2616
The change of cerebral cortex in children with Tourette syndrome1Beijing Children's Hospital, Beijing, China, 2China Academy of Information and Communications Technology, Beijing, China
Synopsis
Tourette syndrome (TS) is a developmental neuropsychiatric disorder and is characterized by multiple motor and vocal tics. To understand the developmental cause of such changes, we investigated microstructural changes of cortical thickness , cortical sulcus, cortical curvature, and LGI in TS children by using sagittal three-dimensional T1-weighted image (3DT1WI) Magnetization. The TS children had the significant differences in cortical thickness, cortical sulcus, cortical curvature, and LGI compared with controls.
Introduction
Tourette syndrome (TS) is a common, chronic neuropsychiatric disorder characterized by the presence of multiple motor and vocal tics[1]. Besides tics ,TS is frequently concomitant with obsessive-compulsive disorder(OCD), attention-deficit-hyperactivity disorder (ADHD) and other social and behavioral disturbances .To further understand the pathogenesis of TS, and promote the early diagnosis, improve the treatment effect,we use magnetic resonance imaging detected the change of cortical thickness in groups of Tourette syndrome relative to controls .Methods
60 children with TS(age 8.79 ± 3.07 years, range 3–16 years; 11 female) and 52 age and gender matched health controls (age 10.82±3.36 years, range 3–16 years; 18 female)were scanned by 3.0T MR scanner with three-dimensional T1-weighted image (3DT1WI). We then extracted some surface-based features by using FreeSurfer and performed the statistical analysis between two groups.Results
