2651
Deep Learning Augmented Cerebral Blood Flow Measurement Using Arterial Spin Labeling Technique in Moyamoya Disease Before and After Direct Bypass Surgery1Radiology, Stanford University, Palo Alto, CA, United States, 2Medical Imaging, Shuan-Ho Hospital, Taipei Medical University, New Taipei City, Taiwan, 3Neurosurgery, Tokyo Medical and Dental University, Tokyo, Japan, 4Bioengineering, University of California Riverside, Riverside, CA, United States
Synopsis
We used single-delayed (SD) pseudo-continuous arterial spin labeling (PCASL), multi-delay (MD) ASL and a new, synthesized (Synth) ASL to longitudinally monitor cerebral blood flow (CBF) before and after direct bypass surgery in Moyamoya disease. The Synth-ASL was generated from a deep convolutional neural network, previously trained on a simultaneous [15O]-water PET/MRI dataset to generate a PET-like CBF map from MRI inputs. The Synth-ASL demonstrated a more homogenous CBF change across the brain and significantly greater CBF increase globally and regionally than SD-ASL and MD-ASL after surgery. Synth-ASL reduces bias in long arterial delay and measurement noise, and may enable robust CBF imaging follow-up in cerebrovascular patients.
Purpose:
Accurate measurement of the cerebral blood flow (CBF) is important in the evaluation and longitudinal monitoring of disease status in Moyamoya disease. Arterial spin labeling (ASL) is a promising, noninvasive method for measurement of CBF. However, conventional single-delay (SD) ASL is difficult to use in patients with prolonged arterial transit times (ATT) [1]. Multi-delay (MD) ASL can detect ATT and improve the accuracy of CBF measurement, but still faces challenges in regions with very long ATT in Moyamoya disease [1]. [15O]-water positron-emission tomography (PET) is considered reference standard for CBF measurement. We previously developed a deep convolutional neural network (dCNN) model, trained on a simultaneous [15O]-water PET/MRI studies of Moyamoya patients and healthy subjects, to generate synthesized CBF maps. The model took multiple MRI images (including ASL and structural images) as input, and learned from the simultaneously acquired [15O]-water PET CBF as the reference. The synthesized (Synth) ASL showed improved image quality and quantification accuracy [2]. The study has two goals, 1) to longitudinally evaluate CBF in Moyamoya patients before and after direct bypass surgery using SD-ASL, MD-ASL and Synth-ASL and 2) to compare CBF between the different ASL methods.Methods:
Subjects: 8 patients (mean age 36.4 years, 5 females) with bilateral Moyamoya disease were included in this retrospective study. Three patients received right-sided and 5 received bilateral direct bypass surgery during the study period.
Image acquisition and processing: For each patient, MR images were acquired pre-operatively about 1 week before surgery and post-operatively several months (average 6.88 months, 4-9 months) after surgery. The perfusion images included a single-delay (SD) pseudo-continuous ASL (PCASL) with labeling duration (LD) = 1.45s and post-labeling delay (PLD) = 2.025s, and a multi-delay (MD) PCASL with LD = 2s and PLD = 0.7/1.275/1.85/2.425 and 3s. CBF maps were quantified with a one-tissue compartment model for SD-ASL [3]; and CBF and ATT maps were quantified with a two-tissue compartment model for MD-ASL [4]. Structural images included 3D high-resolution T1 and T2 FLAIR images. All MRI images were co-registered and normalized to a MNI template. We passed the preprocessed input images (including SD-ASL, MD-ASL, T1 and T2 images) into the pre-trained dCNN model to generate Synth-ASL maps.
Evaluation of longitudinal CBF change: CBF difference maps were calculated by subtracting the pre-operative CBF from the post-operative CBF image for each patient, and then averaging across subjects. Regional CBF values were calculated in ASPECTS regions of interests (ROIs) [5]. ROIs were grouped into those within the anterior circulation (ACA, MCA territories) of the treated hemispheres, in which CBF was considered to be directly affected by the bypass surgery, and ROIs of the posterior circulation (PCA territories), with a more indirect effect by surgery. Change of regional CBF before and after surgery was evaluated by paired t-test, and differences between SD-, MD- and Synth-ASL was assessed by one-way ANOVA with repeated measures.
