2665
Dual Coil Continuous ASL of the human brain at 9.4 T1Magnetic Resonance Center, Max Planck Institute for Biological Cybernetics, Tübingen, Germany, 2Biomedical Magnetic Resonance, University of Tübingen, Tübingen, Germany
Synopsis
Arterial Spin Labeling (ASL) is expected to profit highly from ultra high magnetic fields because of the high SNR and the long longitudinal relaxation time. Here we show first images from dual coil continuous ASL measurements in the human brain at 9.4 T. A separate transmit channel was established to feed two small labeling coils placed at the neck. A power limiter was used to ensure subject safety. First images show strong perfusion contrast and high SNR.
Introduction
Arterial Spin Labeling (ASL) is an established technique to measure the perfusion in the brain and other organs by labeling the inflowing blood. In spite of the limited sensitivity of this technique and the correspondingly large voxel sizes and long scan times, numerous applications for quantitative perfusion imaging in clinical applications or for functional measurements in neuroscience have been reported. Due to the high SNR and the long longitudinal relaxation times, ultra high field strengths are expected to boost the quality of ASL measurements1. However, so far only limited improvements of perfusion measurements with ASL at high field strengths were shown. Reasons for this may be the high SAR of most ASL techniques, the strong transmit field inhomogeneities at high field strengths and the lack of large body coils that are able to label a large part of the head. A solution to some of these problems may be Dual Coil Continuous ASL (DC-CASL)2, where the blood is labeled by small local coils positioned at the neck of the subject, using flow-driven adiabatic inversion as the blood enters the brain through the carotid arteries. Here, we present the first DC-CASL measurements at a field strength of 9.4 T.Methods
