2660
Synthetic MR Angiography: A Feasibility Study of MR Angiography based on 3D Synthetic MRI1Department of Radiology, Juntendo University, Tokyo, Japan, 2Department of Radiology, The University of Tokyo, Tokyo, Japan, 3Milliman Inc., Tokyo, Japan
Synopsis
Quantitative synthetic MRI allows
Introduction
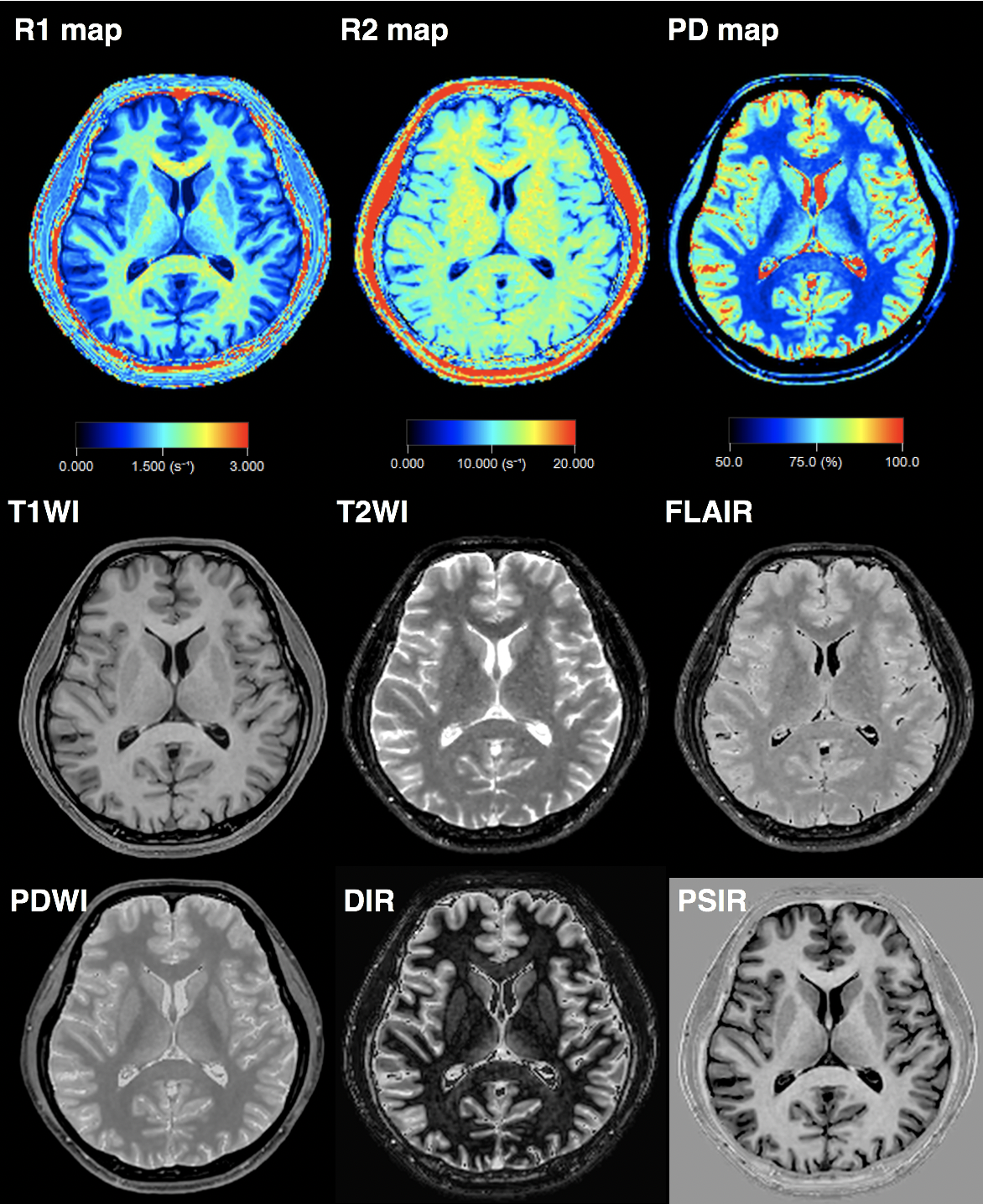
Quantitative synthetic MRI enables simultaneous quantification of T1 and T2 relaxation times and proton density (PD) with high reliability using Bloch equation.1 Based on these quantification maps, quantitative synthetic MRI also allows creation of various contrast-weighted image that is used routinely in clinical settings (Fig. 1).2,3 Thus, synthetic MRI may not only allow access to quantitative imaging but allow reduction of examination time.
However, up until now, clinically widely used MR angiography (MRA) images were unable to obtain using synthetic MRI. Here, we demonstrate the capability of 3D-QALAS (3D- quantification using an interleaved Look-Locker acquisition sequence with T2 preparation pulse) sequence4,5 to generate MRA-like images, without addition of extra scanning time.
