2610
HIV alters brain activation during semantic memory processing demands1University of Warsaw, Warsaw, Poland, 2University of British Columbia, Vancouver, BC, Canada, 3Institute of Physiology and Pathology of Hearing, World Hearing Center, Kajetany, Nadarzyn, Poland, 4The Central Hospital for Infectious Diseases, Warsaw, Poland, 5Medical University of Warsaw, Warsaw, Poland, 6The Institute of Psychiatry and Neurology, Warsaw, Poland, 7The Ohio State University, Columbus, OH, United States, 8The Cleveland Clinic, Cleveland, OH, United States
Synopsis
Memory and executive dysfunctions burden HIV patients even in the highly active antiretroviral treatment (HAART) era. The neurobiological correlates of these cognitive symptoms remain unclear limiting development of targeted treatment options. Functional magnetic resonance imaging (fMRI) is a promising route to estimate neural signature of HIV-related neurocognitive decline. We examined brain activity in HIV+/HAART+ vs. healthy individuals during execution of semantic memory task. Results show that famous names induce lower activation in left caudate, right thalamus and left middle occipital gyrus in HIV+ vs. healthy group, despite lack of behavioral differences. Such hypoactivation suggests brain functional reorganization in HIV+/HAART+ patients.
Introduction
The introduction of highly active antiretroviral therapy (HAART) in 1990s has diminished HIV-related neurocognitive deficits1. Currently, HIV typically involves degeneration in memory or executive functions1,2. Recent brain neuroimaging studies suggest neural grounds of slight cognitive decline revealed with standard tests3. The fMRI technique has proven sensitive to HIV-related brain functional connectivity changes, even before brain atrophy is present1. Here, we implemented semantic memory task-based fMRI sequences to examine brain activation in HIV+/HAART+ subjects vs. HIV- healthy volunteers.Methods
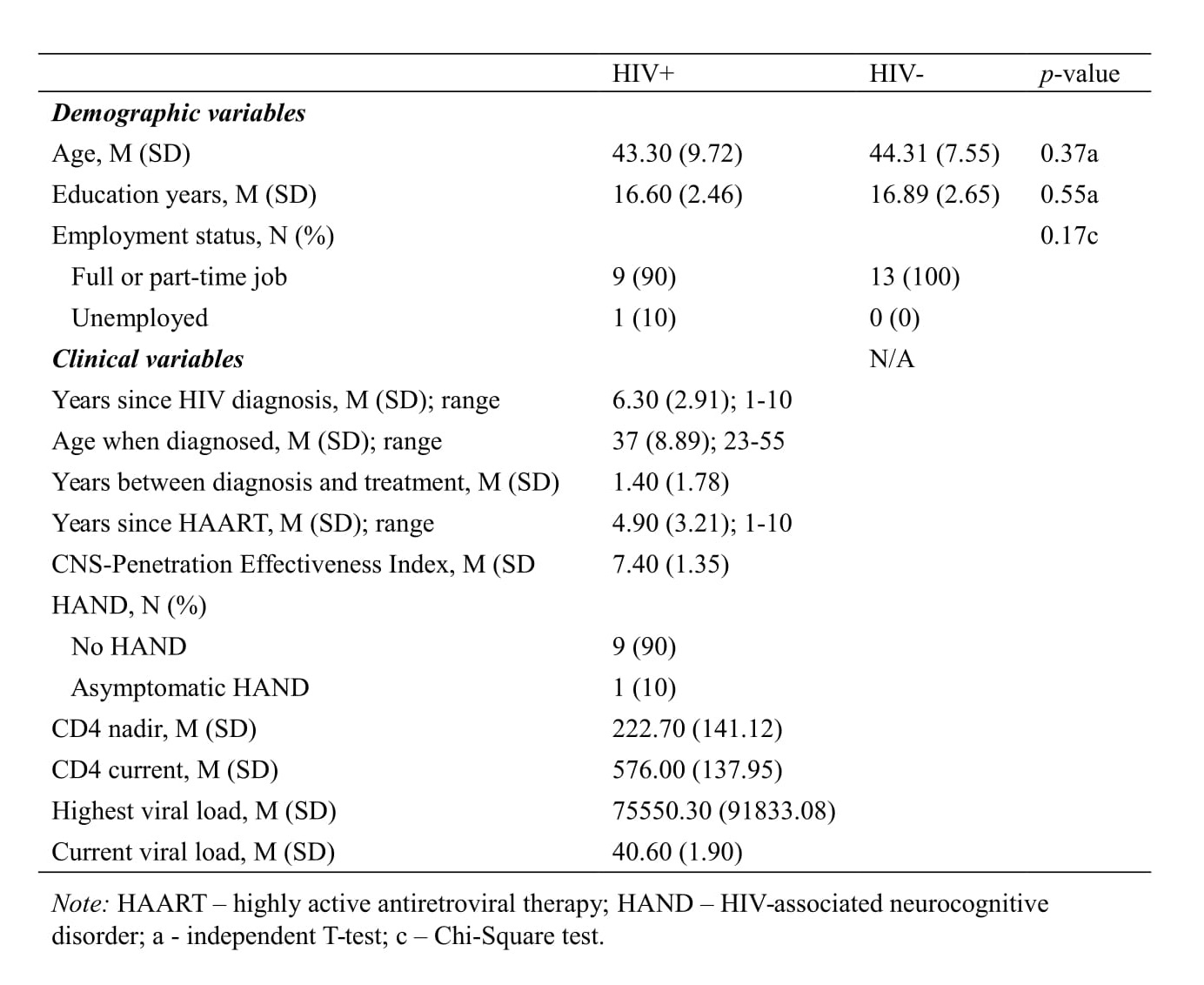
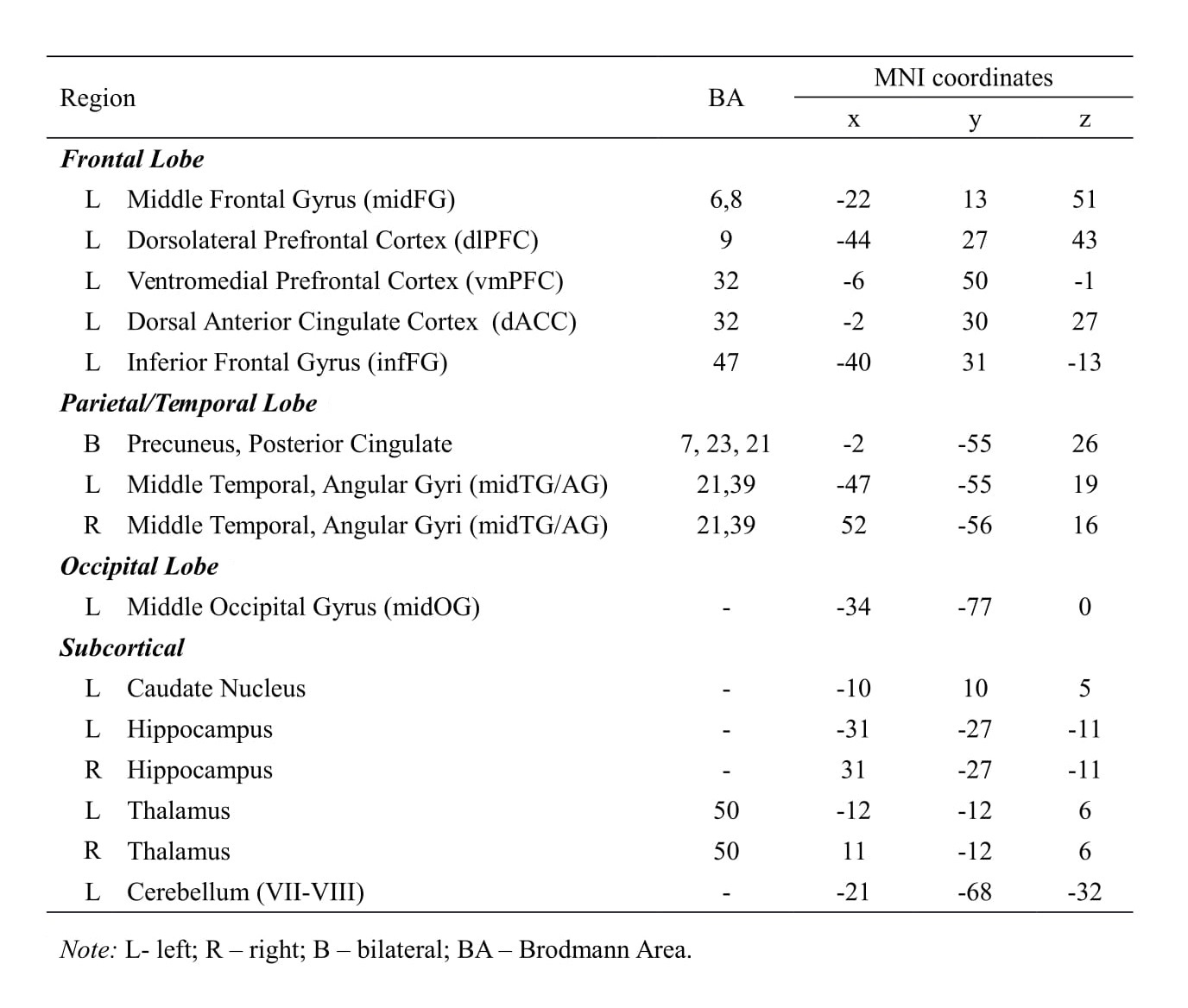
A total of 23 participants (HIV+/HAART+=10; HIV-=13; Mage= 44 years) took part in this study. Groups were matched on age, sex, health-related and socio-economic variables (Table 1). Assessment included comprehensive neuropsychological tests battery (i.e., verbal learning and memory, visual attention, fluency, set-shifting, numerical working memory, verbal fluency) and task-based fMRI conducted using 3T scanner with a 32-channel head coil. During fMRI sequences, subjects were asked to perform a low effort semantic memory task, i.e., the Famous Names Recognition Task4. The