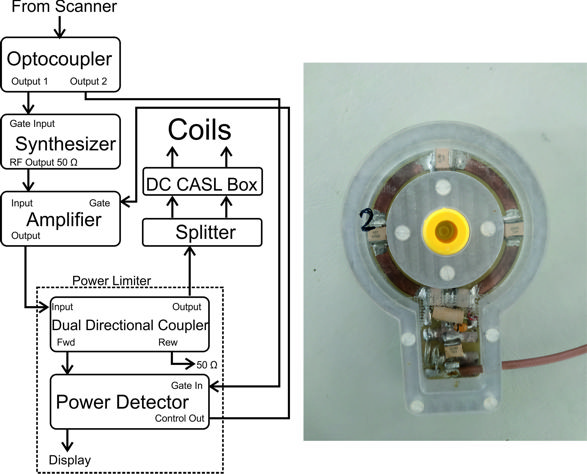
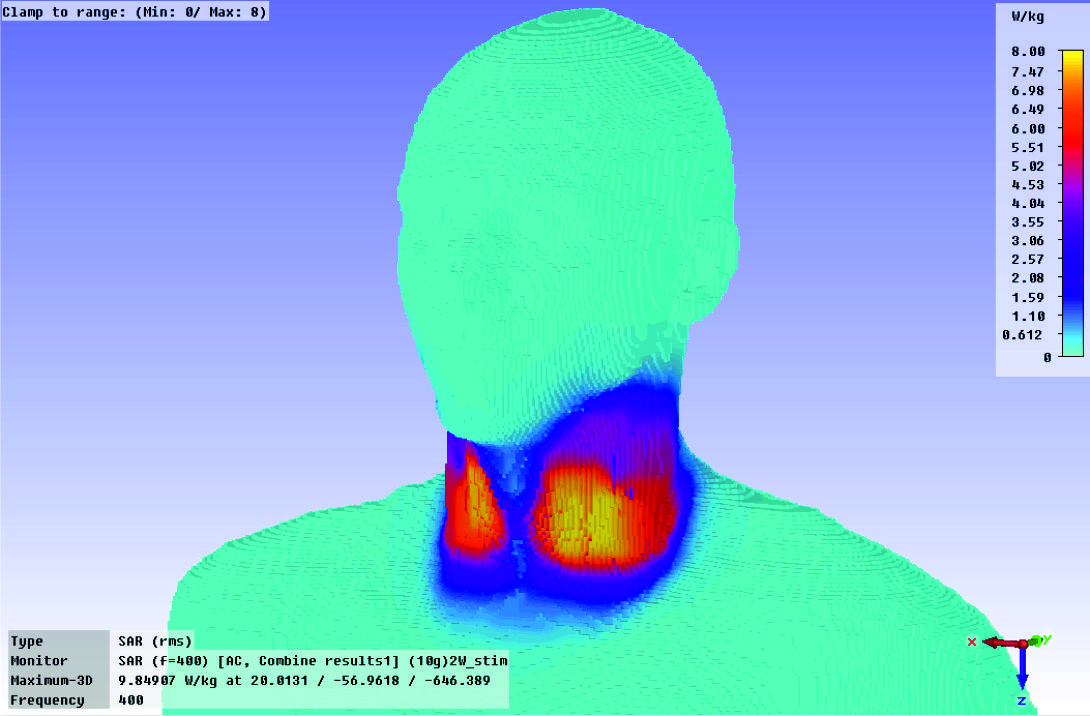
Measurements were performed on a Siemens 9.4 T human scanner. Two local surface coils3 with a diameter of 5 cm each were placed at the neck of the subject, just above the carotid arteries. They were connected to a separate, external transmit channel, basically consisting of an rf-synthesizer, a power amplifier and a splitter to distribute the rf to the two coils (see Fig. 1). A trigger signal from the pulse sequence controlled the labeling pulse. Since the external amplifier was not monitored by the scanner’s SAR supervision, safety was a crucial factor in this setup. To ensure compliance with the approved SAR limits, careful SAR simulations of the coils were performed (Fig. 2). Using their output, including a 50% safety margin, the pulse sequence calculated the maximum allowed power to be set on the transmit channel, taking into account the rf duty cycle of the measurement and the attenuation in the long transmit cables. For additional safety, a home-built power limiter was inserted into the transmit line, which blanked the amplifier, whenever the power exceeded the sequence dependent limit or if the amplifier transmited erroneously. This prevented damage of the subject in case of amplifier malfunction.
For imaging, the head of the subject was positioned inside a head coil with 8 transmit and 16 receive channels. An EPI sequence (TE = 9 ms, TR = 4 s, matrix size = 74×74, voxel size = (3 mm)3, GRAPPA factor = 3, Partial Fourier) with alternate tag and control scans was used for perfusion imaging. 25 repetitions of the tag/control pair were acquired within 3.3 min, with a labeling duration of 1.5 s and an inversion delay of 1.8 s. The optimum values for the rf power and the strength of the gradient applied for inversion were estimated using Bloch equation simulations4.
Results
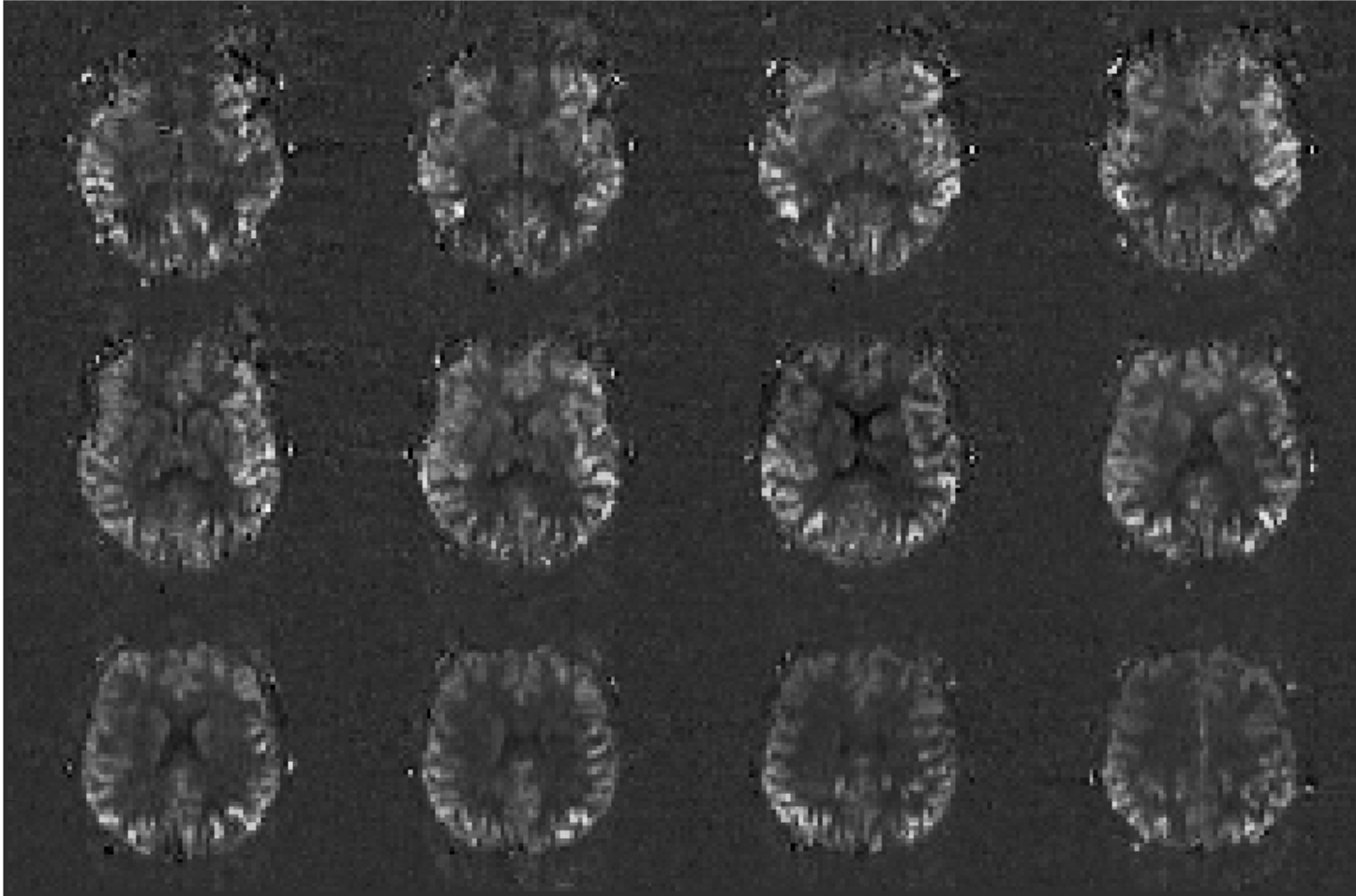