Methods
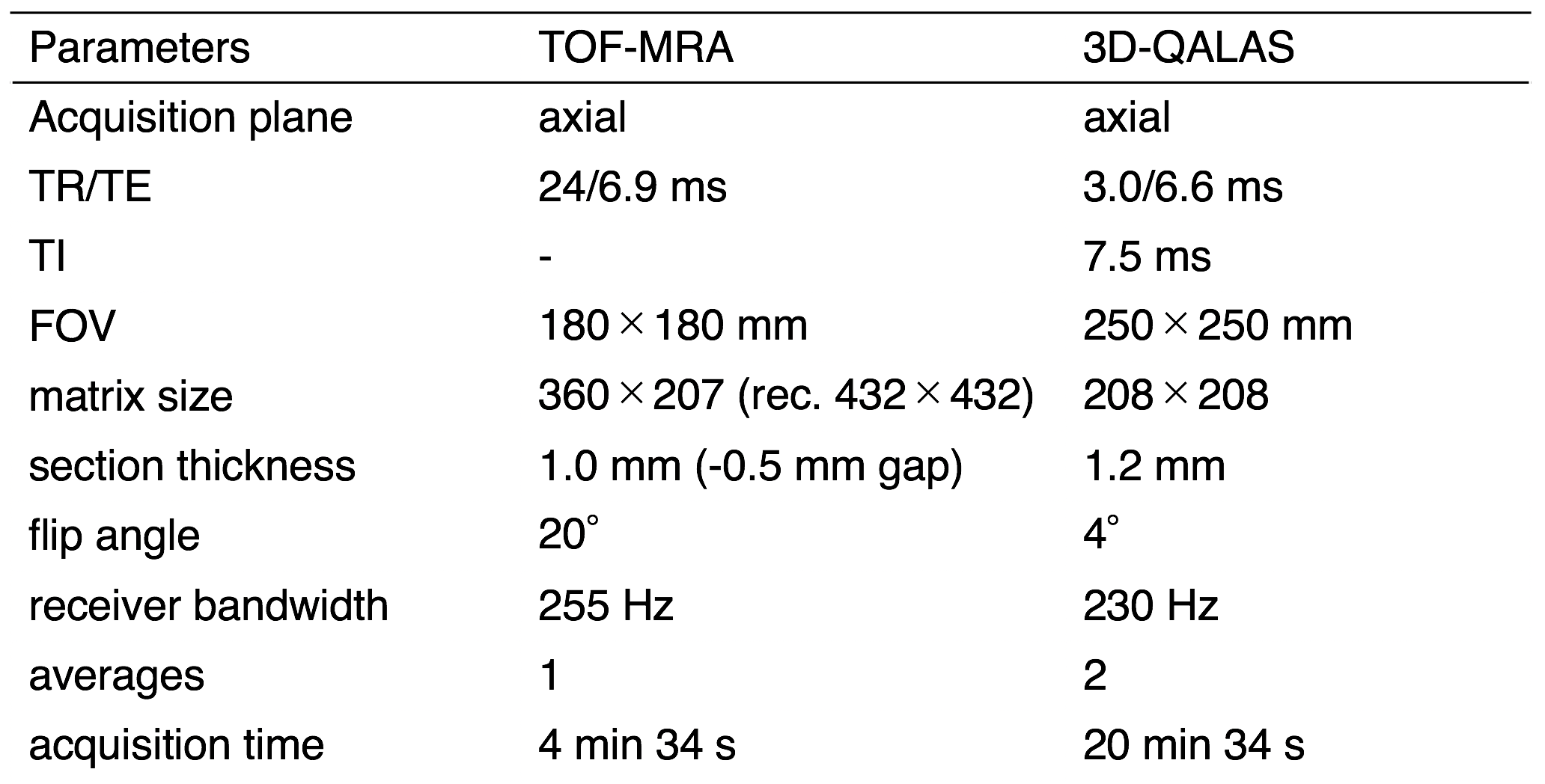
Eight Neurologically healthy volunteers were scanned on a 1.5 T scanner (A patched R5.3.0 Ingenia, Philips Healthcare, Best, The Netherlands) with a 12-channel head coil. Time of flight MRA (TOF-MRA) and 3D-QALAS sequence were performed in the same session on all the participants (Table 1). 3D-QALAS is based on multi-acquisition 3D gradient echo, with 5 acquisitions equally spaced in time, interleaved with a T2 preparation pulse and an inversion pulse. Therefore, a total of 5 original images are produced for each slice.
Our goal was to find the linear combination of the original 5 images of 3D-QALAS sequence that maximizes the signal intensity difference between artery and background. For each image, circular regions of interest were manually placed on the bilateral middle cerebral artery, white matter, gray matter, and CSF. These representative signal intensities were analyzed based on linear algebra to obtain 5 coefficients that maximize the signal intensity difference between artery and background. Synthetic MRA was produced by a linear combination of the original 5 images using coefficients obtained above (Fig. 2).
