2671
4D Flow MRI Analysis of Cerebral Blood Flow Before and After The Superficial Temporal Artery to Middle Cerebral Artery Bypass Surgery for Atherosclerotic Disease1Radiology, Nippon Medical School, Tokyo, Japan, 2Neurosurgery, Nippon Medical School, Tokyo, Japan, 3Radiology, Nihon University, Tokyo, Japan, 4Philips Electronics Japan Ltd, Tokyo, Japan
Synopsis
The purpose of this study was to clarify the change in the hemodynamics after superficial temporal artery to middle cerebral artery (STA-MCA) bypass surgery using 4D Flow MRI. We enrolled 20 patients who underwent 4D Flow MRI preoperatively and 3 weeks after the surgery. The blood flow volume (BFV) of ipsilateral STA and ipsilateral ICA significantly increased after the surgery (0.53±0.22 vs. 1.78±0.54 ml/sec (p< 0.001); 2.37±5.09 vs. 1.82±3.42 ml/sec (p=0.03)).
INTRODUCTION
The superficial temporal artery to middle cerebral artery (STA-MCA) bypass surgery failed to provide superior benefit to best medical therapy alone in the patients with the steno-occlusive cerebrovascular diseases (1). However, the subsequent analysis proved that the most of the complications (86%) in the surgical group were caused by nonbypass-related mechanisms (ischemic due to embolism, hypoperfusion etc.), not by bypass-related one. Beside, bypass surgery significantly improved oxygen extraction fraction and reduced the rate of recurrent ipsilateral ischemic stroke after postoperative day 2 compared with the medical group (9% vs. 22.7%) (2). Through this analysis, one can speculate that EC-IC bypass itself can well restore flow to hypoperfused brain territory in this cohort as it has been expected. From another point of view, the change in physiology after bypass surgery is interesting in order to understand the flow dynamics in the patients with insufficient blood flow in the brain.
Recently, time-resolved 3D-phase contrast (4D Flow) MRI has been tried to clarify the complicated cerebral blood flow(3-5). The purpose of this study was to clarify the change in the hemodynamics after STA-MCA bypass surgery by using 4D Flow MRI.
Methods
We enrolled 20 patients (14 men; mean age 63.9) with intracranial atherosclerotic steno-occlusive disease undergoing STA-MCA bypass surgery. The patient group included 10 internal carotid artery (ICA) lesions and 10 MCA lesions. The indication for STA-MCA bypass at our institution was based on SPECT examination with acetazolamide challenge where the stage Ⅱ hemodynamic impairment of the affected hemisphere was confirmed. We excluded moyamoya disease because its physiology differs from that of atherosclerotic steno-occlusive disease.
All patients underwent 4D Flow MRI preoperatively and 3 weeks after the surgery. The imaging parameters; 3.0-T MRI (Achieva, Philips), TR/TE = 8.4/5.4ms, flip angle = 13 degrees, k-space segmentation = 2, SENSE = 2, elliptical partial k-space coverage in phase- and slice-encoding direction, VENC = 100cm/sec, voxel size = 0.82X0.82X1.4mm, heart phase = 15, scan time = approx. 6 min (3,4).We measured blood flow volume (BFV) of bilateral ICAs, basilar artery (BA), and bilateral STAs using GT Flow (GyroTools, Zurich, Switzerland). The measurement was performed by using the semi-automatic iso-contour mode on the three sequential planes of the target vessel, which were resliced perpendicularly to the target artery points. BFV was calculated by averaging these three values.
The BFV of each vessel and total brain BFV (total-BFV = bilateral ICAs + BA + ipsilateral STA (after surgery)) were compared between before and after surgery with the paired t-test. We evaluated postoperative hyperperfusion syndrome and recurrent stroke based on clinical symptoms.