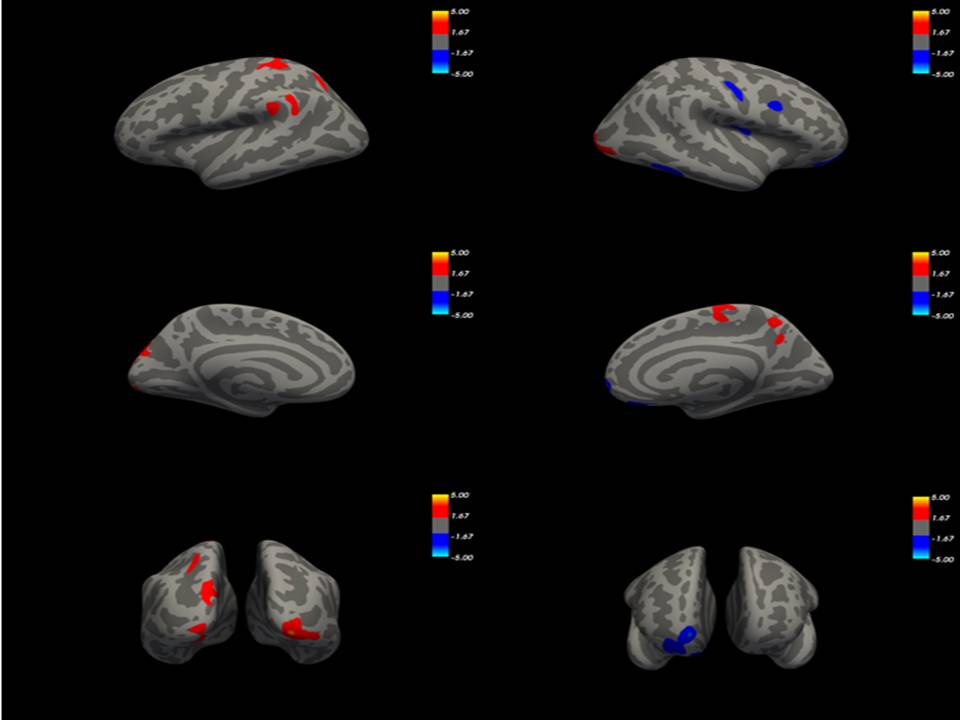
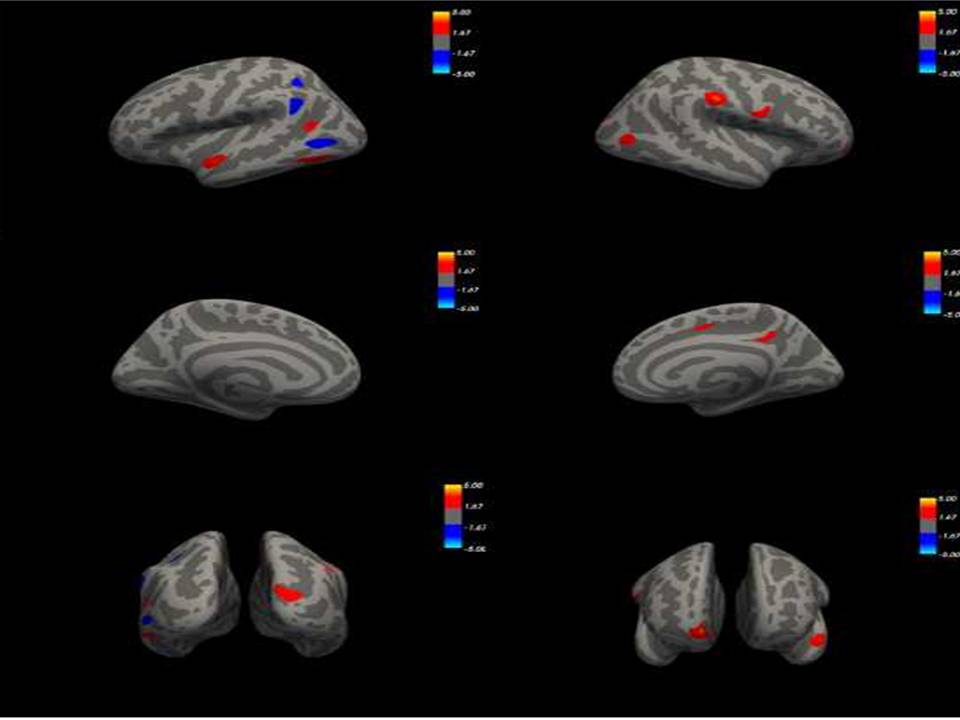
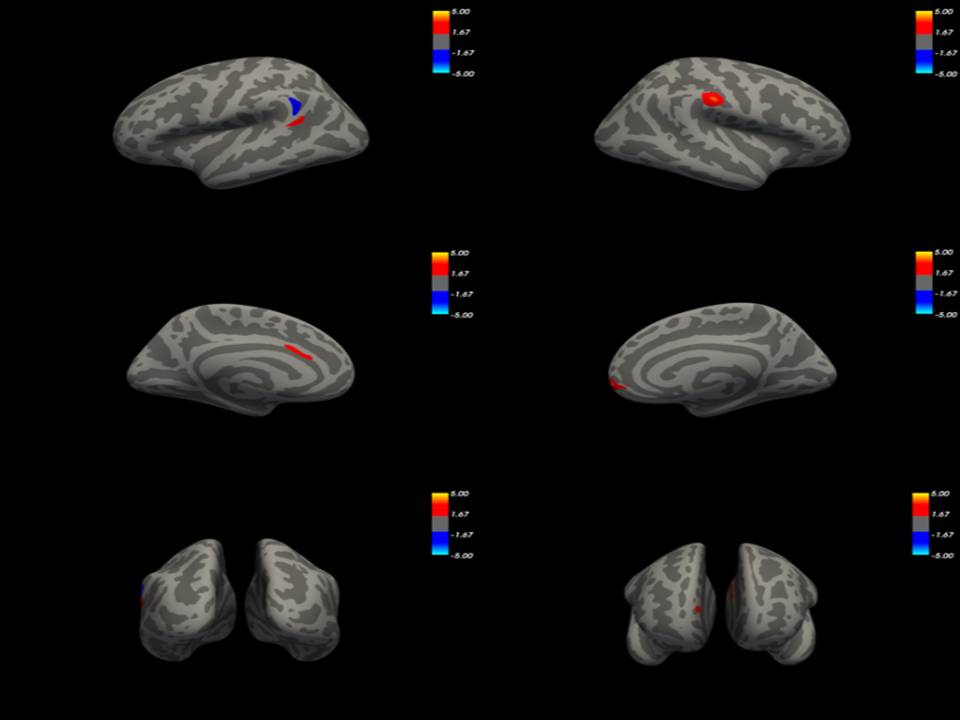
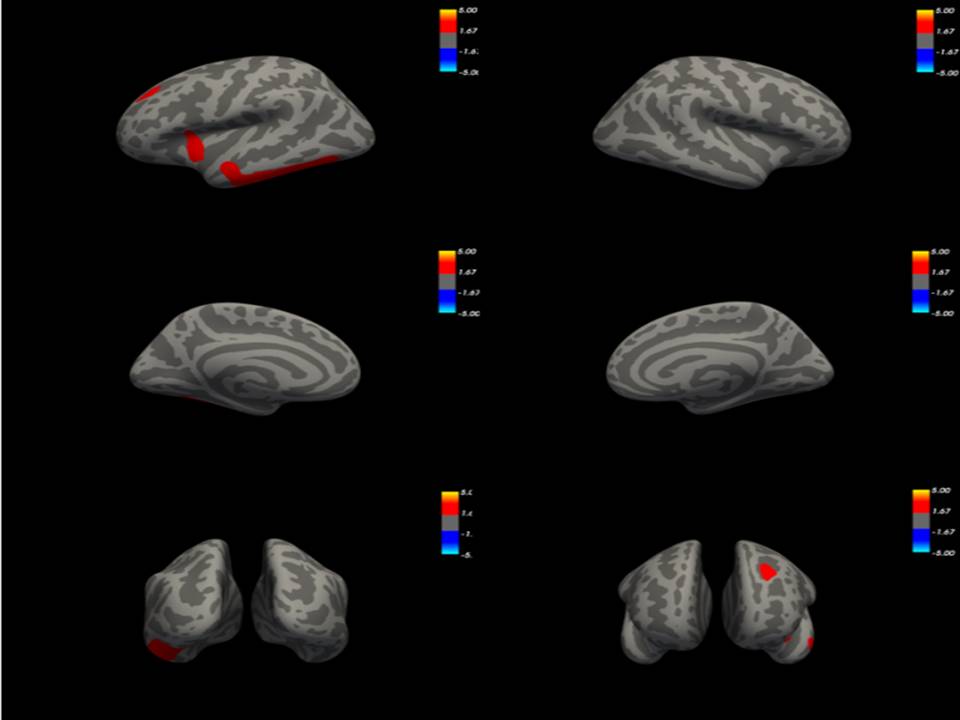
Surface analyses revealed altered cortical thickness, cortical sulcus, cortical curvature and LGI in TS compared to controls. The brain regions with significant differences in cortical thickness between TS patients and healthy subjects were postcentral,superiorparietal,rostralanteriorcingulate in left hemisphere and frontalpole, lateraloccipital, inferiortempora in right hemisphere(Figure 1).The cortical sulcus changed in superiortemporal, medialorbitofrontal, supramarginal, medialorbitofrontal, superiorparietal and lateraloccipital between TS and healthy subjects(Figure 2). The brain regions with significant differences in cortical curvature between TS patients and healthy subjects were caudalanteriorcingulate, supramarginal, inferiorparietal and lateraloccipital(Figure 3). The changes of LGI were most prominent in the inferortemporal and insula. Additionally,there was no statistical difference in brain surface area with controls(Figure 4).Discussion
Motor portions of CSTC circuits have long been postulated to be involved in the pathogenesis of Tourette syndrome[2]. Until now, the involvement of cortical portions of those circuits has not been widely suspected. In this study, We explain the structural correlates of the diversity of symptoms.Our study results