2672
Validation of zTE MRA in the characterization of cerebrovascular diseases: a feasibility study1Department of Radiology, Northern Jiangsu People’s Hospital, Yangzhou, China, 2MR Research China, GE Healthcare, Beijing, China
Synopsis
In this study, we aimed to investigate the feasibility of zero echo time magnetic resonance angiography (zTE-MRA) in the characterization of cerebrovascular diseases. Comparing with the time of flight (TOF) MRA, zTE-MRA showed more robust performance in depicting cerebrovascular diseases with dramatically reduced acoustic noise, higher signal homogeneity, less venous signal/artifact and higher inter-modality agreement and correlation with computed tomography angiography (CTA). We therefore demonstrated that zTE MRA could be a promising technique and further applied routinely in the clinic for patients with cerebrovascular diseases.
Introduction
Cerebrovascular disease is the main factor of ischemia or hemorrhagic accident within brain tissues. Compared to computed tomography angiography (CTA) with risks of radiation, magnetic resonance angiography (MRA) was proposed as a promising alternative for vascular assessment1.
Nowadays, newly developed MRA techniques have dramatically expanded their clinical applications. Particularly, a so-called zero-echo-time (zTE) radial arterial-spin-labeling (ASL) -MRA technique, integrating a continuous ASL strategy and a zTE radial acquisition read-out has demonstrated its potential in follow-up assessment of coiled aneurysm2,3.
However, for other cerebrovascular disorders the feasibility of this technique remains unclear. Therefore, this study aimed to investigate the feasibility of this novel MRA approach in a clinical population. Time-of-flight (TOF)-MRA was also measured for comparison and CTA measurement served as a reference.
Materials and Methods
69 patients (38 males&31 females; 60.13±14.06 years), suspected with cerebrovascular disorders, were recruited. Written consent forms were obtained from them.
All patients received both CTA and MRA (zTE- and TOF-MRA) measurements on GE light speed CT99 and Discovery 750w, respectively.