Results:
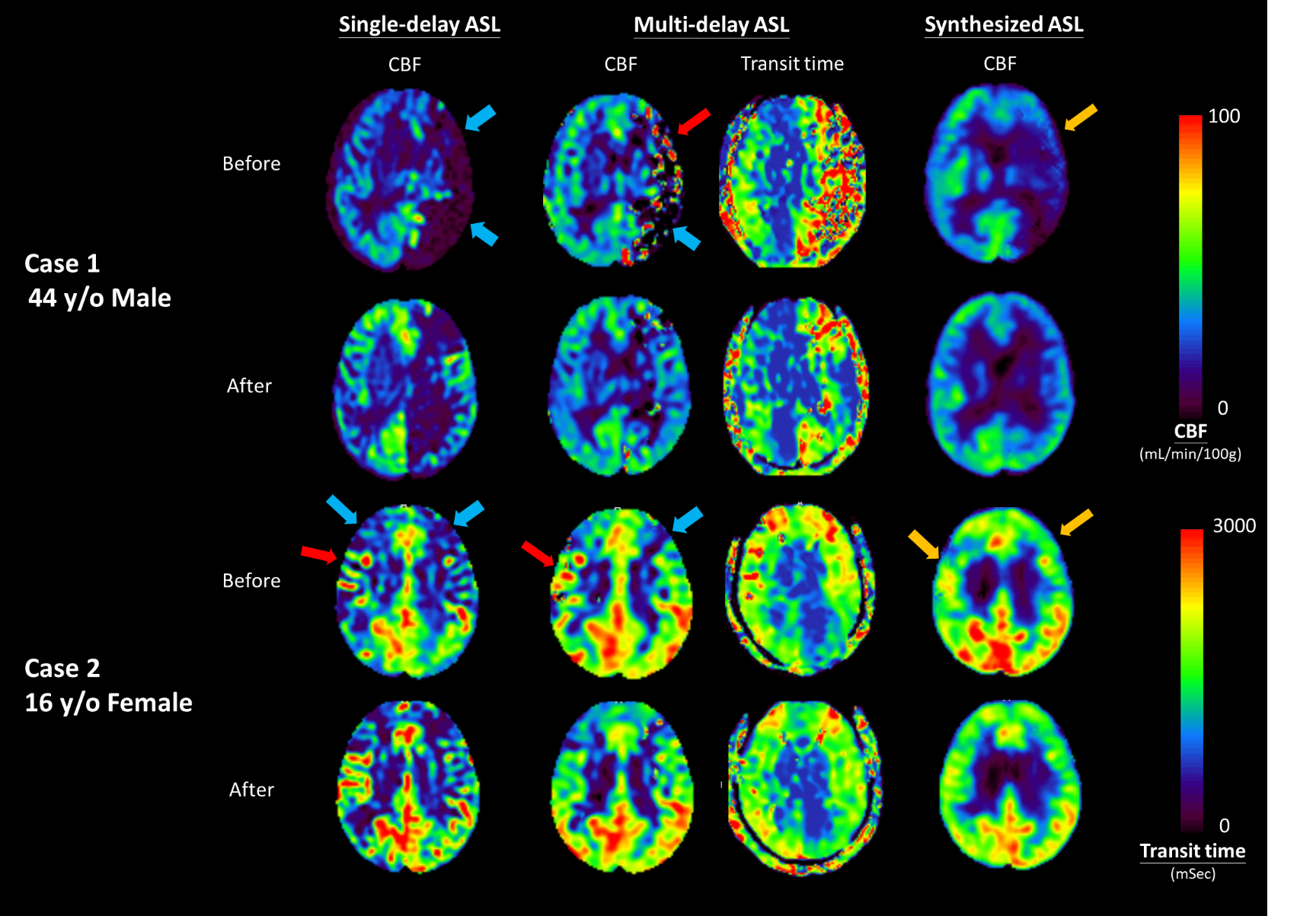
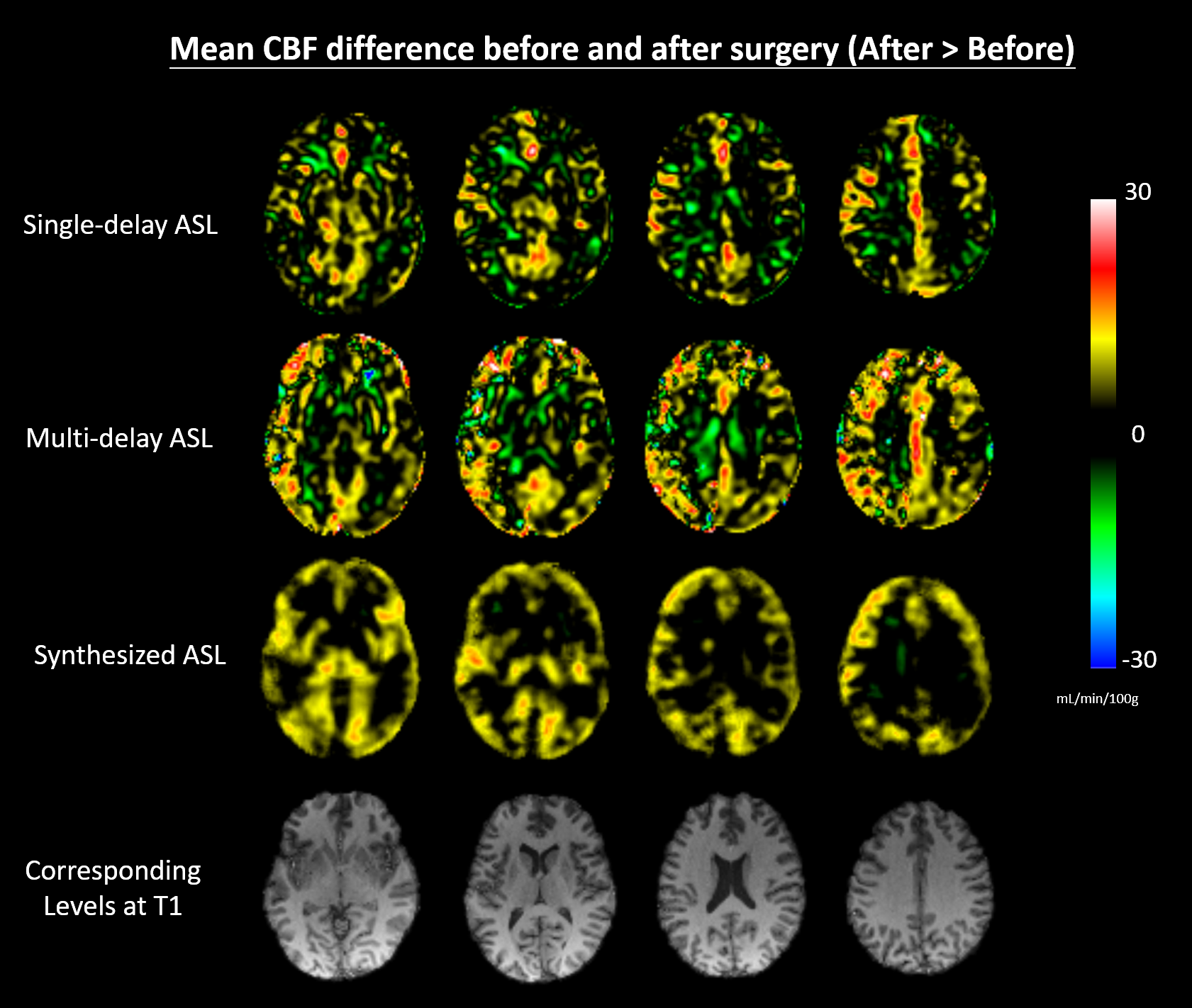
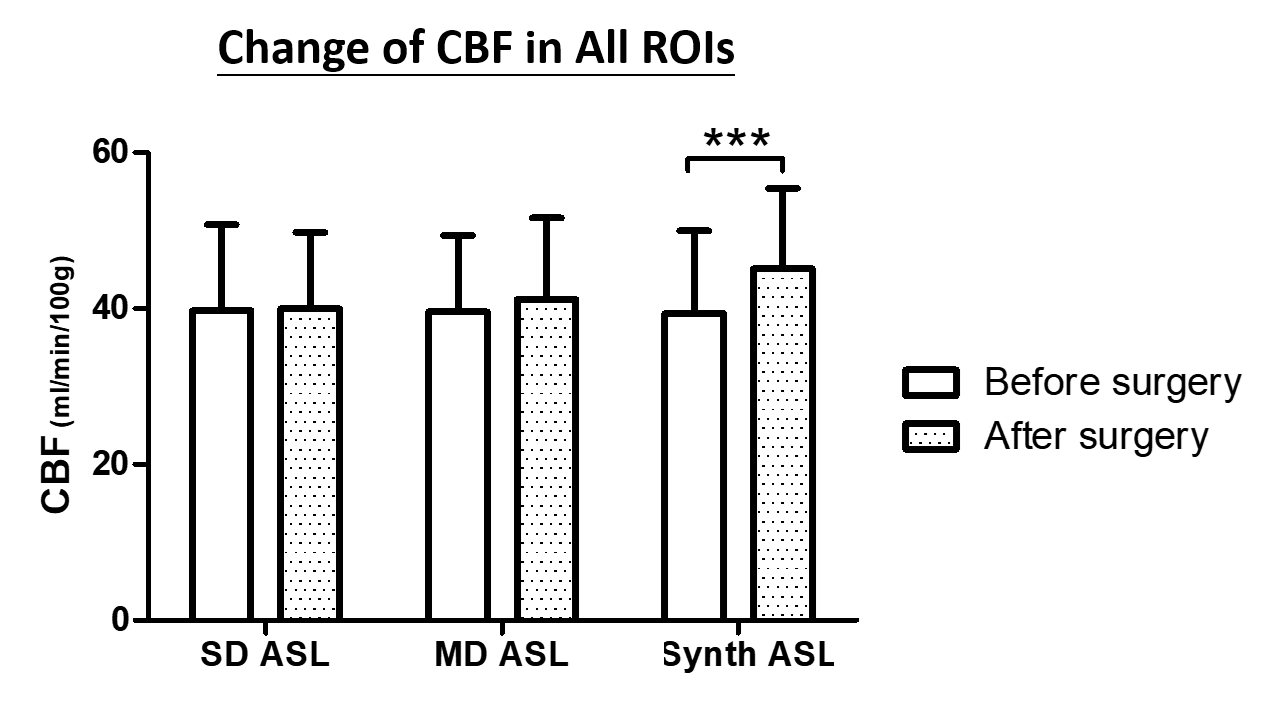
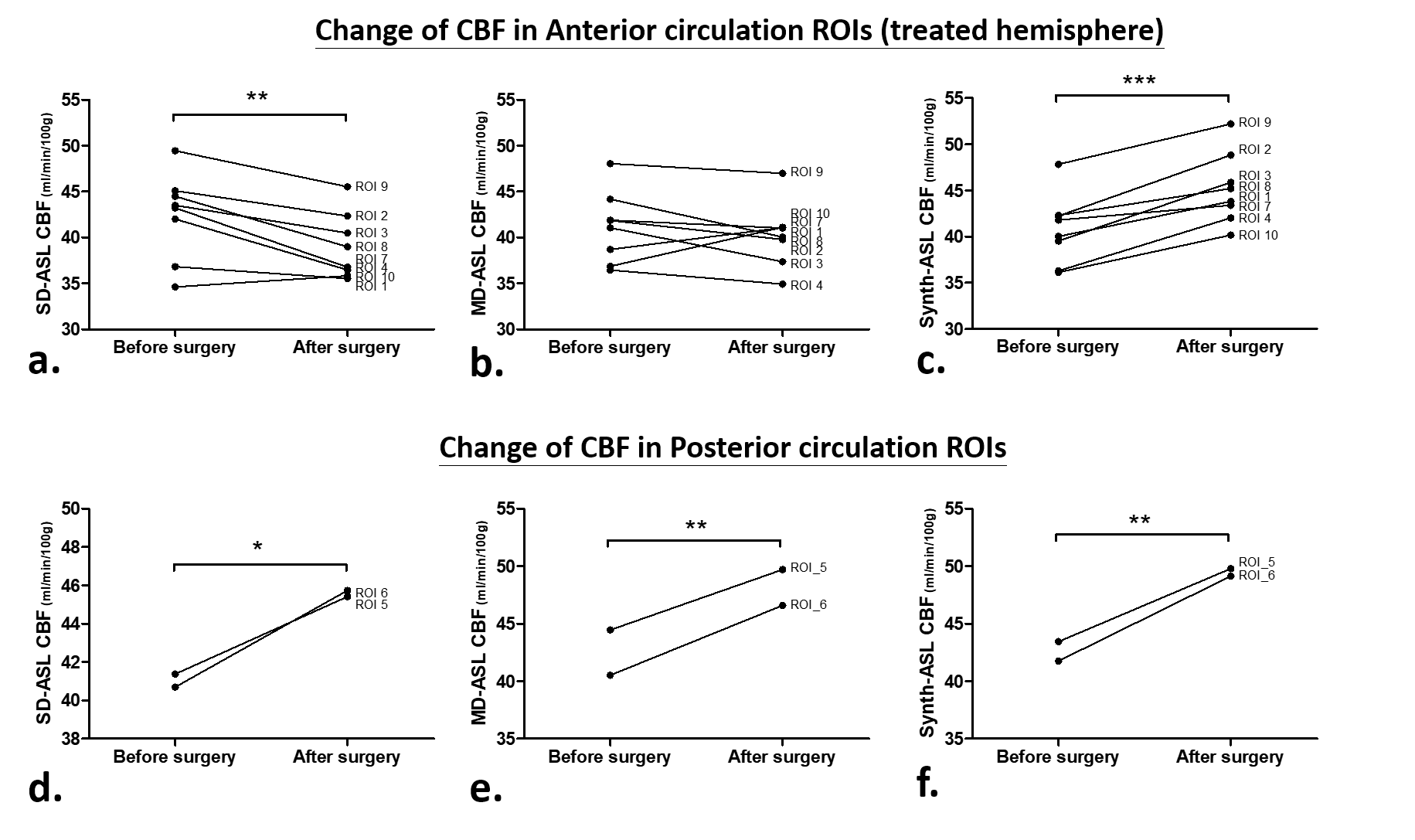
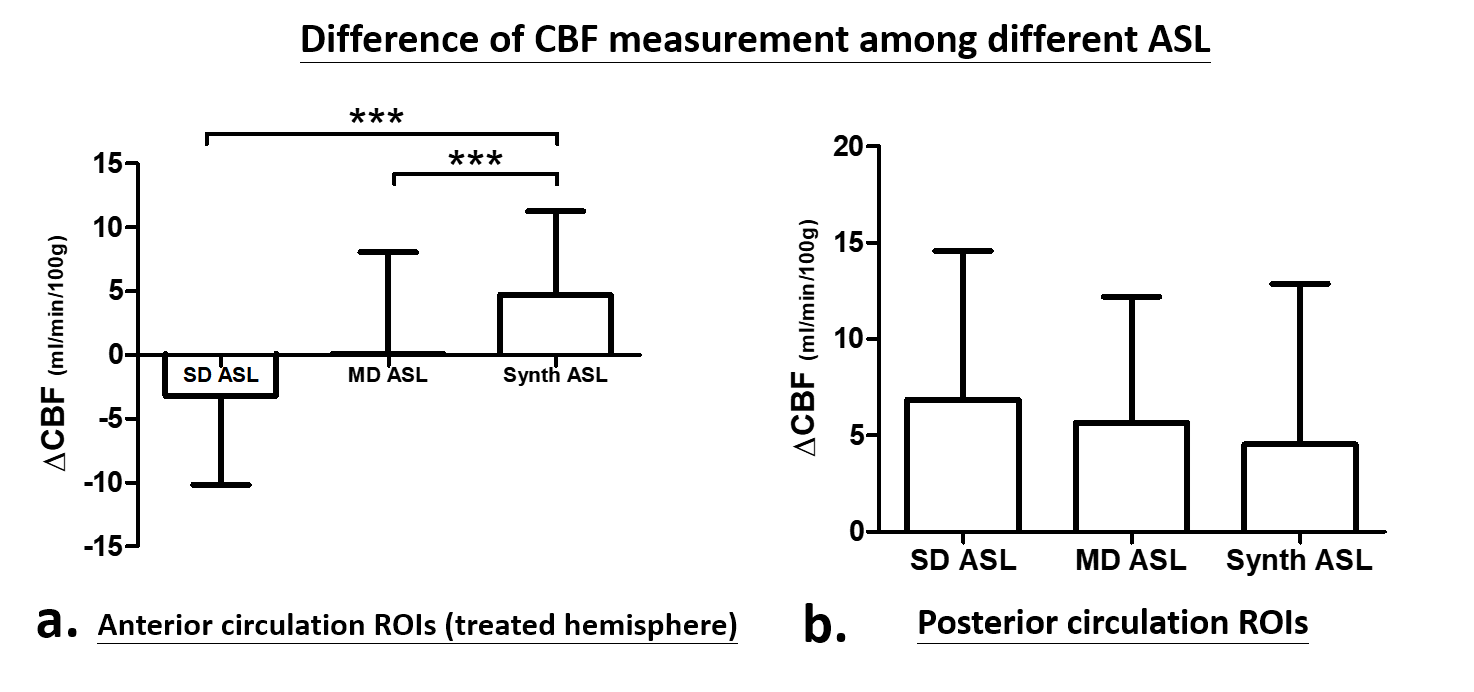
Longitudinal perfusion images of two Moyamoya patients are shown in Figure 1. Local artifacts of hypo- and hyper-perfusion, especially in regions with prolonged ATT, were visualized in SD-ASL and MD-ASL, but were less prominent in Synth-ASL images. In group average CBF difference maps (Figure 2), SD-ASL and MD-ASL demonstrated noisy, heterogeneous change of CBF after surgery, while Synth-ASL revealed a more