2611
A Method for Evaluating Whole Brain Health of the Aging Brain: Assessment of Multiple MRI Detectable Brain Changes using the Brain Atrophy and Lesion Index (BALI)1Biomedical Physiology and Kinesiology, Simon Fraser University, Surrey, BC, Canada, 2Faculty of Applied Science, Simon Fraser University, Surrey, BC, Canada, 3ImageTech Laboratory, Surrey Memorial Hospital, Fraser Health Authority, Surrey, BC, Canada
Synopsis
As our population ages, there is a need for better methods of assessing neurodegeneration. However, current methods are based on a diagnostic model and assess changes in isolation, failing to account for the interconnected nature of the brain and the heterogeneity of the aging process. To address this, we introduced the Brain Atrophy and Lesion Index (BALI) an MRI based tool for the assessment of structural neurodegeneration across the whole brain. Here, we compare results from eight datasets to which BALI was applied (n=3295), and present a literature review to understand consensus regarding the brain changes assessed by the BALI.
Introduction
Degeneration in the aging brain is unavoidable1, yet there is currently no good method of quantifying and tracking structural degeneration across the entire brain as it ages2. To address this gap in the literature, we introduced the Brain Atrophy and Lesion Index (BALI) an MRI based semi-quantitative scale for the assessment of structural neurodegeneration across the whole brain.
While degeneration is ubiquitous in aging brains, the process manifests differently in each person, and the trajectory does not perfectly correspond with chronological age3. This introduces difficulties when attempting to track and quantify the aging process across individuals. Current methods are based on a diagnostic model, where a single element of neurodegeneration is quantified in attempt to connect it to a clinical outcome. However, this approach does not account for the heterogeneity of the degenerative process, and the interconnected nature of the brain4. In contrast, the BALI assesses a range of changes across the entire brain, allowing for a wholistic measure of the brain’s integrity.
Methods
To provide support for the validity of the BALI, we summarized and compared results from eight datasets to which the BALI was applied, and completed a review of literature detailing the prevalence, pathophysiological basis, and clinical connections of the MRI based changes the BALI considers. All data utilizing the BALI was downloaded and results were compiled, and a scoping review was completed to understand current consensus surrounding the brain changes assessed by the BALI.
When applying the BALI to the MR images in the datasets under study, manual raters used axial images to assess seven categories of changes in the brains, summing to a total score out of 25. Figure 1 gives a detailed breakdown of the categories. The BALI has been validated for use by trained non-neuroradiologist raters and can be applied in about 5 mins. Assessment using the BALI was done on a single structural MRI, and validated for use with several clinical available sequences (T1WI, T2WI, T2 FLAIR) at both 1.5T and 3T field strengths.
Results
Analysis from eight datasets revealed a large sample size (n=3,295). Across all datasets, both inter-rater (ICC’s 0.86-0.94) and intra-rater (ICC’s 0.85-0.94) was high, consistent for neuroradiologists and non-expert raters. Scores based on T1WI were correlated with scores from T2WI (r>0.93, P < .001), as well as 3T and 1.5T based scores (r < 0.93, P < .001).
BALI scores correlated with cognitive measures such as MMSE (r’s 0.42-0.52, p<.001), and ADAS-Cog (r’s 0.37-0.69, p<.001), as well as age (r’s 0.37-0.69, p<.001), education (K-W/χ2=6.65, p=0.036), physical activity levels (K-W/χ2 =12.20, p=0.002). The BALI scores were also strongly related to Alzheimers disease diagnostic status, differentiating these patients from those with mild cognitive impairment, and healthy controls (K-W/χ2 ‘s 19.6-156.03, p< .0001).
Additionally, our literature review found that the MRI visible brain changes considered by that BALI are prevalent, result from pathophysiology, and each are individually connected to negative clinical outcomes. Furthermore, research in the field indicates that when multiple changes are considered in unison, the ability of a scale to predict clinical outcomes is increased.
Discussion
The BALI is a new method of assessing neurodegeneration that better reflects the way in which the aging brain degenerates towards failure5. The brain can be considered a “complex system”, a type of system that functions and fails in a specific way. The high-level functions of the brain are emergent properties of the numerous subsystems that make up the brain, and each subsystem contains numerous redundancies, and the capacity for active self-repair6. Rather that high-level failure resulting from a single event, high level failure will generally result from overlapping elements of degeneration that overwhelm repair capabilities and redundancies7.
The multiple categories of the BALI better capture the inherent heterogeneity of the degenerative process, and will thus allow us to better study and track patients as they age. The scale is reliable and easy to employ, with strong correlations to cognitive measurements and diagnostic categories. Its categories are also supported by literature on the underlying pathophysiological processes at play.
