2625
Automated MP2RAGE-based Brain Volumetry for Pediatric Patients: A Clinical Usability Study1Pediatric Radiology, CHRU of Tours, Tours, France, 2Advanced Clinical Imaging Technology, Siemens Healthineers, Lausanne, Switzerland, 3Radiology, Lausanne University Hospital, Lausanne, Switzerland, 4Pediatric Radiology, CHRU of Tours, Tours, Switzerland, 5Neuroradiology, CHRU of Tours, Tours, France
Synopsis
Antenatal and mostly post-natal periods are crucial for brain development, characterized by volume increase, brain maturation, neuronal proliferation, neural migration, and myelination. Head circumference is a reliable clinical assessment of brain volume, correlated with neurodevelopmental outcomes (psychomotor and cognitive development). Particularly in young children, it is a fast and inexpensive tool for brain growth follow-up. Complementarily, brain MRI is becoming more frequently used as a first-line examination for suspected brain development abnormality. In this work, we evaluate the potential of an automated MP2RAGE-based brain volumetry method to objectively support radiologists to better assess brain physiological and pathological cerebral growth.
Introduction
Cerebral MRI is becoming of routine diagnostic utility for evaluating atypical brain developments. Cerebral volume abnormalities are usually clinically assessed by measuring the head circumference (HC) (1-8), but some forms can have a more subclinical presentation, for example in case of low birth body weight and dolichocephaly in premature newborns (9). Moreover, HC is nonspecific; its variations can be related to volume changes of brain parenchyma, extra- and intra-ventricular spaces, intra-cranial blood pool and skull thickness. Although HC is correlated with Total Intra-cranial Volume (TIV) (6), it does not reflect the proportion and variation of cerebro-spinal fluid (CSF), gray matter (GM), and white matter (WM). Subnormal HC in low-birth-weight infants was associated with poor cognitive function (10). The aim of the study was to evaluate whether brain size abnormality can be reliably diagnosed based on automated structural MRI analyses. To this end, we evaluated the inter-rater radiologist diagnostic reliability for the MRI diagnosis of different subtypes of pathologies, including size abnormality, against a fully automated segmentation tool.Materials and Methods
All child’s parents gave informed consent. We performed a monocentric prospective study including 44 patients from 6 months to 5 years (24 males, 20 females). Clinical head circumferences were obtained from medical reports. HC z-scores were then computed with respect to the World Health Organization (WHO) data. All patients were scanned at 1.5T (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) using the MP2RAGE sequence (TI1/TI2=600/2000 ms, TR=5000 ms, TE=2.77 ms voxel size=1.3x1.3x1.3mm3, TA=6:42 min) with a 20-channel coil. All resulting images were blindly reviewed by one junior and two senior pediatric radiologists. Each subject was classified into the following categories: normal MRI or tumor, inflammation, malformation, vascular, head size abnormalities, perinatal injuries sequela, and traumatic pathology. Total intracranial volume, brain parenchyma, CSF volumes were automatically estimated using the MorphoBox prototype (11) which takes both the second inversion contrast and the uniform original MP2RAGE contrast as inputs (12). Statistical analyses were performed using the software R version 3.3.1 (13). Inter-observer agreements on the interpretation of the brain MRI were assessed using Fleiss’ kappa coefficient. A Pearson correlation coefficient was calculated between total intracranial and brain volumes with head circumference.