zTE-MRA was performed with the following parameters: FOV/Matrix=180×180mm/180×180; bandwidth=31.25kHz; flip angle=3o. For TOF-MRA, the scan parameters were FOV/Matrix, 220×220mm/320×320; bandwidth=41.67kHz; flip angle=15o.
The data were analyzed in three steps:
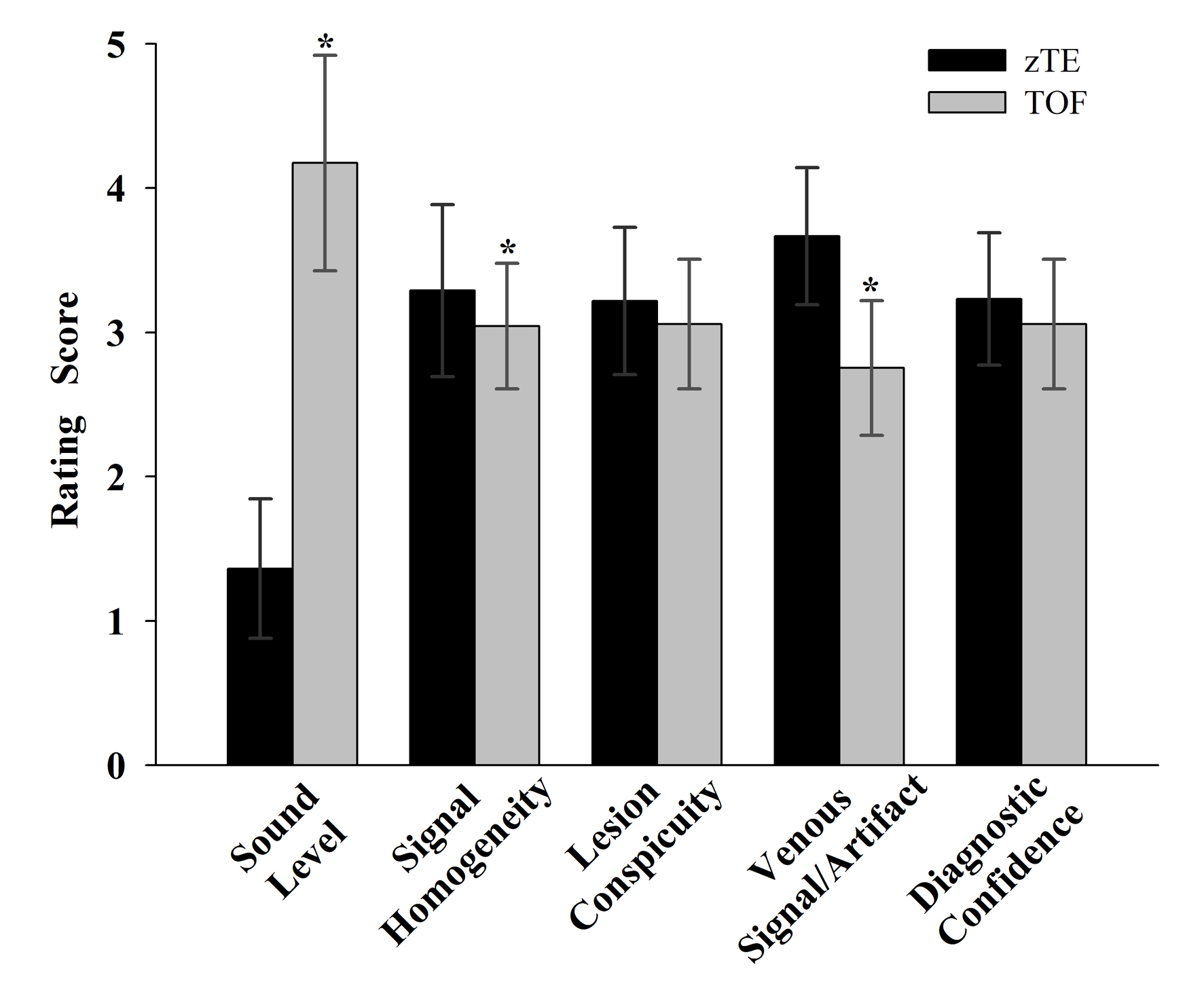
1. Sound levels of zTE and TOF MRA measurement were respectively estimated subjectively with a 5-point scale (0=no, 1=mild, 2=moderate, 3=loud, 4=very loud, 5=unacceptable noise) and objectively using a sound level meter in different modes (Ambient, zTE-MRA scanning, TOF-MRA scanning).
2. For zTE and TOF MRA images, the signal homogeneity, lesion conspicuity, venous signal/artifact and diagnostic confidence were respectively scored using a 4-point scale (4=excellent, 3=good, 2=poor, 1=not visible) independently by two neuro-radiologists.
3. The degree of stenosis was graded using the North American Society of Carotid Surgery standard (1 for <30%, 2 for 30%-69%, 3 for 70%-99%, 4 for 100%). The aneurysms were divided into Group small (≤3mm) and Group large (>3mm) based on the diameters measured.
All statistical analyses were performed using SPSS 19.0 software. The noise level and image quality ratings were evaluated using Wilcoxon-signed-rank tests, respectively. ANOVA test was used to analyze the objective sound level. Spearman’s correlation coefficient was used to evaluate the correlation of both MRAs with CTA for stenosis analysis. Weighted-kappa (κ) statistics were used to assess inter-modality agreement between both MRAs and CTA. The aneurysm diameters measured on MRA and CTA images were respectively correlated with a Pearson analysis. P<0.05 was considered statistically significant.
Results
In total 69 patients, 43 steno-occlusive cases were found in 31 patients and 38 cerebral aneurysm cases in 26 patients. In addition, there were 2 arteriovenous-malformation (AVM) patients, 3 Moyamoya patients, and 7 patients without evident vascular diseases.
The rating scale based on subjective estimation showed significantly lower sound level perception with zTE-MRA compared with TOF-MRA (Fig.1). Noise levels measured objectively were significantly reduced by 37.53% (34.85dB) in zTE-MRA than in TOF-MRA.