fMRI data analyses were executed with the SPM12 and related toolboxes5,6. Predefined 15 regions of interest (ROIs) due to previous literature7-9 (Table 2) were analyzed at voxel-level p<.001 (uncorrected) and at cluster-level p<.05 (FWE corrected).Results
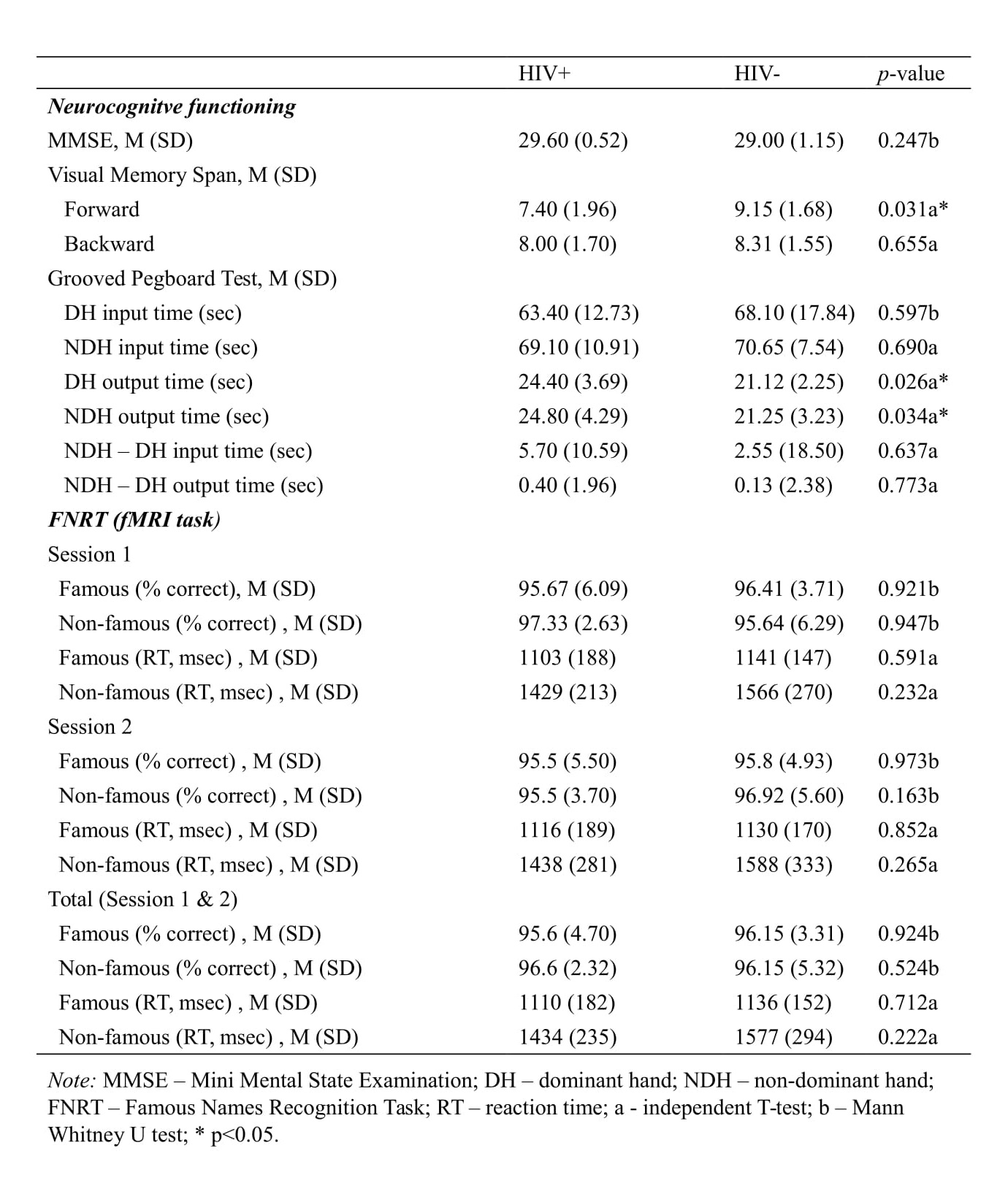
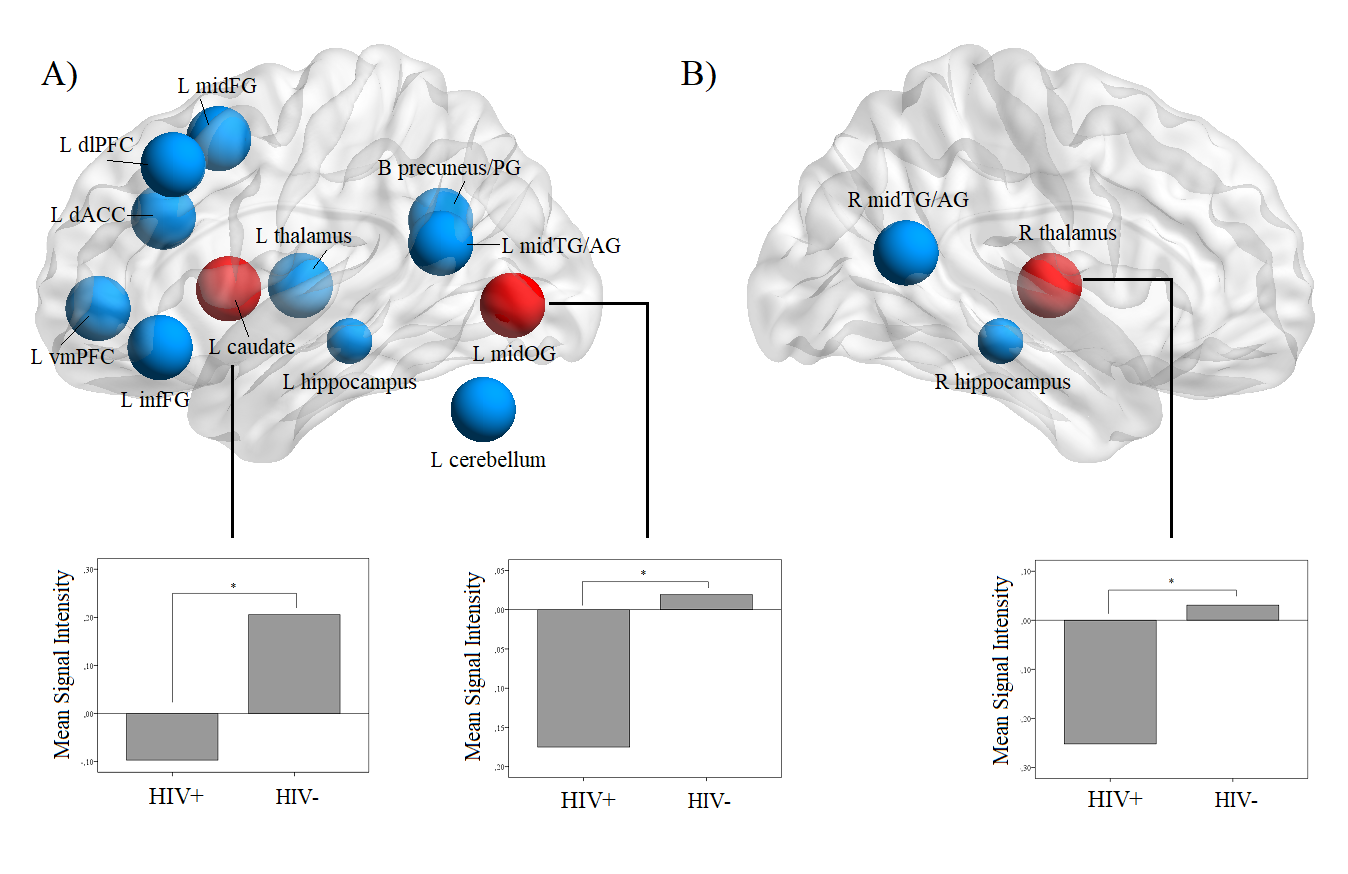
HIV+/HAART+ individuals revealed lower performance on visual memory span forward (t(21)=2.32, p=.031) and manual dexterity (t(21)=2.27, p=.034). No between-group differences were noted on FNRT reaction time or accuracy. (Table 3) The FNRT exhibited significant effects of HIV (corrected for age) in 3 ROIs (Figure 1). Brain activation F vs. NF contrast maps showed decreased brain activation in HIV+ group in left caudate (B=-0.302, p=0.039), right thalamus (B=-0.288, p=0.039), and left middle occipital gyrus (B=-0.192, p=0.048). HIV status alone explained 20% in the variability of fMRI signal change in these brain regions.Discussion
Even in the light of lack of observable neurocognitive decline in HIV+/HAART+ vs. healthy individuals, fMRI technique turned out to be sensitive to brain activity differences during execution of semantic memory task. We captured a pattern of brain regional hypoactivation due to semantic memory task while the performance outcomes