Results
Twenty-four-brain MRI were classified as normal and 20 as pathologic, including 8 brain volume abnormalities, 7 perinatal injury sequela, 4 malformations, and one traumatic hematoma (Figure 1). According to the clinical HC, the seniors radiologists gave 13/44 and 16/44 wrong brain size interpretations, the junior radiologist 13/44. Concerning other pathological conditions, inter-observer kappa coefficients were of 0.93 between junior and seniors and between seniors. Total intracranial volume and brain volumes were significantly correlated with head circumference (Figure 2, p<0.0001). Total intracranial volume, brain parenchyma, and CSF volumes are provided in Figure 3. CSF volumes appeared to be relatively constant during childhood. Brain parenchyma volumes have a regular increase.Conclusion
While radiologists performed well with fairly good consistency in interpreting brain MRI, this study shows that an automated brain segmentation would be more suitable to describe and follow-up growth delay and brain size abnormalities in an objective manner. It could also assist radiologists determining which brain structures have a pathological development, hence avoiding incorrect interpretations. This would require establishing normative ranges, which requires further research.Acknowledgements
No acknowledgement found.References
1. Gale CR, O’Callaghan FJ, Godfrey KM, Law CM, Martyn CN. Critical periods of brain growth and cognitive function in children. Brain J. Neurol. 2004;127:321–329 doi: 10.1093/brain/awh034. 2. Ehrenkranz RA, Dusick AM, Vohr BR, Wright LL, Wrage LA, Poole WK. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics 2006;117:1253–1261 doi: 10.1542/peds.2005-1368. 3. Leppänen M, Lapinleimu H, Lind A, et al. Antenatal and postnatal growth and 5-year cognitive outcome in very preterm infants. Pediatrics 2014;133:63–70 doi: 10.1542/peds.2013-1187. 4. Ghods E, Kreissl A, Brandstetter S, Fuiko R, Widhalm K. Head circumference catch-up growth among preterm very low birth weight infants: effect on neurodevelopmental outcome. J. Perinat. Med. 2011;39:579–586 doi: 10.1515/JPM.2011.049. 