2674
Cortical structure mediates the effect of childhood maltreatment on depression relapse during longitudinal follow-upHarald Kugel1, Nils Opel2, Ronny Redlich2, Katharina Dohm2, Dario Zaremba2, Janik Goltermann2, Jonathan Repple Repple2, Claas Kaehler2,3, Dominik Grotegerd2, Elisabeth J. J. Leehr2, Joscha Böhnlein2, Katharina Förster2, Susanne Meinert2, Verena Enneking2, Lisa Sindermann2, Fanny Dzvonyar2, Daniel Emden2, Ramona Leenings2, Nils Winter2, Tim Hahn2, Walter Heindel1, Ulrike Buhlmann4, Bernhard T. Baune5, Volker Arolt2, and Udo Dannlowski2
1Institute of Clinical Radiology, University of Münster, Münster, Germany, 2Department of Psychiatry, University of Münster, Münster, Germany, 3Department of Mathematics and Computer Science, University of Münster, Münster, Germany, 4Department of Clinical Psychology and Psychotherapy, University of Münster, Münster, Germany, 5Department of Psychiatry, University of Melbourne, Melbourne, Australia
Synopsis
Childhood maltreatment is a strong risk factor for the onset of major depressive disorder (MDD) and associated with unfavorable course of the disease. Both, maltreatment and MDD have been independently associated with structural alterations in partly overlapping brain regions suggesting that brain structural changes could mediate the adverse influence of maltreatment on clinical outcome in MDD. In this study the relationship between childhood trauma, brain structural alterations and adverse disease course was investigated in a longitudinal design. Our results suggest that cortical surface area reductions might mediate the prospective association between early life stress and future depression relapse.
Introduction
With a lifetime prevalence of 16%, major depressive disorder (MDD) is one of the most common and debilitating psychiatric disorders.1 Childhood maltreatment is among the strongest risk factors for the onset of MDD2 that has also been associated with unfavorable course of this disease.3,4 Moreover, both maltreatment and MDD have repeatedly been associated with structural alterations in partly overlapping brain regions suggesting that brain structural changes could mediate the adverse influence of maltreatment on clinical outcome in MDD.5-10 While these associations are well-known, there are no longitudinal studies to confirm this hypothesis. Our aim therefore was to investigate the mechanistic relationship between childhood trauma, brain structural alterations and adverse disease course as indicated by depression relapse in a longitudinal design.Methods
A total of n = 110 MDD patients participated in the present study. Baseline data acquisition comprised clinical assessments, structural MRI and retrospective assessment of the extent of childhood maltreatment experiences using the Childhood Trauma Questionnaire (CTQ).11 Clinical assessments were done in all participants at baseline and at follow-up 2 years after initial recruitment. Depending of experience of another depressive episode during the follow-up period, patients were assigned to a 'Relapse' (n = 75) and a 'No Relapse' (n = 35) group.12 In addition, medication load and previous disease course were assessed. MRI images were obtained at 3 T (Gyroscan Intera with Achieva upgrade) using a 3D T1w TFE-sequence (TR/TE/FA = 7.4 ms/3.4 ms/9°, inversion prepulse every 814.5 ms, reconstructed to voxels of .5 mm edge length). Images were preprocessed using the cortical parcellation stream of Freesurfer (Version 5.3) with default parameters.13 Volumes of the 14 available subcortical brain structures and surface and thickness measures of 68 cortical regions bilaterally were evaluated. Statistical analysis with SPSS version 25 was performed to evaluate the association of (1) Childhood maltreatment and MDD relapse (independent sample t-test), (2) brain structure at baseline and relapse at follow-up (ANCOVA, corrected for multiple comparisons), and (3) childhood maltreatment and brain structure (partial correlation). Possible mediation effects were analyzed using a bootstrapping approach as implemented in the SPSS macro PROCESS.14Results
(1) Patients with depression relapse at follow-up showed a higher Childhood Maltreatment level (CTQ score) (t(1,108) = -2.07, p = 0.041; Fig 1). (2) Cortical surface of the right insular cortex at baseline was reduced in patients with depression relapse at follow-up (F(1,105) = 13.755, p < 0.001, ηp2 = 0.116; Fig 2), while baseline subcortical volume and cortical thickness showed no associations with future relapse. (3) CTQ scores correlated with reduced right insular surface area (r = -0.198, p = 0.023; Fig. 3). The applied mediation model indicated that the effect of CTQ scores on future depression relapse was significantly mediated by right insular surface area (Fig. 4). Controlling for depression medication and disease course prior to recruitment did not alter the results.Discussion