were retained at an adequate level in HIV+/HAART+ patients. This finding is consistent with other research demonstrating functional brain abnormalities in HIV-positive subjects in the absence of cognitive decline3,10 and points to successful functional reorganization in asymptomatic HIV+/HAART+ patients. Furthermore, the depicted here brain regions belong to the fronto-striatal network (FSN), thus suggesting the significance of FSN reorganization in HIV infection. Our results are significant for articulating new hypotheses in future fMRI research in HIV infection.Conclusion
This study adds evidence for HIV-associated changes in task-related brain activation, particularly within the fronto-striatal network, that precede cognitive decline and brain atrophy.Acknowledgements
This study was supported by the Polish National Science Center (UMO-2012/06/M/H56/00316).References
- Heaton R, Franklin D, Ellis R, McCutchan J, Letendre S, LeBlanc S, et al. HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. J Neurovirol. 2010;17(1):3-16.
- Treisman G, Soudry O. Neuropsychiatric Effects of HIV Antiviral Medications. Drug Safety. 2016;39(10):945-957.
- Hakkers C, Arends J, Barth R, Du Plessis S, Hoepelman A, Vink M. Review of functional MRI in HIV: effects of aging and medication. J Neurovirol. 2016;23(1):20-32.
- Douville K, Woodard J, Seidenberg M, Miller S, Leveroni C, Nielson K et al. Medial temporal lobe activity for recognition of recent and remote famous names: an event-related fMRI study. Neuropsychologia. 2005;43(5):693-703.
- Statistical Parametric Mapping Version 12. Wellcome Department of Imaging Neuroscience London; 2014. http://www.fil.ion.ucl.ac.uk/spm/software/.
- Brett M, Anton J, Valabregue R, & Poline J. Region of interest analysis using the MarsBar toolbox for SPM 99. Neuroimage. 2002;16(2):S497.
- Woodard J, Seidenberg M, Nielson, Antuono P, Guidotti L, Durgerian S, Rao S, et al. Semantic memory activation in amnestic mild cognitive impairment. Brain. 2009;132(8):2068-2078.
- Rao S, Bonner-Jackson A, Nielson K, Seidenberg M, Smith J, Woodard J, Durgerian S. Genetic risk for Alzheimer's disease alters the five-year trajectory of semantic memory activation in cognitively intact elders. Neuroimage. 2015;111:136-146.
- Plessis S, Vink M, Joska J, Koutsilieri E, Stein D, Emsley R. HIV infection and the fronto–striatal system. AIDS. 2014;28(6):803-811
- Melrose R, Tinaz S, Castelo J, Courtney M, & Stern C. Compromised fronto-striatal functioning in HIV: An fMRI investigation of semantic event sequencing. Behav Brain Res. 2008;188(2):337-347.
Figures