5. Sicard M, Nusinovici S, Hanf M, et al. Fetal and Postnatal Head Circumference Growth: Synergetic Factors for Neurodevelopmental Outcome at 2 Years of Age for Preterm Infants. Neonatology 2017;112:122–129 doi: 10.1159/000464272. 6. Cooke RW, Lucas A, Yudkin PL, Pryse-Davies J. Head circumference as an index of brain weight in the fetus and newborn. Early Hum. Dev. 1977;1:145–149. 7. Lindley AA, Benson JE, Grimes C, Cole TM, Herman AA. The relationship in neonates between clinically measured head circumference and brain volume estimated from head CT-scans. Early Hum. Dev. 1999;56:17–29 doi: 10.1016/S0378-3782(99)00033-X. 8. Bartholomeusz HH, Courchesne E, Karns CM. Relationship Between Head Circumference and Brain Volume in Healthy Normal Toddlers, Children, and Adults. Neuropediatrics 2002;33:239–241 doi: 10.1055/s-2002-36735. 9. Kawasaki Y, Yoshida T, Matsui M, et al. Clinical Factors That Affect the Relationship between Head Circumference and Brain Volume in Very-Low-Birth-Weight Infants. J. Neuroimaging Off. J. Am. Soc. Neuroimaging 2018 doi: 10.1111/jon.12558. 10. Hack M, Breslau N, Weissman B, Aram D, Klein N, Borawski E. Effect of very low birth weight and subnormal head size on cognitive abilities at school age. N. Engl. J. Med. 1991;325:231–237 doi: 10.1056/NEJM199107253250403. 11. Schmitter D, Roche A, Maréchal B, et al. An evaluation of volume-based morphometry for prediction of mild cognitive impairment and Alzheimer’s disease. NeuroImage Clin. 2015;7:7–17 doi: 10.1016/j.nicl.2014.11.001. 12. Boto J, Gkinis G, Roche A, et al. Evaluating anorexia-related brain atrophy using MP2RAGE-based morphometry. Eur. Radiol. 2017;27:5064–5072 doi: 10.1007/s00330-017-4914-9. 13. Team RC. R: A language and environment for statistical computing. Vienna, Austria;Figures
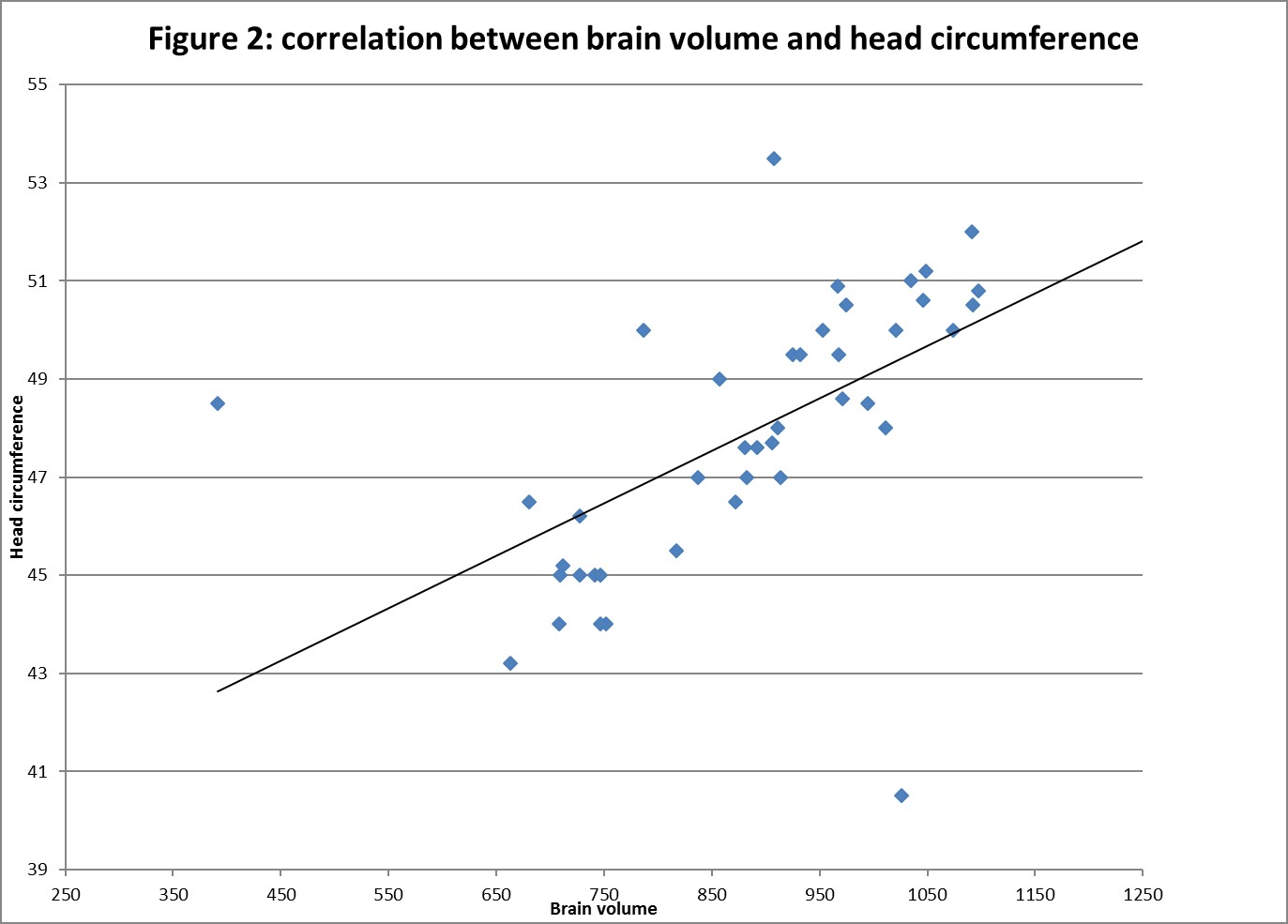
Figure 2
Correlation between automatically estimated brain volume (ml) and head circumference (cm)
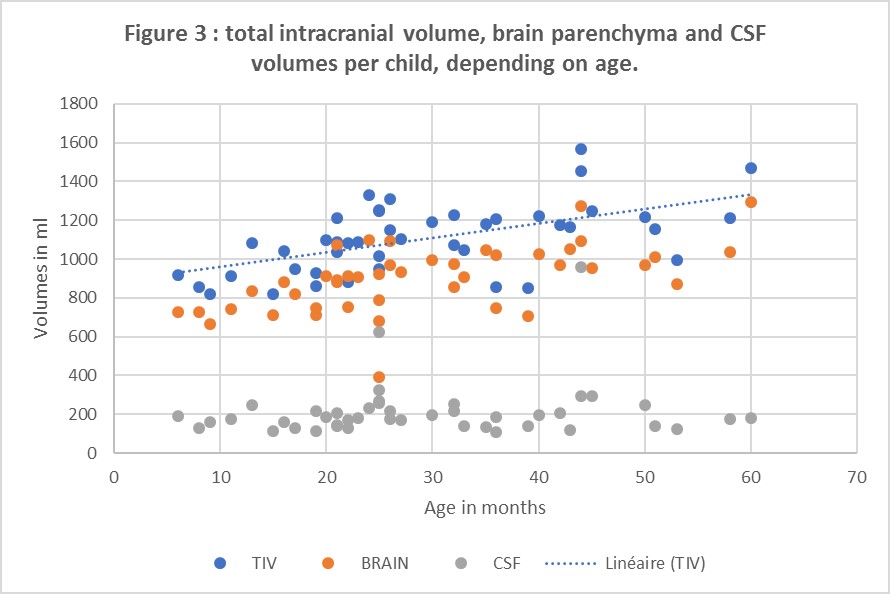
Figure3
Scatter graph showing TIV and brain parenchyma volumes (ml) according to ages (months).