The finding of a prospective association between childhood maltreatment and depression relapse is well in line with reports from the literature including meta-analytic evidence. It supports a hypothesis that exposure to maltreatment might represent a clinical distinct subtype of MDD characterized by poorer treatment response, recurrent forms of MDD and greater symptom severity.2,3,15 Moreover, the presented results highlight the clinical relevance of the previously introduced concept of “limbic scars”6 as an adverse consequence of maltreatment experiences in depression, a notion that is supported by a multitude of studies demonstrating associations between maltreatment and altered brain structure.5,6,8,16 Yet, the present study is the first to combine both concepts and thus sheds more light on potential mechanisms that might underlie this clinical distinct subtype of MDD.Conclusions
The present study provides a comprehensive empirically based concept linking maltreatment and brain structural alterations with unfavorable clinical outcomes in major depression. Our results suggest that cortical surface area reductions mediate the prospective association between early life stress and future depression relapse, i.e. the detrimental impact of early life stress on brain structural alterations increases the risk of adverse disease courses in major depression.Acknowledgements
Funded by German Research Foundation (DFG, grant FOR2107 DA1151/5-1 and DA1151/5-2; SFB-TRR58, Projects C09 and Z02) and Interdisciplinary Center for Clinical Research (IZKF) of the medical faculty of Münster (grant Dan3/012/17) and Deanery of the Medical Faculty of the University of Münster.References
1. Kessler RC, Berglund P, Demler O, et al. The Epidemiology of Major Depressive Disorder. JAMA. 2003;289(23):3095-3105. 2. Gilbert R, Widom CS, Browne K, et al. Burden and consequences of child maltreatment in high-income countries. Lancet 2009; 373(9657):68-81. 3. Teicher MH, Samson JA. Childhood Maltreatment and Psychopathology: A Case for Ecophenotypic Variants as Clinically and Neurobiologically Distinct Subtypes. Am J Psychiatry. 2013;170(10):1114-1133. 4. Nelson J, Klumparendt A, Doebler P, Ehring T. Childhood maltreatment and characteristics of adult depression: Meta-analysis. Br J Psychiatry 2017;210(2):96-104. 5. Opel N, Redlich R, Zwanzger P, et al. Hippocampal Atrophy in Major Depression: a Function of Childhood Maltreatment Rather than Diagnosis? Neuropsychopharmacology. 2014;39(12):2723-2731. 6. Dannlowski U, Stuhrmann A, Beutelmann V, et al. Limbic scars: long-term consequences of childhood maltreatment revealed by functional and structural magnetic resonance imaging. Biol Psychiatry. 2012;71(4):286-293. 7. Kelly PA, Viding E, Wallace GL, et al. Cortical Thickness, Surface Area, and Gyrification Abnormalities in Children Exposed to Maltreatment: Neural Markers of Vulnerability?Biol Psychiatry. 2013;74(11):845-852. 8. Teicher MH, Anderson CM, Polcari A. Childhood maltreatment is associated with reduced volume in the hippocampal subfields CA3, dentate gyrus, and subiculum. Proc Natl Acad Sci USA. 2012;109(9):E563-572. 9. Redlich R, Opel N, Bürger C, et al. The Limbic System in Youth Depression: Brain Structural and Functional Alterations in Adolescent In-Patients with Severe Depression. Neuropsychopharmacology. 2018;43(3):546-554. 10. Rao U, Chen L-A, Bidesi AS, et al. Hippocampal changes associated with early-life adversity and vulnerability to depression. Biol Psychiatry. 2010;67(4):357-364. 11. Bernstein DP, Fink L, Handelsman L, et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry.1994;151(8):1132-1136. 12. Zaremba D, Dohm K, Redlich R, et al. Association of Brain Cortical Changes With Relapse in Patients With Major Depressive Disorder. JAMA Psychiatry. 2018;75(5):484-492. 13. https://surfer.nmr.mgh.harvard.edu/ 14. Mackey S, Chaarani B, Kan K-J, et al. Brain Regions Related to Impulsivity Mediate the Effects of Early Adversity on Antisocial Behavior. Biol Psychiatry. 2017;82(4):275-282. 15. Nemeroff CB. Paradise Lost: The Neurobiological and Clinical Consequences of Child Abuse and Neglect. Neuron.2016;89(5):892-909. 16. Frodl T, Janowitz D, Schmaal L, et al.Childhood adversity impacts on brain subcortical structures relevant to depression. J Psychiatr Res. 2017;86:58-65Figures
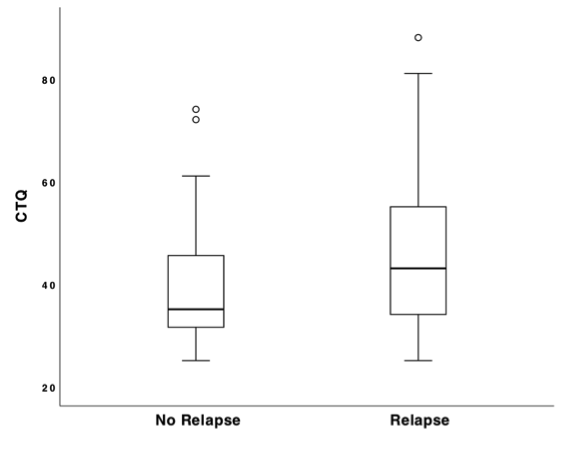
Figure 1. Association between MDD relapse at follow-up and childhood maltreatment. Boxplots show minimum, first quartile, median, third quartile, and maximum; CTQ, Childhood trauma questionnaire score.
