2602
Changes in GABA associated with a sham-controlled transcranial direct current stimulation language intervention for primary progressive aphasia.1Department of Radiology, University of Calgary, Calgary, AB, Canada, 2Children’s Hospital Research Institute and Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada, 3Department of Biostatistics, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States, 4Department of Neurology, Johns Hopkins School of Medicine, Baltimore, MD, United States, 5Department of Otolaryngology Head & Neck Surgery, Johns Hopkins School of Medicine, Baltimore, MD, United States, 6Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins School of Medicine, Baltimore, MD, United States, 7F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, MD, United States
Synopsis
Primary Progressive Aphasia is a neurodegenerative disorder primarily affecting language. We applied GABA-edited MRS to examine GABA changes with anodal tDCS to augment language-therapy for patients with PPA. With tDCS targeting the left inferior frontal gyus, we see a decrease in IFG GABA following the intervention. No changes were observed in the sham group. While all patients showed improvements with language therapy, those receiving tDCS showed greater improvements that were maintained at 2 months follow-up. This work supports the use of tDCS to augment language therapy in PPA.
Introduction
Transcranial direct current stimulation (tDCS) passes a weak current between two electrodes and appears to modulate cortical excitability, increasing excitability at the anode and decreasing excitability at the cathode.[1] Studies in young, healthy, control adults suggest that anodal tDCS (atDCS) increases glutamate and/or decreases GABA at the anode.[2-4] Changes in glutamate and GABA and the associated changes in inhibition and excitation are proposed to provide an optimal neural environment for plasticity and learning.[1] tDCS has shown potential to augment language therapy for Primary Progressive Aphasia (PPA), a neurodegenerative disorder that primary affects language.[5,6] This study applied GABA-edited MRS to examine metabolite changes in a sham-controlled study applying tDCS to augment language therapy in PPA. We expect decreases in GABA in the left inferior frontal gyrus (IFG), the site of simulation.Methods
Twenty-two patients diagnosed with PPA were recruited to participate in a language-therapy and tDCS intervention that consisted of 15 sessions over ~3 weeks. Patients were randomized to atDCS (n=11) or sham (n=11) for the duration of the study. Imaging and language assessments were performed at baseline, after the intervention and 2 months post-intervention.
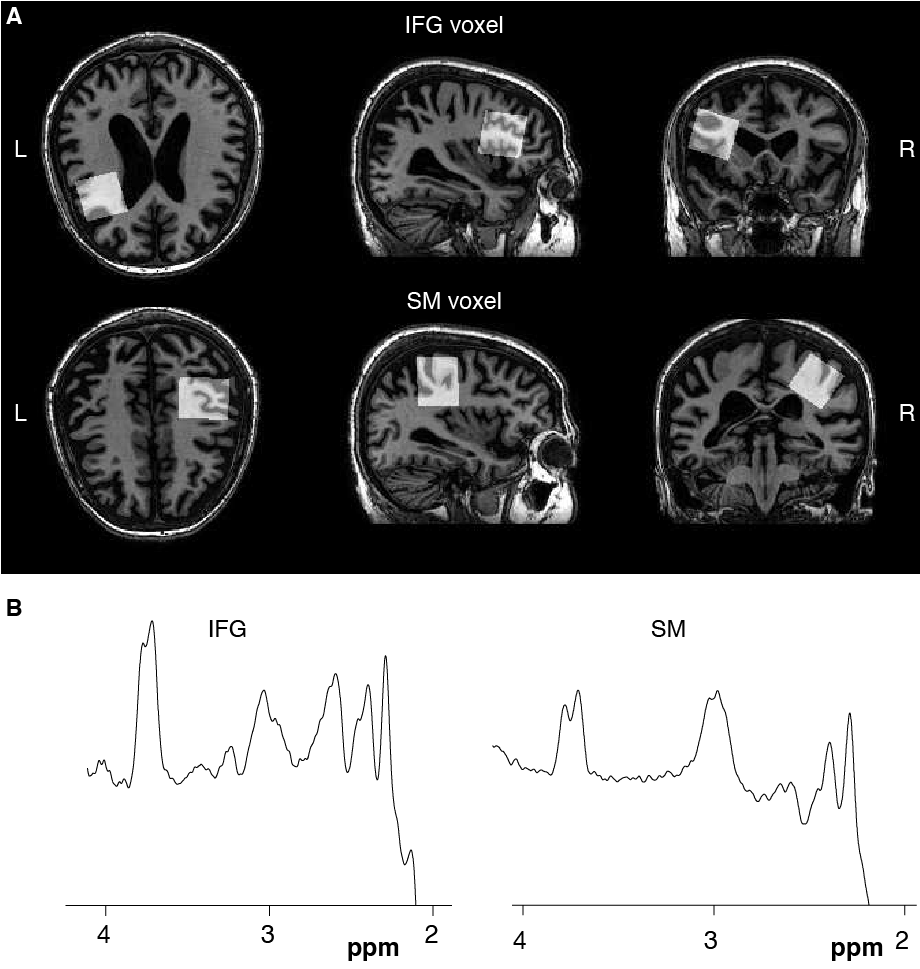