Conclusions
Overall, this work supports the assertion that the BALI is a valid scale for the quantification of age-related structural neurodegeneration. Having a scale capable of tracking the aging brains degeneration will allow us to better study the aging process, and will allow for the identification of patients at risk. Future work aims to automate the BALI for ease of application in clinical environments, and when using larger datasets.Acknowledgements
We gratefully acknowledge Canadas National Science and Engineering Research Council (NSERC) for providing funding to L. Grajauskas; the China Scholarship Council for providing funding for H. Guo to conduct research in Canada; and the Canadian Institutes of Health Research (#CSE-125739) and Surrey Hospital and Outpatient Centre Foundation (#FHREB2015-030) for providing operating grants to X. Song.References
1. Chowdhury, M. H., Nagai, A., Bokura, H., Nakamura, E., Kobayashi, S., & Yamaguchi, S. (2011). Age-Related Changes in White Matter Lesions, Hippocampal Atrophy, and Cerebral Microbleeds in Healthy Subjects Without Major Cerebrovascular Risk Factors. Journal of Stroke and Cerebrovascular Diseases, 20, 302–309. https://doi.org/10.1016/j.jstrokecerebrovasdis.2009.12.010
2. Grajauskas, L. A., Guo, H., D’Arcy, R. C. N., & Song, X. (2018). Toward MRI‐based whole‐brain health assessment: The brain atrophy and lesion index (BALI). Aging Medicine, 1(1), 55–63.
3. Mitnitski, A., Song, X., & Rockwood, K. (2013). Assessing biological aging: The origin of deficit accumulation. Biogerontology, 14(6), 709–717. https://doi.org/10.1007/s10522-013-9446-3
