2637
Assessment of inter-fractional positional accuracy of anterior visual pathway in a frameless stereotactic radiosurgery using an MR-simulator1Medical Physics and Research Department, Hong Kong Sanatorium & Hospital, Happy Valley, Hong Kong, 2Department of radiotherapy, Hong Kong Sanatorium & Hospital, Happy Valley, Hong Kong
Synopsis
In hypofractionized stereotactic radiosurgery (SRS), radiation-induced optic neuropathy (RION) might associate with the local radiation injury to anterior visual pathway (AVP), while the irradiated dose to AVP is much influenced by its positional variation. We for the first time assessed the inter-fractional AVP positional variation in a hypofractionized frameless SRS setting on 13 volunteers using a 1.5T MR-simulator. The results suggested that sub-millimeter AVP positional accuracy could be achieved in the frameless SRS after brain alignment. However, the dose uncertainty in the most anterior optical nerves should be concerned (1.2±2.6 mm positional variability) in a sharp dose gradient of SRS.
INTRODUCTION
Radiation-induced optic neuropathy (RION) is a late complication of radiotherapy (RT) to the anterior visual pathway (AVP) resulting in acute, profound, irreversible visual loss (1). Previous data obtained in conventional fractionized and single-fraction RT strongly indicates that total dose and fraction size are the two most important RT-related risk factors (2). However, for hypofractionized stereotactic radiosurgery (SRS) associated with high dose per fraction and steep dose gradient, the radiation injury might occur just locally rather than globally in the AVP, and the radiation dose delivered to the part of the AVP could also be much influenced by the inter-fractional AVP positional variation, but this has not been validated by any prospective imaging study so far. We hypothesized that the inter-fractional position variation of the AVP could be revealed and quantitatively assessed by using an MR-simulator on which the patient could be scanned in the identical position as in the real SRS treatment. As such, we attempted to investigate the inter-fractional positional accuracy of AVP in a frameless SRS scheme on a cohort of healthy volunteers using a 1.5T RT-dedicated MR-simulator.METHODS
Thirteen healthy volunteers each received 4-6 MRI scans to simulate the hypofractionized SRS treatment on a 1.5T MR-simulator in a frameless SRS treatment position immobilized with a thermoplastic mask. All subjects were each time aligned with a 3D external laser to minimize positional variability. A 3D-T1w-SPACE sequence enabling 3D geometric distortion correction (TE/TR=7.2/420ms, turbo factor=40, isotropic-voxel-size=1.05mm, GRAPPA factor=3, bandwidth=657Hz/pixel, acquisition time=5min) was used.
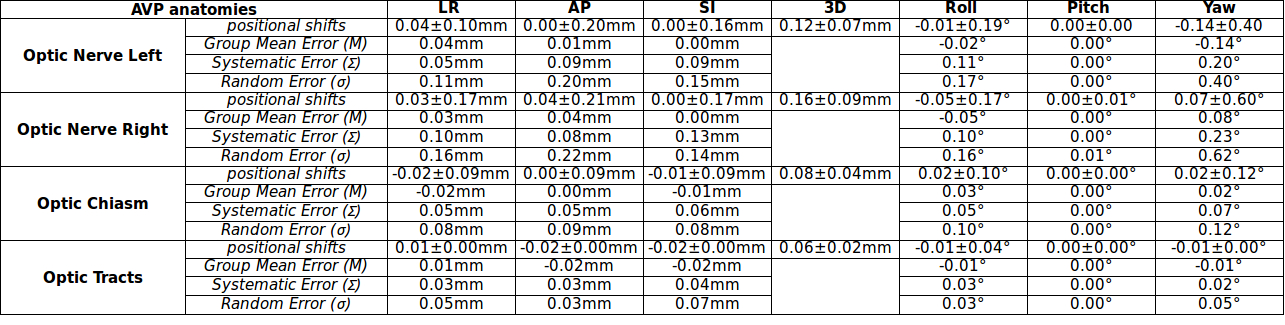
First scan MR images were used as reference. Firstly, brain in the subsequent scan MR images was rigidly registered to the reference. This brain pre-registration was used to mimic the X-ray imaging based patient positioning verification and correction prior to each SRS treatment in practice. Then, the brain pre-registered image series were again rigidly registered to the reference focusing on four individual anatomies of left optic nerve (ONL), right optic nerve (ONR), optic chiasm (CH) and optic tract (OT) manually delineated from the reference. Transformation matrics for each anatomy were used to calculate the residual positional shift relative to the reference. Group mean error (M), systematic error (Σ) and random error (σ) were quantified. Positional variation differences between anatomies were compared using signed-rank test. Positional variation correlations between anatomies were assessed using Pearson correlation coefficient r. As the anterior optic nerves subjected to high deformability in their motion, the central line position of the optic nerve anterior end connecting to the eyeball was also calculated on optic nerve registered images.
RESULTS
The inter-fractional residual positional variation of AVP in a subject after brain alignment was animated (Fig. 1). The residual positional variations of the four AVP anatomies relative to the reference were summarized (Table 1), smallest in OC and largest in ONR (Fig. 2), with significant difference (p<0.05). All four anatomies exhibited insignificant correlations on their residual positional variations (r: ranged from -0.03 to 0.43; p>0.05). The systematic error and random error of all anatomies were smaller than 0.22 mm and 0.62o, indicating the high positional accuracy achieved in the frameless SRS. However, even after this rigorous alignment, it was observed that the most anterior optical nerves could still have the positional variability in 3D up to 1.2±2.6 mm.DISCUSSION
With the high radiation dose and uniformly sharp gradients used in SRS, even the small positional uncertainty in the AVP could result in considerable irradiated dose volume to a certain part in the AVP. In contrast to the well acknowledged dose and fraction size effects on RION, the imaging study to investigate position and volume effect on RION is still sparse. By taking the advantages of non-ionizing imaging nature, superior soft tissue contrast, high isotropic resolution, and precise identical treatment position setup of a 1.5T MR-sim, the inter-fractional AVP positional variability was for the first time prospectively revealed and assessed in this study. This study would be helpful in SRS treatment planning to account for dose volume effect on AVP so as to better spare AVP and thus hopefully reduce RION incidence. This study also has limitations. Only Healthy volunteers were recruited and the sample size was small. Dose effect resulted from AVP positional uncertainty could not be assessed in its study design either.CONCLUSION
We for the first time quantitatively assessed the inter-fractional positional variation of the AVP in a hypofractionized frameless SRS setting using a 1.5T MR-simulator. The results suggested that very small residual positional error and high positional accuracy of AVP could be achieved in the frameless SRS. However, the dose uncertainty delivered to the most anterior optical nerves should still be concerned due to their large positional variability in the presence of sharp dose gradient.Acknowledgements
No acknowledgement found.References
1. Danesh-Meyer HV. Radiation-induced optic neuropathy. J Clin Neurosci 2008;15(2):95-100.
2. Mayo C, Martel MK, Marks LB, Flickinger J, Nam J, Kirkpatrick J. Radiation dose-volume effects of optic nerves and chiasm. Int J Radiat Oncol Biol Phys 2010;76(3 Suppl):S28-35.
Figures