Results
Patency of the bypass artery was confirmed in all patients using TOF-MRA and 4D Flow MRI. Results of the BFV analysis are summarized in Figure 1 and 2. BFV of ipsilateral STA significantly increased after surgery (0.53 ± 0.22 vs. 1.78 ± 0.54 ml/sec (p < 0.001)). BFV of ipsilateral ICA significantly decreased after surgery (2.37 ± 5.09 vs. 1.82 ± 3.42 ml/sec (p = 0.03)). While, no significant difference was observed in total-BFV (12.40 ± 5.55 vs. 12.94 ± 6.71 ml/sec (p = 0.24)) or BFV of contralateral ICA (5.14 ±5.87 vs. 4.72 ± 4.60 ml/sec (p = 0.06)), BFV of BA (4.89 ± 2.89 vs. 4.61 ±2.48 ml/sec (p = 0.11)), and BFV of contralateral STA (0.33 ± 0.06 vs. 0.40 ±0.06 ml/sec (p = 0.07)) between before and after surgery.
Hyperperfusion syndrome occurred in 1 case (Figure 3). In the patient, total-BFVincreased by 13.2% (from 13.90 ml to 15.74 ml). The increased volume was mainly derived from the markedly high-flow STA-bypass artery (BFV of ipsilateral STA after the surgery was 3.03 ml).
Conclusion
4D Flow MRI revealed that BFV of ipsilateral STA significantly increased and total BFV didn’t change after EC-IC bypass surgery in the patients with the atherosclerotic steno-occlusive disease. It may indicate that the blood flow via ipsilateral STA bypass does not simply add the blood flow volume to the brain. The bypass artery and the native intracranial arteries (i.e., bilateral ICAs and BA) supply blood flow complementarily after surgery.Acknowledgements
This work was supported by PMOD Technologies LLC and with Fujifilm corporation regarding 4D Flow MRI software development. And it was also supported by investigator-initiated study grants from Hitachi Global Foundation, Fukuda Foundation for Medical Technology and Terumo foundation for life sciences and arts.References
1. Powers WJ, Clarke WR, Grubb RL, Jr., et al. Extracranial-intracranial bypass surgery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Surgery Study randomized trial. JAMA. 2011;306:1983-1992.
2. Esposito G, Amin-Hanjani S, Regli L. Role of and Indications for Bypass Surgery After Carotid Occlusion Surgery Study (COSS)? Stroke. 2016;47:282-290.
3. Orita E, Murai Y, Sekine T, et al. Four-Dimensional Flow MRI Analysis of Cerebral Blood Flow Before and After High-Flow Extracranial-Intracranial Bypass Surgery With Internal Carotid Artery Ligation. Neurosurgery. 2018.
4. Sekine T, Takagi R, Amano Y, et al. 4D flow MRI assessment of extracranial-intracranial bypass: qualitative and quantitative evaluation of the hemodynamics. Neuroradiology. 2016;58:237-244.
5. Sekine T, Takagi R, Amano Y, et al. 4D Flow MR Imaging of Ophthalmic Artery Flow in Patients with Internal Carotid Artery Stenosis. Magn Reson Med Sci 2018;17:13-20.
Figures

Figure 1
Data presented as mean ± SD (mL/s).
