morphometry (VBM) with Diffeomorphic Anatomical Registration Through Exponentiated Lie Algebra (DARTEL) was performed on the T1-weighted images using SPM8 software; the steps are segment, create template, normalize to Montreal Neurological Institute (MNI) space and smooth. To characterize differences between MDD and HC, voxel-based functional connectivity maps and gray matter volumecomparison of these ROIs between the two groups was performed, with a random-effects two-sample t test. The significance threshold was set to p < 0.005 at the voxel level and to (p<0.05 FWE corrected) at the cluster level.Results
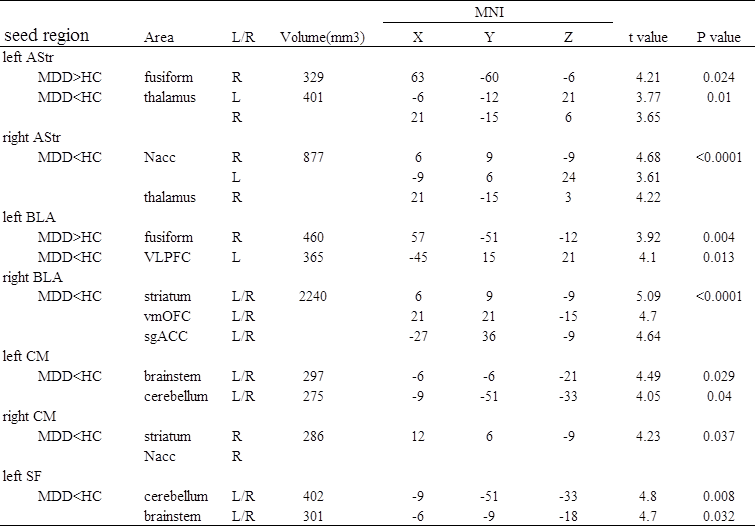
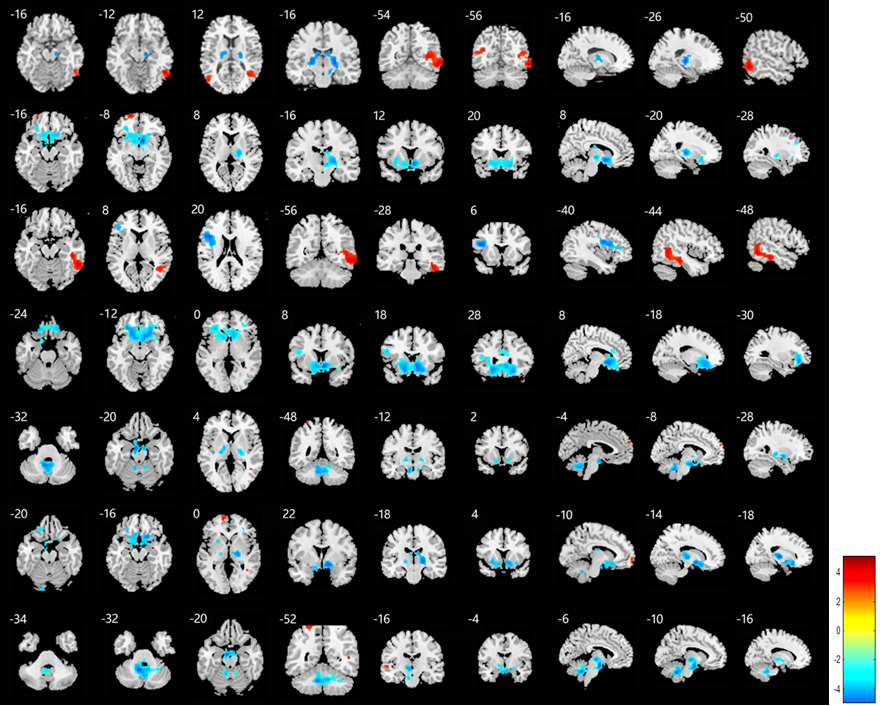
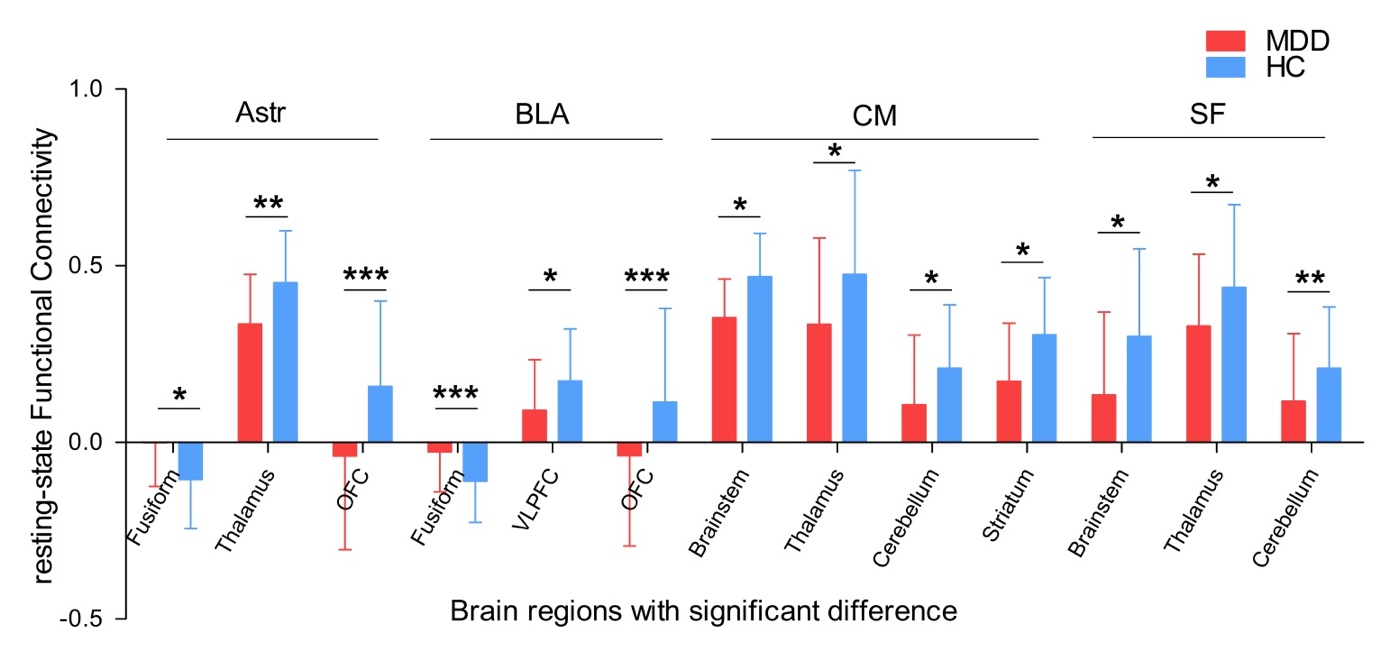
The demographics and clinical characteristics of the subjects are shown in Table 1. There are no difference in age and sex between MDD and HC. Compared with HC, patients with MDD showed decreased functional connectivity in AStr and LB with orbital frontal cortex (OFC), in CM and SF with brainstem/cerebellum and in AStr/CM/SF-thalamus/striatum networks. Increased connectivity was observed in the left AStr/LB with the fusiform gyrus. (Fig. 1-3 and Table 2) There is no difference in GMV of amygdala and amygdala subregions between the two groups.
Discussion & Conclusion
In the current study, we found amygdala subregional network dysfunction in MDD which is independent of structural changes. And more importantly, hypoconnectivity and hyperconnectivity in different subregional networks may reflect an imbalanced network functioning, which possibly modulates different emotional and cognitive dysfunction in MDD. Hyperconnectivity