Imaging was performed at 3T (Phillips, Acheiva) and included a whole-brain MPRAGE sequence (TR/TE=8 ms/3.75 ms, 1mm3 isotropic voxels) for voxel placement and tissue segmentation. GABA-edited MEGA-PRESS data (TR/TE=2s/68 ms, 14 ms editing pulses at 1.9 ppm and 7.46 ppm alternating every 2 averages, 320 averages, 8 unsuppressed water scans for quantification) were collected from two 3×3×3 cm3 voxels. One voxel was centered on the left IFG (Figure 1) and a control voxel was placed on the right sensorimotor cortex (SM). GABA data were analyzed using the Gannet pipeline [7,8] including tissue correction.
tDCS (Model 1500, Soterix) was applied using 2-inch square saline soaked electrodes with the anode over the left IFG (electrode F7 in the EEG 10-20 system). The cathode was placed on the participant’s right cheek. For atDCS, 2mA of current (ramped up from 0 mA over 30 sec) was applied for 20 min. For sham, a validated procedure was followed.[9] The language therapy has been described previously [5,10] and includes oral and written tasks. Scoring is reported as a percentage of possible points. Language therapy started at the beginning of tDCS and lasted for 45-50 mins (i.e., 25-30 min after tDCS finished).
Changes in GABA and language score comparing baseline to post-intervention and baseline to 2-month follow-up were tested using paired t-tests within the atDCS and sham groups. Dropouts at the 2-month follow-up were assumed to be random. Welch two-sample t-tests with Satterthwaith degrees of freedom (DF) were applied for comparison of language scores between the two groups due to the inequality of group variances.[11]