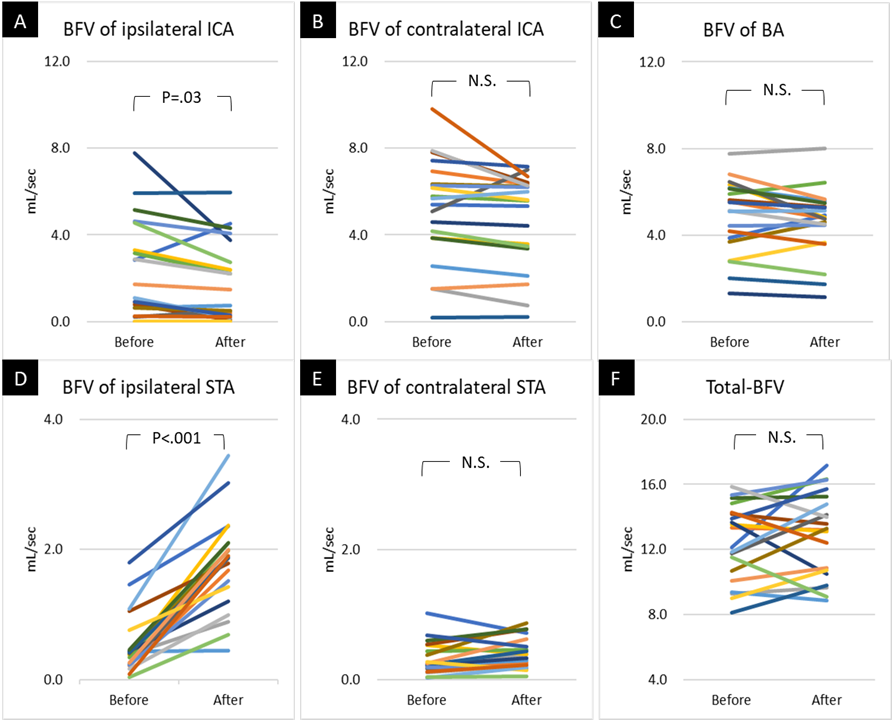
Figure 2
A~F: Graphs show the comparison of BFV between before and 3 weeks after STA-MCA bypass surgery. BFV of ipsilateral ICA significantly decreased after surgery (A). BFV of ipsilateral STA significantly increased after surgery (D).
Abbreviations: BA = basilar artery, BFV = blood flow volume, ICA = internal carotid artery, MCA = middle cerebral artery, STA = superficial temporal artery
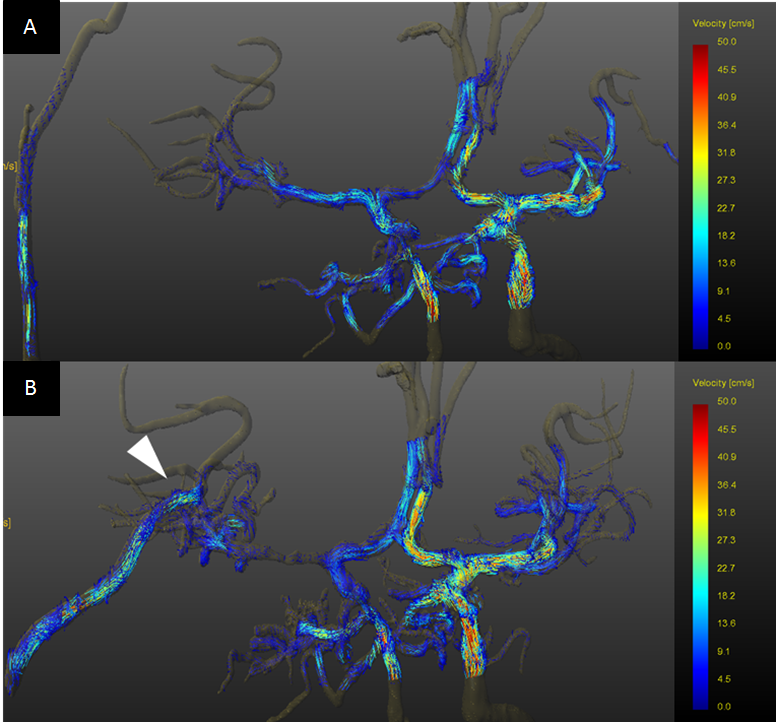
Figure 3
A 62-year-old male with right ICA occlusion. He underwent right STA-MCA bypass surgery (white arrowhead). 4D Flow MRI was performed preoperatively (A) and 3 weeks after the surgery (B). The BFV of ipsilateral STA and that of total-BFV increased after the surgery. Postoperative hyperperfusion syndrome was observed in this case.
Abbreviations: BFV = blood flow volume, ICA = internal carotid artery, MCA = middle cerebral artery, STA = superficial temporal artery