homogenous increase of CBF. Across the ASPECTS ROIs, Synth-ASL measured a significant increase of CBF after surgery (before/after 39.38/45.11 mL/mins/100g, p-value <0.00001), whereas SD-ASL and MD-ASL did not show a significant change in CBF (SD, 39.73/39.99, p-value 0.799; MD, 39.59/41.17, p-value 0.098) (Figure 3). In the anterior circulation of treated hemispheres, synth-ASL showed a significant increase of CBF after surgery (p-value < 0.0001), whereas SD-ASL showed significant decrease of CBF (p-value 0.0017) and MD-ASL showed no significant change (p-value 0.461). In the posterior circulation, all three ASL show significant CBF increase after surgery (p-value 0.0459, 0.0035, 0.0029 for SD-, MD-, synth-ASL respectively) (Figure 4). Synth-ASL measured significantly greater CBF change due to surgery compared to SD-ASL and MD-ASL in the anterior circulation of treated hemisphere. Measured CBF change in the posterior circulation was not different between SD-, MD- and Synth-ASL (Figure 5).
Conclusion:
In longitudinal CBF follow-up before and after bypass surgery in Moyamoya disease, Synth-ASL showed greater CBF increase due to treatment compared to SD-ASL and MD-ASL. CBF difference maps from Synth-ASL were also more homogeneous than SD-ASL and