Results
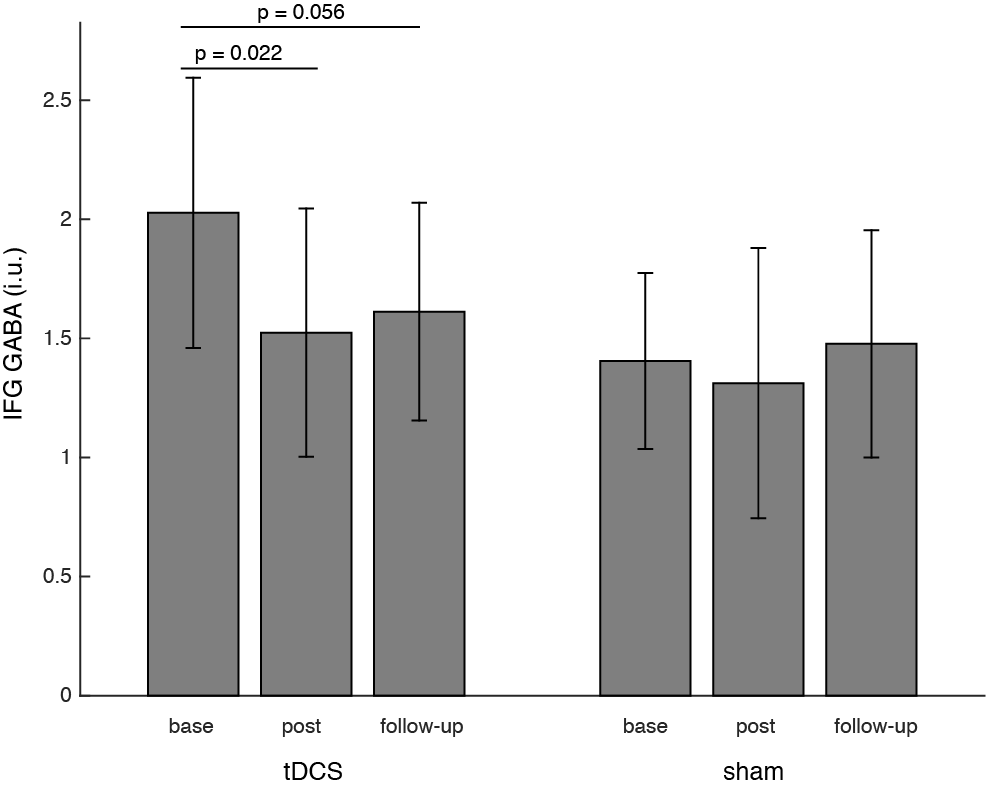
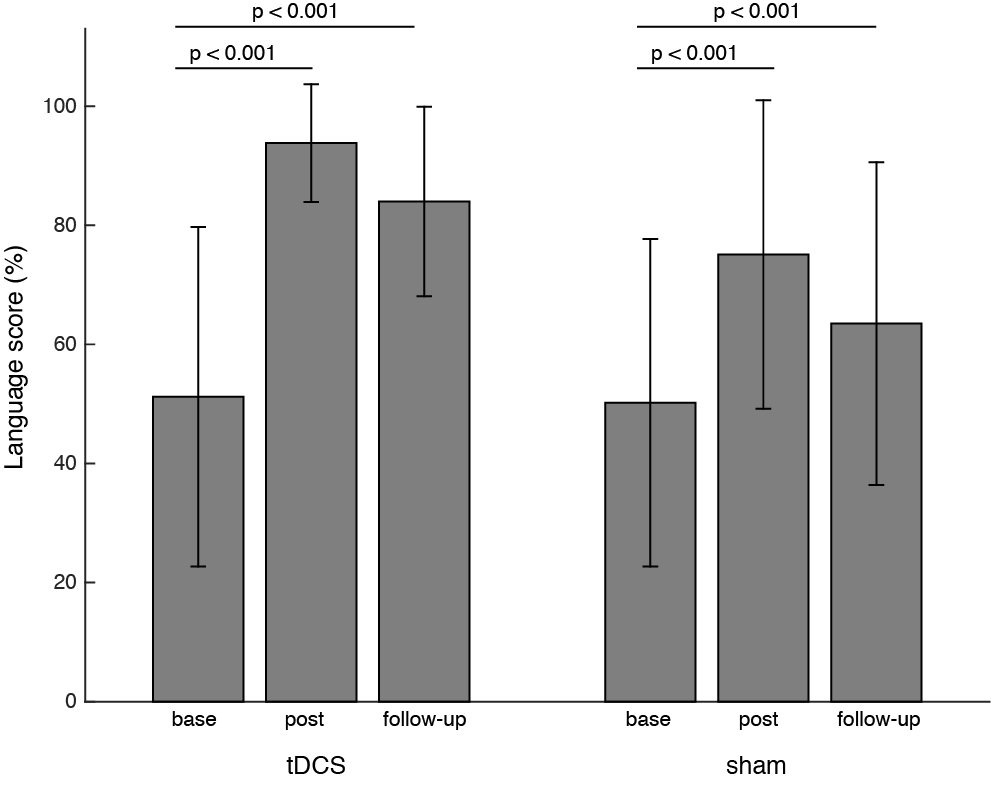
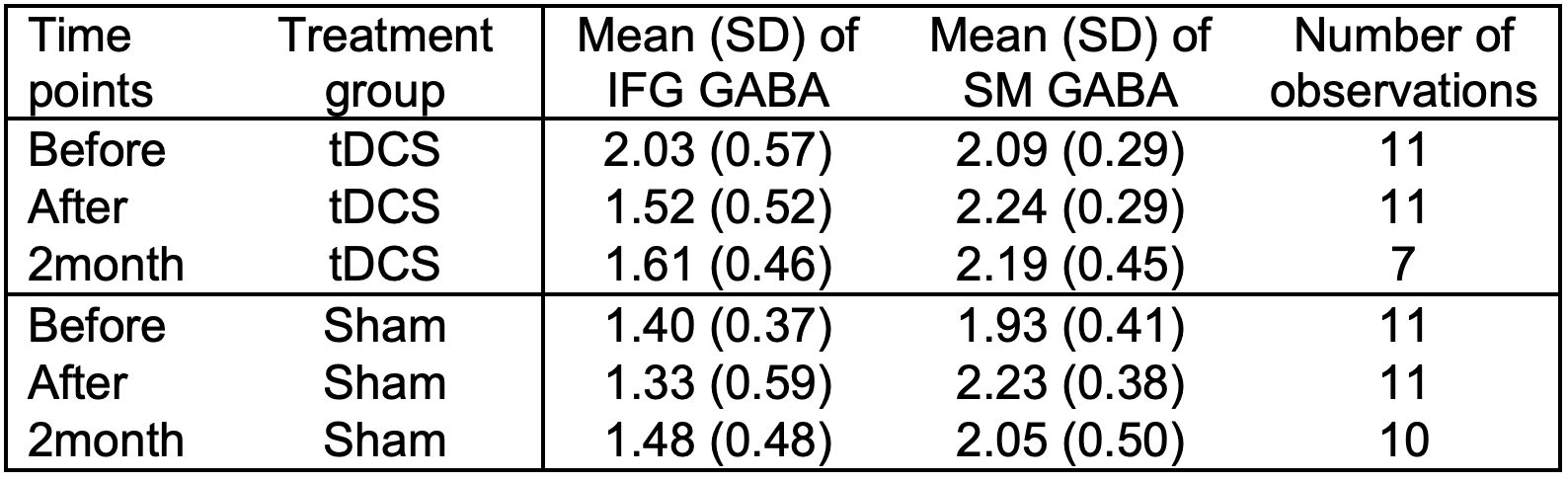
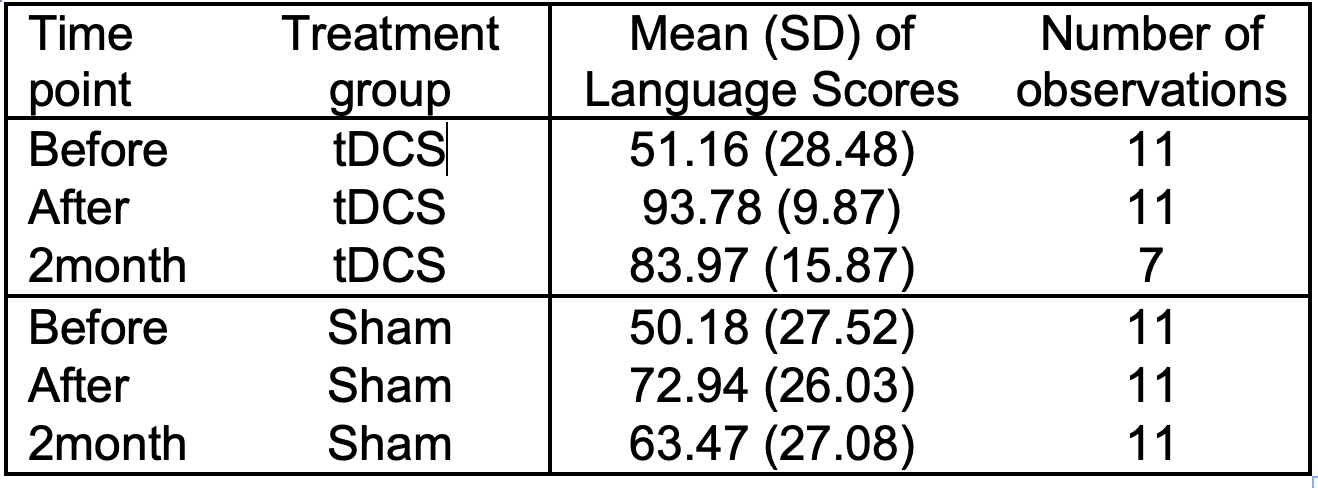
Tables 1 and 2 summarize raw data and final group sizes. GABA in the IFG of the atDCS group significantly decreased directly after the tDCS intervention compared to baseline (DF=10, T=-2.70, p=0.022) and non-significantly at 2-months follow-up (DF=6, T=-2.37, p=0.056). GABA did not change in the IFG of the sham group and no changes were seen in the SM voxel of either group (Figure 2). All patients showed improvements in language scores (Figure 3). The atDCS group significantly improved from an average baseline score of 51.2%±28.5% to 93.8%±9.9% (DF=10, T=5.13, p<0.001) after the intervention and maintained a significant improvement at follow-up (average score = 83.9%±15.9%, DF=6, T=4.34, p=0.005). The sham group significantly improved (DF=10, T=5.02, p<0.001) from a baseline score of 50.2%±27.5% to 72.9%±26.0% after the intervention. At 2-months follow-up the average language score was 63.5%±27.1%, also significantly higher than baseline (DF=10, T=4.57, p=0.001). Increase in language scores of the atDCS group compared to the sham group was confirmed from the baseline to the 2-months follow-up (atDCS average increase=40.94, sham average increase=13.29, DF=7.15, T=2.79, p=0.026), but not significantly immediately after the intervention.