First images acquired with DC-CASL at 9.4 T are shown in Fig. 3. Although the inversion parameters have not yet been fully optimized, the images show strong perfusion contrast and high SNR, which will make higher spatial or temporal resolutions possible.Discussion
The high SNR and the long T1 at 9.4 T should provide excellent conditions for highly sensitive ASL measurements. Our results indicate that using the dual coil ASL approach, it may be possible to realize these advantages to obtain perfusion images with high spatial resolution. Compared to pulsed arterial spin labeling1, this technique has the advantages of avoiding slice profile effects, reducing SAR, since no inversion pulse is needed for the control scan, and being independent of the covered volume of the head coil. Due to the small size of the labeling coil, an accurate prediction of the inversion efficiency and hence a quantitative perfusion measurement may be difficult. Possible first applications thus will be based on measuring changes of perfusion, e.g. in functional studies.Conclusion
Our preliminary data indicates that dual coil CASL at 9.4 T is possible within the SAR limits and has the potential to yield high-resolution perfusion images.Acknowledgements
No acknowledgement found.References
1: Zaharchuk, G., et al. (1999). "Multislice perfusion and perfusion territory imaging in humans with separate label and image coils." Magnetic Resonance in Medicine 41(6): 1093-1098.
2: Bause, J., et al. (2016). "Quantitative and functional pulsed arterial spin labeling in the human brain at 9.4 T." Magnetic Resonance in Medicine 75(3): 1054-1063.
3. Bause J., et al. (2012)., “Design and SAR Estimation of a Segmented Loop for Dual Coil CASL at 9.4 T”, ISMRM 2012, Melbourne, Australia
4. Bause J., et al., (2015). “Simulation of flow driven adiabatic inversion in dual coil CASL at 9.4 T.” ESMRMB 2015, Edinburgh, UK, 28(1 Supplement) S367-S368
Figures