4. Guo, H., Siu, W., D’Arcy, R. C., Black, S. E. S. E., Grajauskas, L. A. L. A., Singh, S., … Song, X. (2017). MRI assessment of whole-brain structural changes in aging. Clinical Interventions in Aging, 12, 1251–1270. https://doi.org/10.2147/CIA.S139515\
5. Guo, H., Song, X., Schmidt, M. H., Vandorpe, R., Yang, Z., LeBlanc, E., … Rockwood, K. (2014). Evaluation of whole brain health in aging and Alzheimer’s disease: A standard procedure for scoring an MRI-based brain atrophy and lesion index. Journal of Alzheimer’s Disease. https://doi.org/10.3233/JAD-140333
6. Cook, R. I. (2000). How Complex Systems Fail. Cognitive Technologies Laboratory; University of Chicago, 1–5. Retrieved from http://web.mit.edu/2.75/resources/random/How Complex Systems Fail.pdf
7. Mitnitski, A. B., Rutenberg, A. D., Farrell, S., & Rockwood, K. (2017). Aging, frailty and complex networks. Biogerontology, 1–14. https://doi.org/10.1007/s10522-017-9684-x
Figures
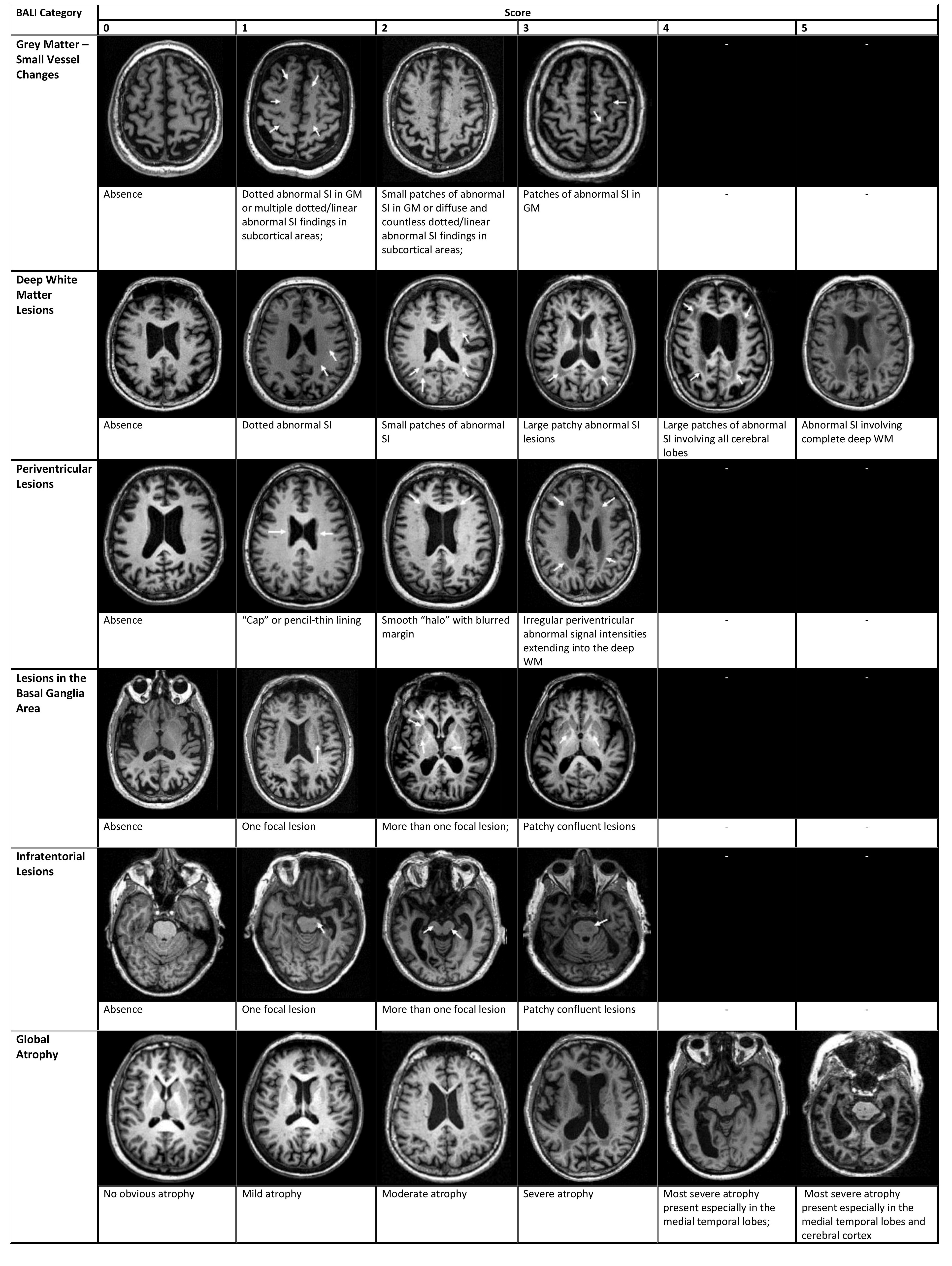
Figure 1. Assessment of Age-Related Brain Changes using the BALI on T1 MRI
A rater manually assesses the seven BALI categories on axial slices. Category seven is "other findings", which notes the presence of other changes such as malacia or hydrocephalus. This is then summed to a total score out of 25.
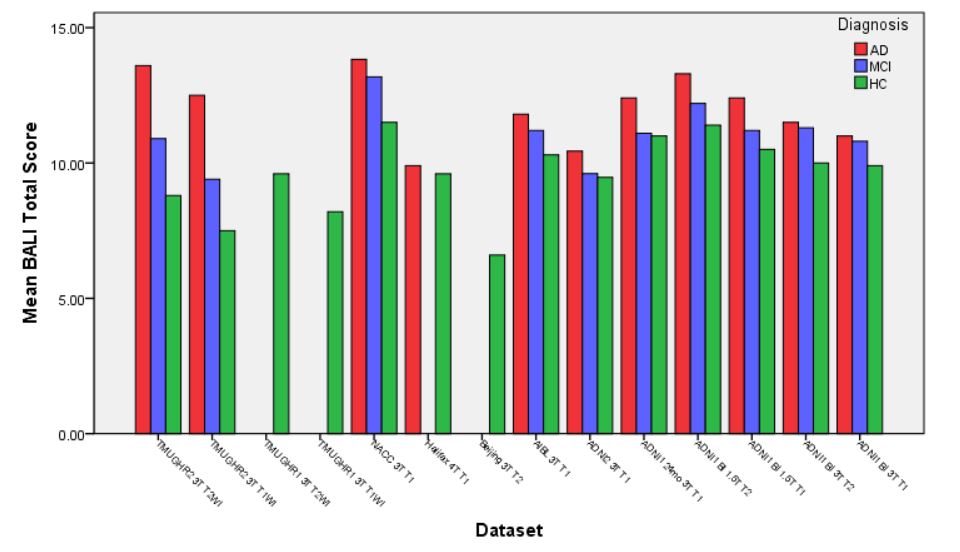
Figure 2. Mean BALI Score for Diagnostic Categories in Studied Datasets
Acronyms: AD = Alzheimers Disease, ADNI1 = Alzheimer's Disease Neuroimaging Initiative Phase 1, ADNI2 = Alzheimer's Disease Neuroimaging Initiative Phase 2, AIBL = Australian Imaging Biomarkers and Lifestyle Study of Ageing, HC = Healthy Controls, MCI = Mild Cognitive Impairment, T = Tesla, T1WI = T1 Weighted Image, T2WI = T2 Weighted Image, TMUGHR = Tianjin Medical University General Hospital Research.