Discussion
As expected, GABA decreased in the IFG (target tissue) in the atDCS group after the intervention. Interestingly, the GABA reduction was sustained at 2 months follow-up. It is accepted that GABA decreases for learning and neuroplasticity but we expected it to return towards baseline after learning has completed [12]. This sustained reduction in GABA may reflect on-going learning and plasticity, as patients likely continued to work on their language skills. Alternatively, it may indicate the effects of atDCS are more long-term than previously predicted. All patients showed language improvements but atDCS group showed greater improvements that persisted after 2 months. These results support the use of tDCS to augment language therapy in PPA and provide new insight into the persistence of GABA reductions following atDCS.Acknowledgements
We would like to thank our participants and referring physicians for their dedication and interest in our study. This work was supported by grants from the Science of Learning Institute at Johns Hopkins University and by the National Institutes of Health (National Institute of Deafness and Communication Disorders) through award R01 DC014475 to KT.References
[1] Krause B, Márquez-Ruiz J, Kadosh RC. The effect of transcranial direct current stimulation: a role for cortical excitation/inhibition balance? Front Hum Neurosci 2013;7.
[2] Clark VP, Coffman BA, Trumbo MC, Gasparovic C. Transcranial direct current stimulation (tDCS) produces localized and specific alterations in neurochemistry: a 1 H magnetic resonance spectroscopy study. Neurosci Lett 2011;500:67–71.
[3] Kim S, Stephenson MC, Morris PG, Jackson SR. tDCS-induced alterations in GABA concentration within primary motor cortex predict motor learning and motor memory: a 7T magnetic resonance spectroscopy study. Neuroimage 2014;99:237–243.
[4] Stagg CJ, Best JG, Stephenson MC, O’Shea J, Wylezinska M, Kincses ZT, et al. Polarity-sensitive modulation of cortical neurotransmitters by transcranial stimulation. J Neurosci 2009;29:5202–5206.
[5] Tsapkini K, Frangakis C, Gomez Y, Davis C, Hillis AE. Augmentation of spelling therapy with transcranial direct current stimulation in primary progressive aphasia: Preliminary results and challenges. Aphasiology 2014;28(:1112–30.
[6] Cotelli M, Manenti R, Petesi M, Brambilla M, Cosseddu M, Zanetti O, et al. Treatment of primary progressive aphasias by transcranial direct current stimulation combined with language training. J Alzheimers Dis JAD 2014;39:799–808.
[7] Harris AD, Puts NA, Edden RA. Tissue correction for GABA-edited MRS: Considerations of voxel composition, tissue segmentation, and tissue relaxations. J Magn Reson Imaging 2015;42:1431–1440.
[8] Edden RA, Puts NA, Harris AD, Barker PB, Evans CJ. Gannet: A batch-processing tool for the quantitative analysis of gamma-aminobutyric acid–edited MR spectroscopy spectra. J Magn Reson Imaging 2014;40:1445–1452.
[9] Gandiga PC, Hummel FC, Cohen LG. Transcranial DC stimulation (tDCS): a tool for double-blind sham-controlled clinical studies in brain stimulation. Clin Neurophysiol Off J Int Fed Clin Neurophysiol 2006;117:845–50.
[10] Beeson PM, Egnor H. Combining treatment for written and spoken naming. J Int Neuropsychol Soc JINS 2006;12:816–27.
[11] Ruxton. The unequal variance t-test is an underused alternative to Student's t-test and the Mann–Whitney U test. Behavioral Ecology 2006; 17: 688-900.
[12] Floyer-Lea, Wylezinska, Kincses, Matthews. Rapid modulation of GABA concentration in the human sensorimotor cortex during motor learning. J Neurophysiol 2006; 95: 1639–1644.
Figures