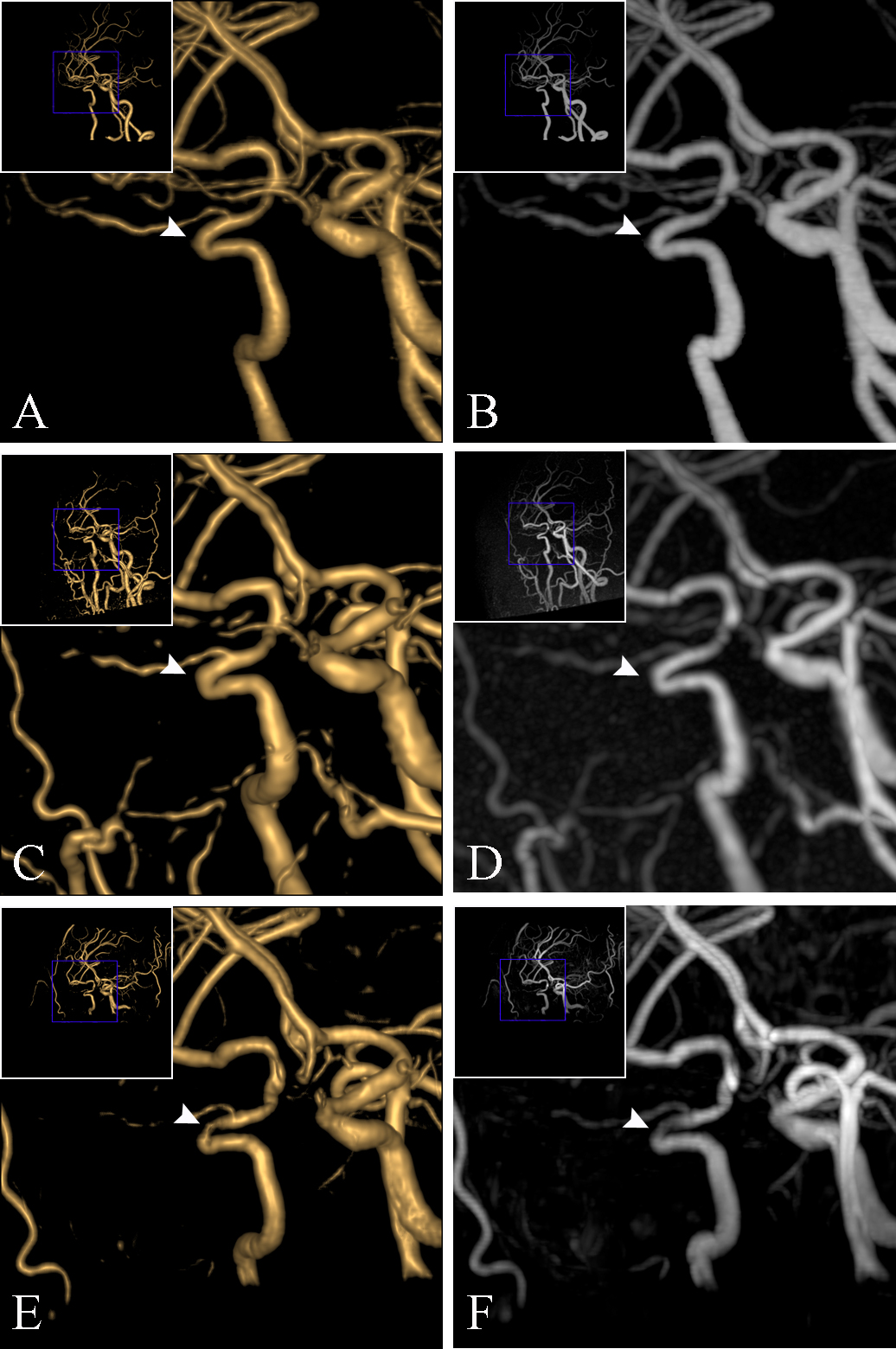
Compared with TOF-MRA images, zTE-MRA images showed significantly higher signal homogeneity (3.29±0.59 vs. 3.04±0.43; P=0.03), and larger venous signal/artifact (3.67±0.47 vs. 2.75±0.46; P=0.01; Figs.1-5). For lesion conspicuity and diagnostic confidence, comparable performance was found between zTE- and TOF-MRA images (lesion conspicuity: 3.21±0.51 vs. 3.06±0.45; P=0.08; diagnostic confidence: 3.23±0.46 vs. 3.05±0.44; P = 0.06; Fig.1).
The correlation of MRA sequences with CTA results were both high (zTE, r: 0.94; TOF, r: 0.92). The inter-modality agreement between zTE-MRA and CTA (weighted κ: 0.90; confidence interval (CI): 0.82–0.99) was higher than that between TOF-MRA and CTA (weighted κ: 0.81; CI: 0.71–0.92). Disagreements between MRAs often occurred for Grades 2 to 4. Some lesions might be overestimated on TOF-MRA, while on zTE-MRA, the stenosis was equal to that on CTA (Fig.2).