Two radiologists independently evaluated visualizations of major cerebral arteries on synthetic MRA and compared them with TOF-MRA subjectively on a five-point scale as shown in Table 2. An interrater reliability coefficient was calculated using squared weighted Cohen’s Kappa test after pooling the results from synthetic MRA and TOF-MRA considering all the locations of arteries. For quantitative evaluation, the signal-to-noise ratio (SNR) of ICA on synthetic MRA and TOF-MRA was calculated using the following formula: SNR = SIICA/ SDbackground, where SIICA is the mean signal intensity in the region of interest placed on the cavernous portion of ICA and SDbackground is the standard deviation in the brain parenchyma. Paired t-test was performed to compare SNRs of both sequences.
Results
In all volunteers, synthetic MRAs were successfully obtained from 3D-QALAS raw images. A representative image is shown in Figure 3. The mean scores evaluated by the first neuroradiologist were 2.6±0.7, 2.8±0.5, 2.5±0.5, 2.4±0.5, and 2.9±0.4, respectively, for the ICA, MCA, ACA, PCA, and BA (values represent mean score±SD). SNR of ICA showed no significant difference between TOF-MRA (9.47±2.24, mean±SD) and synthetic MRA (10.24±3.49) (p=0.814). Considering synthetic MRA and TOF-MRA for all locations of arteries, the agreement between the two neuroradiologists was substantial, with the squared weighted Cohen’s Kappa coefficient being 0.74 (p < 0.05).Discussion
This study demonstrated the capability of 3D-QALAS sequence to visualize main parts of intracranial arteries in volunteers without additional scanning. ICA, VA, BA, ACA, MCA, and PCA were clearly visualized in synthetic MRA, with comparable quality to that of TOF-MRA. Synthetic MRA may function as a screening tool to detect lesions of major intracranial arteries (eg, aneurysm, occlusion, stenosis), without additional scan time. However, visualization of distal segments of intracranial arteries (eg, A3, M3/4, P3/4) were generally inferior to TOF-MRA. TOF-MRA should be added to obtain reliable morphological information for detailed analysis.
The limitation of this study was that no patient was included. Complex blood flow in lesions such as brain aneurysm, stenosis, arteriovenous malformations, and intratumoral shunt could affect signal intensities, and thus may derange the quality of the proposed MRA-like images. Further investigation is needed before being introduced into clinical practice. Another limitation is the long scanning time in this study, making it difficult to use in clinical settings. Further research may be useful that combines synthetic MRI with techniques such as compressed sensing6 and multi-band method7 to further reduce scan time to a clinically applicable level.
Conclusion
In volunteers, 3D synthetic MRA allowed visualizing major intracranial arteries as efficient as TOF MRA, without additional scanning. Synthetic MRA might be useful for screening and may reduce total scan time, even though this study’s results are only preliminary due to some limitations.Acknowledgements
This work was supported by the program for Brain Mapping by Integrated Neurotechnologies for Disease Studies (Brain/MINDS) from Japan Agency for Medical Research and development, AMED; ImPACT Program of Council for Science, Technology and Innovation (Cabinet Office, Government of Japan); JSPS KAKENHI grant number 16K19852; JSPS KAKENHI Grant Number JP16H06280, Grant-in-Aid for Scientific Research on Innovative Areas- Resource and technical support platforms for promoting research ’Advanced Bioimaging Support’.References
1. Hagiwara A, Hori M, Cohen-Adad J, Nakazawa M, Suzuki Y, Kasahara A, et al. Linearity, Bias, Intra-Scanner Repeatability, and Inter-Scanner Reproducibility of Quantitative Multi-Dynamic Multi-Echo Sequence for Rapid Simultaneous Relaxometry at 3T: A Validation Study with a Standardized Phantom and Healthy Controls. Invest Radiol. 2018 [in press].
2. Tanenbaum LN, Tsiouris AJ, Johnson AN, Naidich TP, DeLano MC, Melhem ER, et al. Synthetic MRI for Clinical Neuroimaging: Results of the Magnetic Resonance Image Compilation (MAGiC) Prospective, Multicenter, Multireader Trial. AJNR Am J Neuroradiol. 2017;38(6):1103-10.
3. Blystad I, Warntjes JB, Smedby O, Landtblom AM, Lundberg P, Larsson EM. Synthetic MRI of the brain in a clinical setting. Acta Radiol. 2012;53(10):1158-63.
4. Kvernby S, Warntjes MJ, Haraldsson H, Carlhall CJ, Engvall J, Ebbers T. Simultaneous three-dimensional myocardial T1 and T2 mapping in one breath hold with 3D-QALAS. J Cardiovasc Magn Reson. 2014;16:102.
5. Kvernby S, Warntjes M, Engvall J, Carlhall CJ, Ebbers T. Clinical feasibility of 3D-QALAS - Single breath-hold 3D myocardial T1- and T2-mapping. Magn Reson Imaging. 2017;38:13-20.
6. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58(6):1182-95.
7. Feinberg DA, Moeller S, Smith SM, Auerbach E, Ramanna S, Gunther M, et al. Multiplexed echo planar imaging for sub-second whole brain FMRI and fast diffusion imaging. PLoS One. 2010;5(12):e15710.
Figures