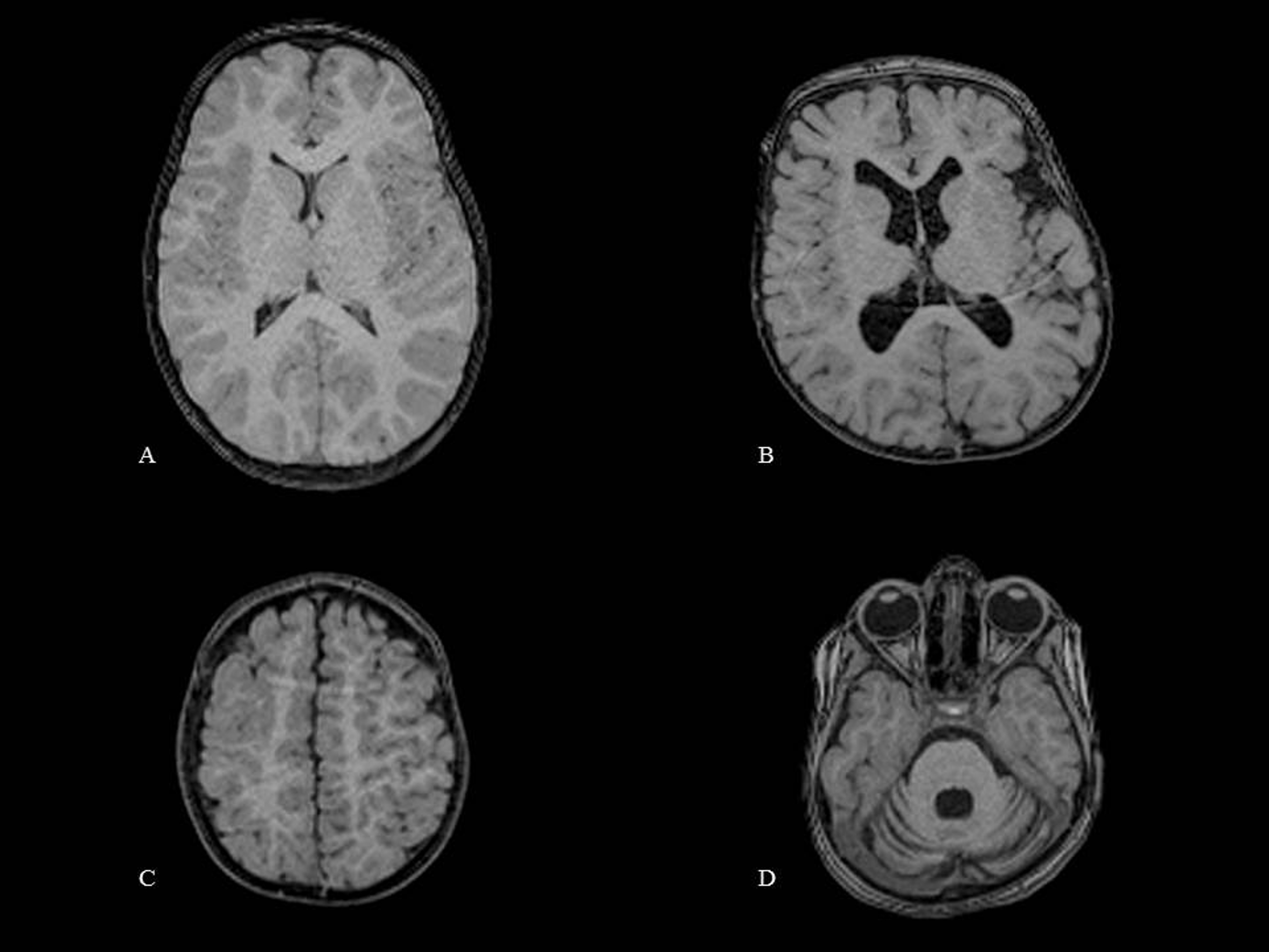
Figure 1
Exemplary MPR axial INV2 images from 3D MP2RAGE sequence.
A. Normal brain image from a 3-years-and-7-month-old boy.
B. Ventricular dilatation image from a 2-year-and-1-month-old girl.
C. Polymicrogyria in a 1-year-and-5-month-old boy
D. Hemispheric cerebellar atrophy in a 3-year-and-3-month-old girl.