of Astr/LB-fusiform and hypoconnectivity of AStr/LB-PFC imply increased sensitivity to emotional stimulus but poor control of emotion stimulus; while hypoconnectivity of CM/SF-brainstem/cerebellum may underlie vegetative symptomatology and dysfunction of behavioral response to emotional stimulus. In addition, AStr/LB/CM-striatum/thalamus hypoconnectivity may interfere with reward and goal-related processes.3-6 These findings suggested that amygdala subregions play different roles in affective or cognitive dysfunctions, which may underlie the neural mechanism of MDD and potentially put new insights into clinical treatment.
Acknowledgements
This study was supported by a grant from the National Natural Science Foundation of China (81671669) and by a Sichuan Provincial Youth Grant (2017JQ0001).References
1. LeDoux, J.E., Emotion circuits in the brain. Annu Rev Neurosci, 2000. 23: p. 155-84.
2. Eickhoff, S.B., et al., A new SPM toolbox for combining probabilistic cytoarchitectonic maps and functional imaging data. Neuroimage, 2005. 25(4): p. 1325-35.
3. Etkin, A., T. Egner, and R. Kalisch, Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn Sci, 2011. 15(2): p. 85-93.
4. Price, J.L. and W.C. Drevets, Neurocircuitry of mood disorders. Neuropsychopharmacology, 2010. 35(1): p. 192-216.
5. Cullen, K.R., et al., Abnormal amygdala resting-state functional connectivity in adolescent depression. JAMA Psychiatry, 2014. 71(10): p. 1138-47.
6. Sacchetti, B., T. Sacco, and P. Strata, Reversible inactivation of amygdala and cerebellum but not perirhinal cortex impairs reactivated fear memories. Eur J Neurosci, 2007. 25(9): p. 2875-84.
Figures