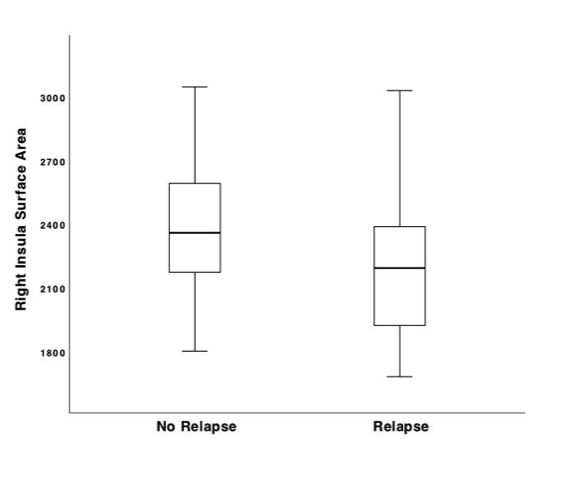
Figure 2. Association between right insula surface area at baseline (in mm2) and MDD relapse at follow-up.
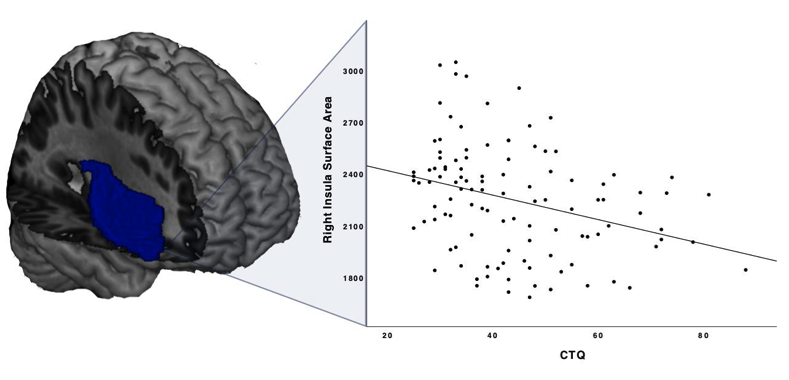
Figure 3. Association between right insula surface area at baseline (in mm2) and CTQ score.
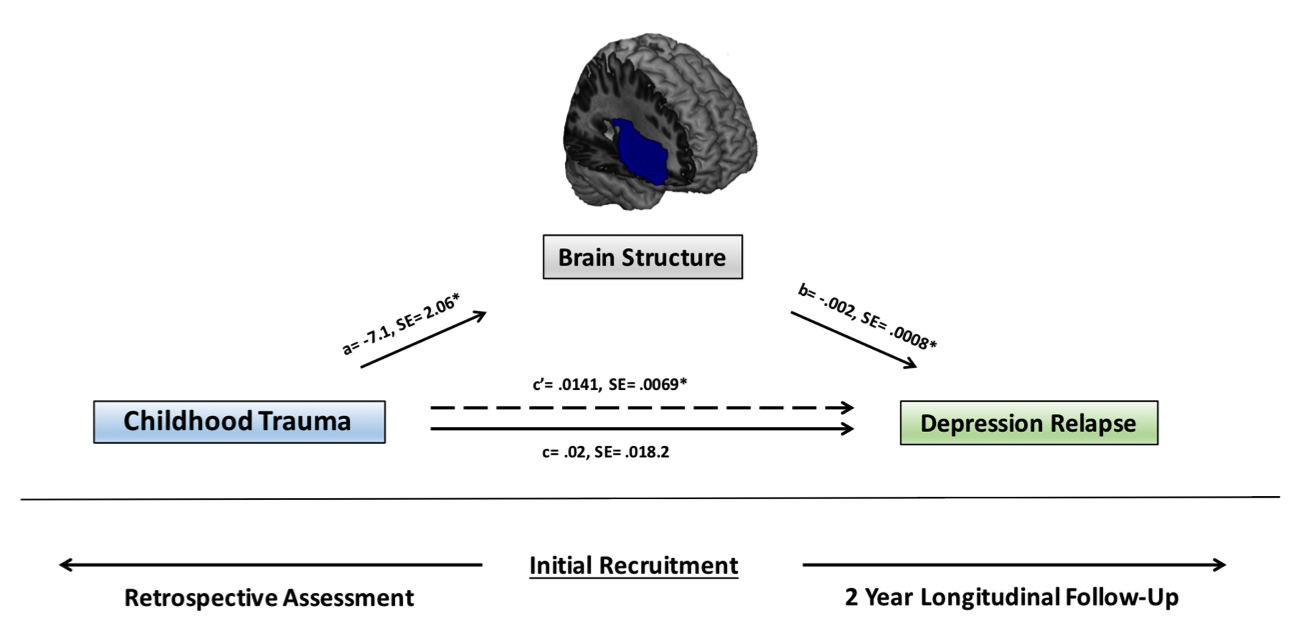
Figure 4. Applied mediation model and underlying study design for data acquisition. Unstandardized coefficients and standard errors for each path of the mediation model are presented. *indicates significance at p < 0.05