prove that TS patients have abnormal changes in cortical structure. Combined with previous studies of basal ganglia[3,4] and thalamus[5] , we think that the nervous system develops rapidly in childhood, which may lead to the imperfect structure of CSTC circuit. Then the children show some tic. During adolescence, the physical growth and neurodevelopment of children is rapidly. The structure of CSTC circuit in some children may become perfect and the clinical symptoms will decrease. However, the structure of CSTC circuit in some children are still not perfect. The symptoms of this part of the TS children may continue into adulthood. Therefore, it is important to treat children before puberty.Acknowledgements
We thank Dr.Bin Lv for his time and suggestion that helped to enhance the quality of this article.References
[1]. Malaty, I.A. and U. Akbar, Updates in medical and surgical therapies for Tourette syndrome. Curr Neurol Neurosci Rep, 2014. 14(7): p. 458.
[2]. Albin, R.L. and J.W. Mink, Recent advances in Tourette syndrome research. Trends Neurosci, 2006. 29(3): p. 175-82.
[3]. Makki, M.I.,et al., Microstructural abnormalities of striatum and thalamus in children with Tourette syndrome. Mov Disord 2008.23:p2349-2356.
[4]. Worbe, Y.,et al., Distinct structural changes underpin clinical phenotypes in patients with Gilles de la Tourette syndrome. BRAIN 2010.133:p3649-3660.
[5]. Worbe, Y., et al., Altered structural connectivity of cortico-striato-pallido-thalamic networks in Gilles de la Tourette syndrome. BRAIN 2015. 138:p472-482.
Figures