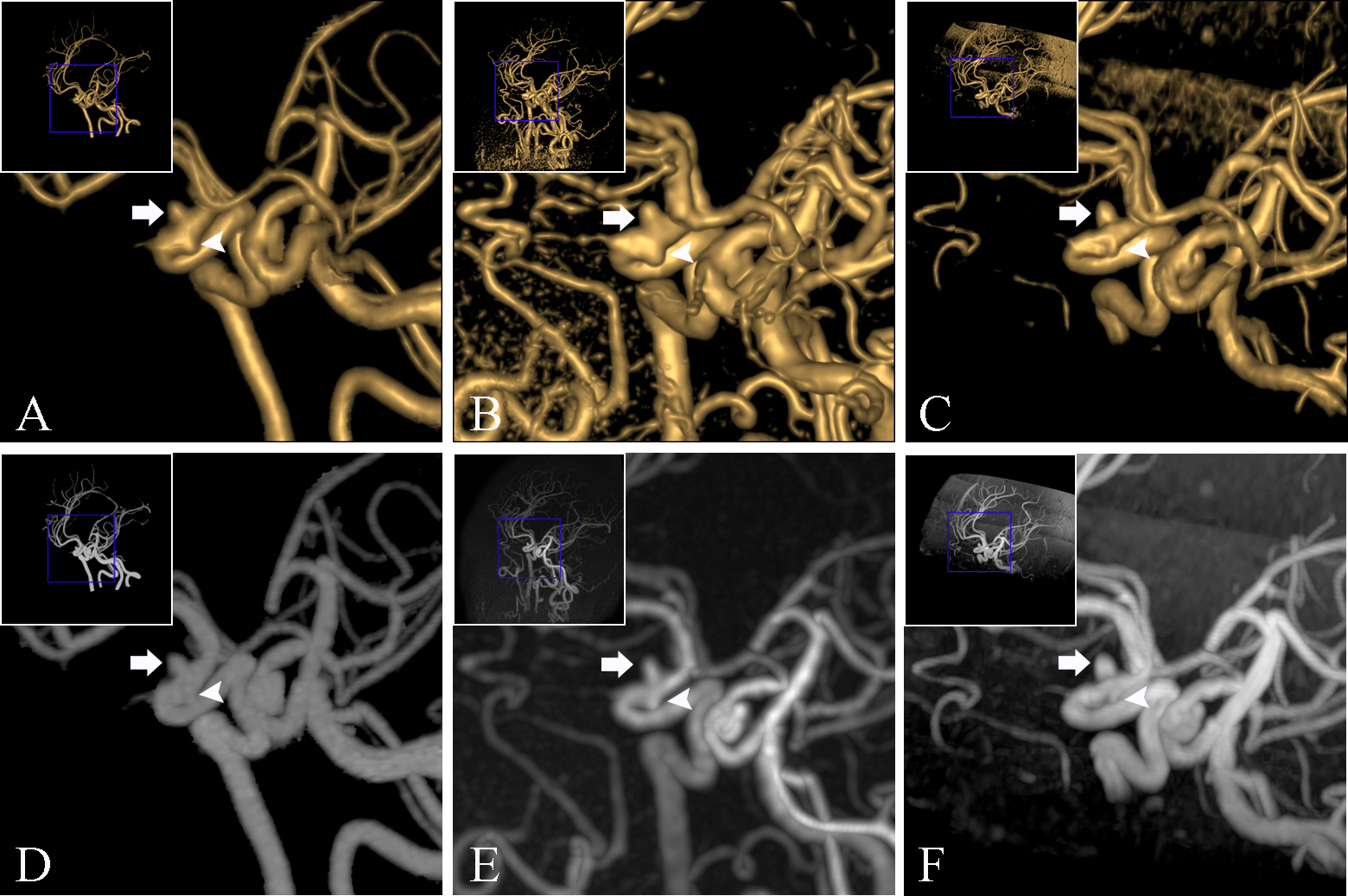
For Group small, the correlation coefficients between MRAs and CTA were 0.84 and 0.74, respectively, while they were 0.98 and 0.95 for Group large. zTE-MRA was thus more sensitive than TOF-MRA in the depiction of small aneurysms (Fig.3).
