2609
Thalamus in chronic low back pain: vertex-based morphometry and connectivity-based thalamic white-matter studiesHuiling Peng1, Jason Craggs2, Kelly Boland2, and Carmen Cirstea2
1Psychology, Temple University, Philadelphia, PA, United States, 2University of Missouri-Columbia, Columbia, MO, United States
Synopsis
Chronic low back pain (CLBP) is now considered a central nervous system disease. Thalamus is a key relay station for processing and transmission of nociceptive information to the cerebral cortex. We used vertex-based morphometry and connectivity-based diffusion tractography to test the hypothesis that the CLBP is associated with altered thalamic shape and altered white matter integrity of the thalamic projections to cortical regions in frontal and parietal lobes. Compare to controls, CLBP exhibited significant surface depression in left thalamus and lower fractional anisotropy in left thalamic projections to the posterior parietal cortex. This may represent a degenerative pain-related process.
Introduction:
Chronic low back pain (CLBP) is the leading cause of activity limitation and work absence in the U.S. No therapies are cited in CLBP as having persuasive evidence of improvement free of undesirable side-effects. This is a considerable issue for the U.S. healthcare system: total cost related to CLBP exceeds $100 billion per year. Despite the lack of clear pathology in CLBP, it is now considered a disease of the central nervous system (CNS) 1. Specifically, studies have suggested that thalamus is a key relay station for the processing and transmission of nociceptive information to the cerebral cortex. Thalamus also plays a key role of mediating different components of pain: sensory discriminative (lateral pain pathway) and affective-motivational (medial pain pathway) components 2-3. Decreased gray matter and white matter volume of certain brain regions, including thalamus has been reported, yet not present in all studies4-6. Likewise, it is not well understood whether the microstructural integrity of the thalamic projections to cortices involved in pain processing, e.g., somatosensory, cingulate, prelimbic, infralimbic, is altered. In this study, we used vertex-based morphometry and connectivity-based diffusion tensor tractography to test the hypothesis that the CLBP is associated with altered thalamic shape as well as altered white matter integrity, as measured via reduced fractional anisotropy (FA), of the thalamic projections to cortical regions in frontal and parietal lobes.Methods:
High-resolution T1-weighted MRI images were obtained in 45 CLBP and 57 age/sex-matched healthy controls. Vertex-based analysis (FIRST, FSL) was used to quantify the thalamic surface. The vertex locations from each subject are projected onto the surface normal of the average shape in MIN-152 space. The projection values representing the perpendicular distance from the average surface were stored in a 4D file and group analysis was performed using randomize (FSL) corrected for multiple comparisons to show localized shape differences. Among these subjects, 40 CLBP and 37 age/sex-matched healthy controls scanned using the same diffusion tensor imaging protocols were selected for connectivity-based thalamic white-matter analysis. FSL Oxford probabilistic atlas of sub-thalamic regions (Figure 1), segmented according to their white-matter connectivity to cortical areas (primary motor, sensory, pre-frontal, pre-motor, and posterior parietal cortex; connectivity probability > 50%), were used as group masks in MNI-152 space7-9. FA maps derived from all subjects’ DTI data were transformed into MNI-152 space using nonlinear registration. The mean FA of each of the 5 sub-thalamic regions was then calculated for all subjects and compared between CLBP and control groups using Mann-Whitney U test. Spearman correlation analysis was also performed to detect relationship between FA and the clinical score of pain measures (McGill pain questionnaire) in CLBP.Results:
As predicted, CLBP exhibited significant surface depression (p < 0.05, corrected for multiple comparisons using FDR) in dorsal and ventral regions of left thalamus compared to healthy controls (Figure 2). Likewise, the left thalamic projections to the posterior parietal cortex showed significant lower FA in CLBP vs. controls (0.37±0.03 vs. 0.39±0.04, p < 0.05), reflective of reduced axonal density, thickness, or demyelination. Contrary to our prediction, there were no significant changes in the right thalamus shape (Figure 3) or bilateral thalamic projections to regions in frontal cortex. No correlations between FA and pain measures were found in CLBP.Discussion:
Individuals with CLBP had distinct abnormalities in thalamic morphometry and thalamic projections to posterior parietal cortex compared to healthy controls. Previous studies showed that the posterior parietal cortex may play a role in conscious pain perception 10. Although the precise mechanisms underlying such changes remain unclear, an altered thalamus shape and altered white matter integrity may represent a degenerative pain-related process. Additional work is underway to decipher the functional implications of such changes.Acknowledgements
Supported by NIH Grant R01 NR015314-01A1 to Jason CraggsReferences
[1] Melzack R et al, J Dent Rduc. 2001; 65:1378-82. [2] Andersson JL et al, Exp Brain Res. 1997; 117(2):192–99. [3] Royce GJ et al, J Comp Neurol. 1985; 235(3):277–300. [4] Apkarian AV et al, J Neurosci. 2004; 24:10410-15. [5] Balike MN et al, PLoS One. 2011; 6:e26010. [6] Buckalew N et al, Pain med. 2008; 9:240-48. [6] Buckalew N et al, Pain Med. 2010; 11:1183-97. [7] Johansen-Berg H et al, Cerebral Cortex. 2005; 15(1):31-9. [8] Behrens TEJ et al, Nature Neuroscience. 2003; 6(7):750-757. [9] Behrens TEJ et al, MRM. 2003; 50:1077-1088. [10] Witting N et al, Neurology. 2001; 57(10):1817-24.Figures
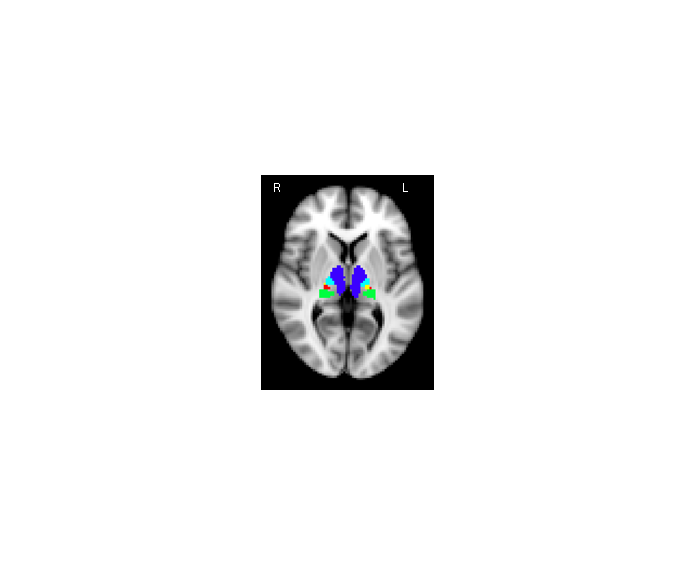
Figure 1.
FSL Oxford probabilistic atlas of sub-thalamic regions, segmented according to
their white-matter connectivity to cortical areas, overlaid on the MNI-152 T1
image in MNI space. Blue: pre-frontal; Light-blue: pre-motor; Yellow: primary
motor; Red: sensory; Green: posterior parietal.
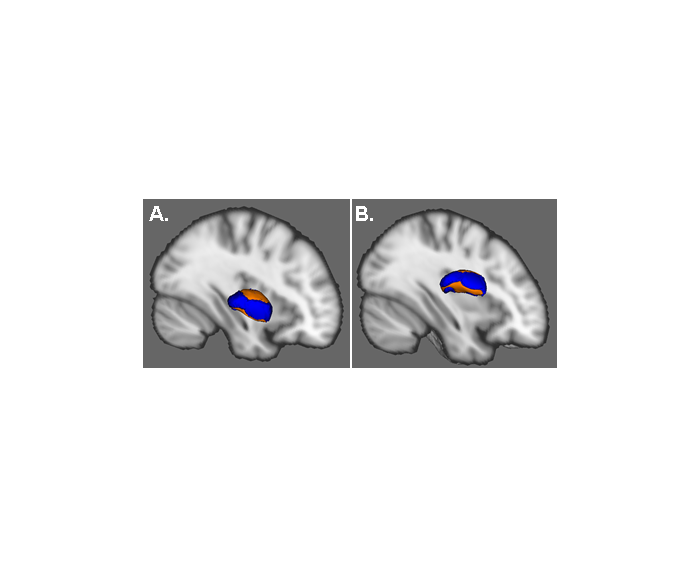
Figure 2.
3D-view results of the shape analysis in
MNI space for the left thalamus in CLBP vs. controls. Orange represents regions
with significant surface depression (p<0.05, corrected for multiple
comparisons using FDR) in CLBP compared to controls. Blue represents the
regions with non-significant surface changes between groups. A. Rotate
to view the dorsal surface of the left thalamus. B. Rotate to view the
ventral surface of the left thalamus.
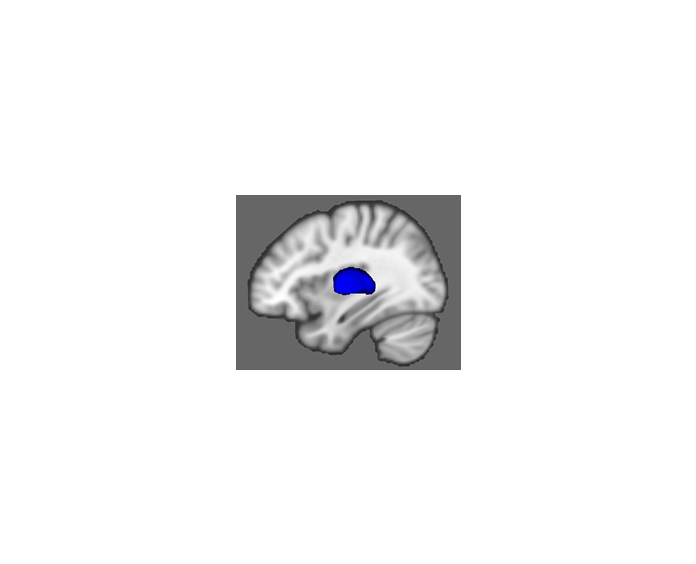
Figure 3. 3D-view results
of the shape analysis in MNI space for the right thalamus in CLBP vs. controls.
Blue represents the regions with non-significant surface change (p>0.05,
corrected for multiple comparisons using FDR) between groups.