MD-ASL, likely reflecting a reduction of CBF bias in areas with long ATT and reduction of noise by the deep learning network. Synth-ASL may serve as a robust technique for CBF follow-up in cerebrovascular patients.Acknowledgements
No acknowledgement found.References
1. Audrey P. Fan, Jia Guo, Mohammad M. Khalighi et al. Long-Delay Arterial Spin Labeling Provides More Accurate Cerebral Blood Flow Measurements in Moyamoya Patients A Simultaneous Positron Emission Tomography/MRI Study. Stroke. 2017;48(9):2441-2449
2. Guo J, Gong E, Goubran M, Fan AP, Khalighi M, Zaharchuk G. Improving Perfusion Image Quality and Quantification Accuracy Using Multi-contrast MRI and Deep Convolutional Neural Networks. 26th annual meeting of the Int Soc Magn Reson Med, Paris France: 310 (2017).
3. Alsop DC, Detre JA, Golay X, et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med. 2015;73(1):102-16.
4. Buxton RB, Frank LR, Wong EC, Siewert B, Warach S, Edelman RR. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med. 1998;40:383-96.
5. Kim JJ, Fischbein NJ, Lu Y, Pham D, Dillon WP. Regional angiographic grading system for collateral flow: correlation with cerebral infarction in patients with middle cerebral artery occlusion. Stroke. 2004;35:1340–1344.
Figures