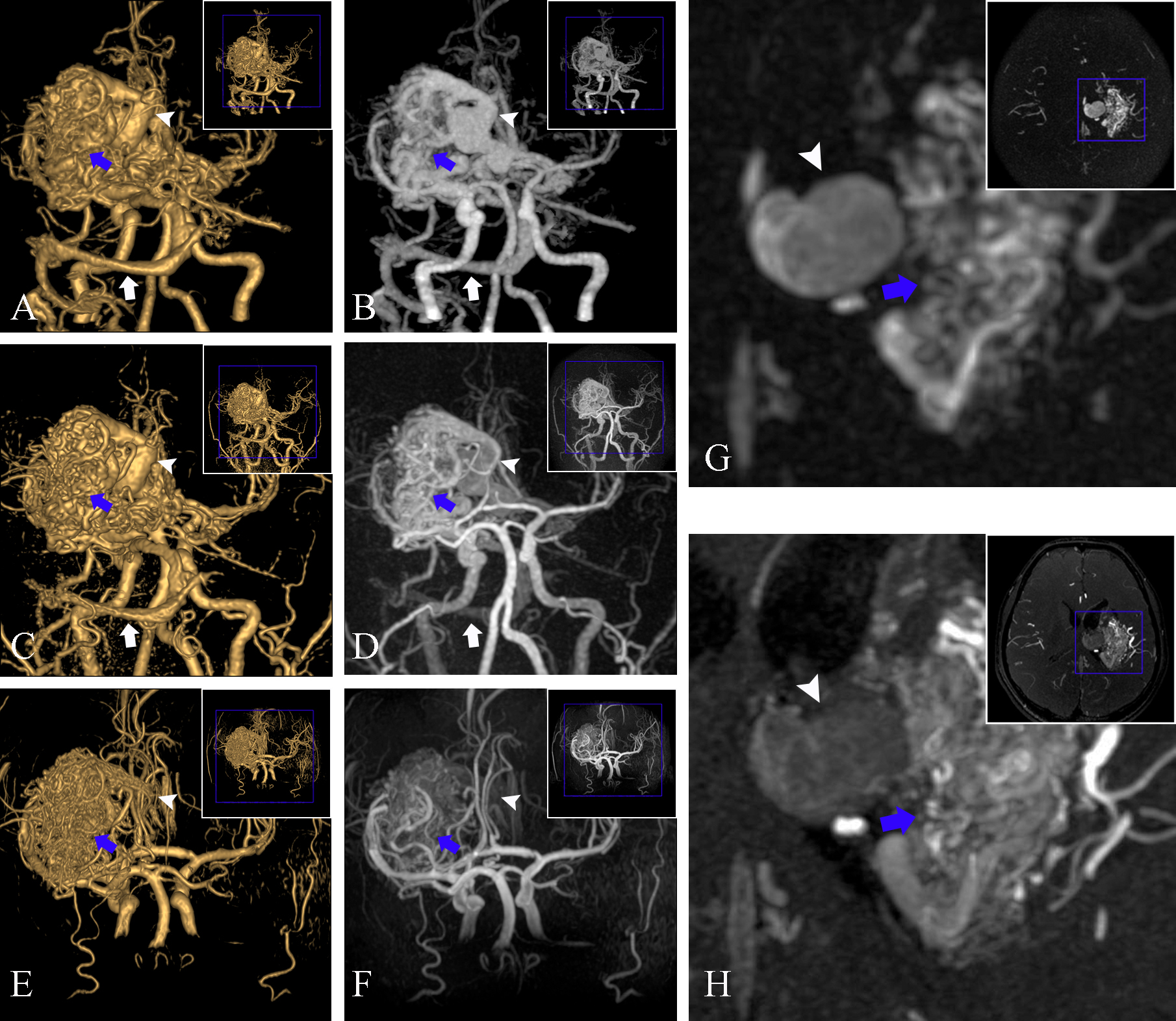
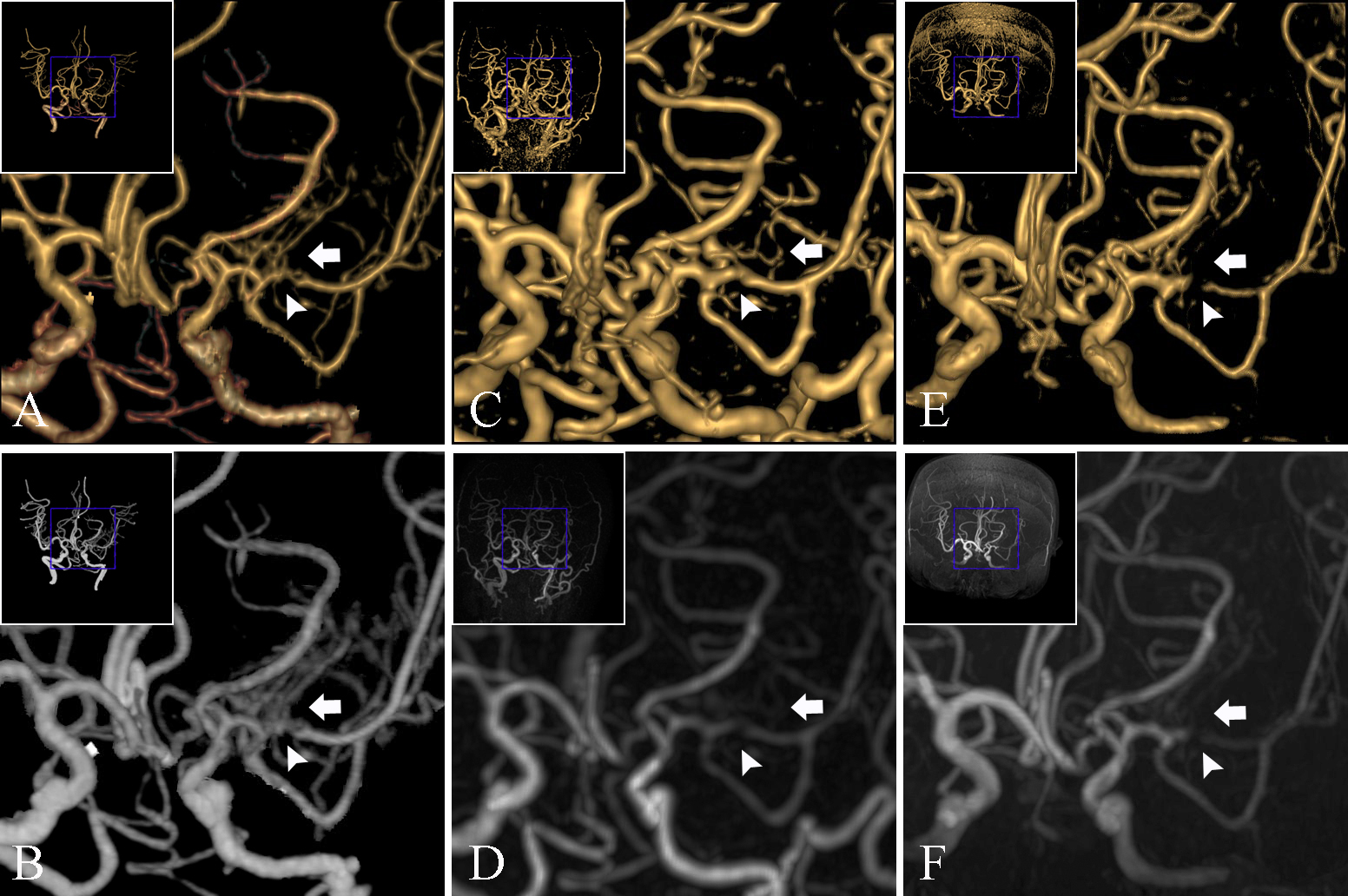
In addition, all 2 AVM patients and 3 moyamoya patients could be diagnosed using both MRAs. zTE-MRA however, showed more accurate details than TOF-MRA using CTA as a reference (Figs.4-5).
Discussion and conclusion
In this study, zTE-MRA, relative to TOF-MRA, showed more robust performance in depicting cerebrovascular diseases with dramatically reduced acoustic noise, higher signal homogeneity, less venous signal/artifact and higher inter-modality agreement and correlation with CTA.
Furthermore, due to its intrinsic characteristics, zTE-MRA has less vulnerability to blood flow disturbances, reduced risk of movement artefacts, and large coverage with additional findings.
In conclusion, zTE-MRA can be demonstrated to be a promising MRA technique to be further applied routinely in the clinic for patients with cerebrovascular diseases.
Acknowledgements
No acknowledgement found.References
1. Bash S, Villablanca JP, Jahan R, et al. Intracranial Vascular Stenosis and Occlusive Disease: Evaluation with CT Angiography, MR Angiography, and Digital Subtraction Angiography. Ajnr Am J Neuroradiol. 2005;26 (5):1012-1021.
2. Irie R, Suzuki M, Yamamoto M, et al. Assessing Blood Flow in an Intracranial Stent: A Feasibility Study of MR Angiography Using a Silent Scan after Stent-Assisted Coil Embolization for Anterior Circulation Aneurysms. AJNR Am J Neuroradiol. 2015;36 (5):967-970.
3. Takano N, Suzuki M, Irie R, et al.
Usefulness of Non-Contrast-Enhanced MR Angiography Using a Silent Scan for
Follow-Up after Y-Configuration Stent-Assisted Coil Embolization for Basilar
Tip Aneurysms. AJNR Am J Neuroradiol. 2017;38 (3):577-581.
Figures