2597
Towards identification of neuroanatomical correlates of neuropsychological scores in Parkinson’s disease patients, with and without, memory impairment1Imaging Research, Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, United States, 2Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, United States, 3University of California, San Diego, San Diego, CA, United States, 4Department of Neurology and Neurosciences Stanford Movement Disorders Center (SMDC), Stanford University, Stanford, CA, United States
Synopsis
With a well-characterized dataset of Parkinson’s disease (PD) participants, with and without memory impairment, this study shows that there is a distinct structural network organization between PD with mild cognitive impairment (PD-MCI) and without MCI(PD-nMCI). This study further shows that while there are no discernible differences in scalar diffusion-MRI derived measures, fractional anisotropy in PD-nMCI is negatively associated with trail making test-A. Our study demonstrates the feasibility towards identifying neuroanatomical correlates of neuropsychological scores that will not only aid in our understanding of the underlying neural correlates of cognitive impairment in PD, as well as differentiating PD-MCI and PD-nMCI in an objective and reproducible manner.
Introduction
Mild Cognitive Impairment (MCI) are common in Parkinson’s disease (PD), even in early stages of the disease1. Current clinical diagnosis of PD-MCI is based on the criteria defined by the task force from the International Parkinson and Movement Disorder Society2. According to this subjective criteria, PD-MCI is diagnosed if neuropsychological tests reveal deficits in at least 2 out of the 5 cognitive domains tested. In this study, we collected diffusion-weighted MRI (dMRI) data on a well-characterized cohort of PD-MCI and PD-nMCI participants to identify neuroanatomical correlates of the neuropsychological scores employed in the clinical diagnosis of PD-MCI. We hypothesized that there will be differences between PD-MCI and PD-nMCI in the scalar diffusion-derived measures in addition to a shift in the structural network organization pattern.Methods
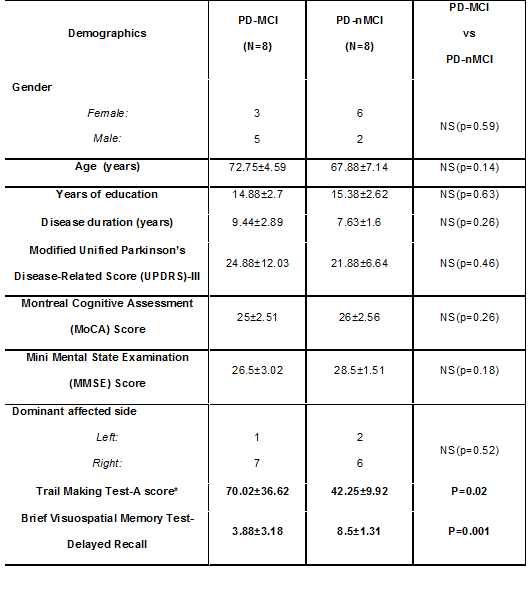
Participants: 32 PD participants were recruited at our Center for Neurodegeneration and Translational Neuroscience, Cleveland Clinic Lou Ruvo Center for Brain Health. 16/32 participants were identified as PD-MCI according to the current clinical diagnostic criteria, and neurological evaluations. Although the cognitive profile used for diagnosis of PD-MCI is heterogeneous, in general, we see two forms of cognitive impairment in PD-MCI: one with features of “cortical impairments” (likely to have concurrent AD) and one with the frontal-striatal impairments (likely to have pure PD). The selection of the Trail Making Test A (TMT-A) and Brief Visual Memory Test-Delayed Recall (BVMT) was chosen to capture these deficits. These selective criteria yielded 8/16 PD-MCI with deficits in TMT-A and BVMT. Age, education, gender, disease duration, handedness, and global cognition matched PD-nMCI were randomly chosen from 8/16 PD-nMCI participants. All PD participants used in this study were in the practically defined “ON” condition (with levodopa). Data acquisition: 71 directions high spatial resolution (1.5mm3) dMRI data was acquired for every participant with b-value of 1000s/mm2. 25 non-diffusion weighted (b0) images interspersed between diffusion encoding directions were also acquired. Both dMRI and b0s were acquired with P>>A phase encoding direction. To correct for eddy current distortion a b0 data was acquired with A>>P. In addition, MMSE, MoCA, and the Movement Disorders Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) III motor scores were also collected for every participant. Processing: Eddy-current distortion was performed on every participant using FSL3, and single tensor was fitted for every participant using FSL. Voxelwise estimate of various scalar dMRI-derived metrics was then obtained and was statistically compared between the groups, along with testing for association with clinical observation metrics. Graph-theoretical analysis: Whole-brain deterministic tracking was performed using TrackVis4. AAL5 and ATAG6 atlas were transformed to each participant’s native space to generate the nodes for the graph-theoretical approach. Symmetric structural connectivity matrix was generated for every participant where every element of the matrix was binarized if there is a tract having its end in both nodal region of interest (ROI). Of note, tracts shorter than 10mm7 or having fractional anisotropy (FA) <0.2 were removed from this analysis. Various graph-theoretical properties were computed using GRETNA8 or in-house MATLAB scripts. Statistical analysis: Network-based statistic (NBS)9 was used to compare structural network disorganization between groups. PALM9 in FSL was used to statistically compare voxelwise scalar dMRI-derived metrics and graph-theoretical measures between the groups, and identify the association of dMRI-derived metrics and graph-theoretical measures with clinical observations in each group. All statistical measures were considered significant either at family-wise error corrected p<0.05 or at uncorrected p<0.001.Results
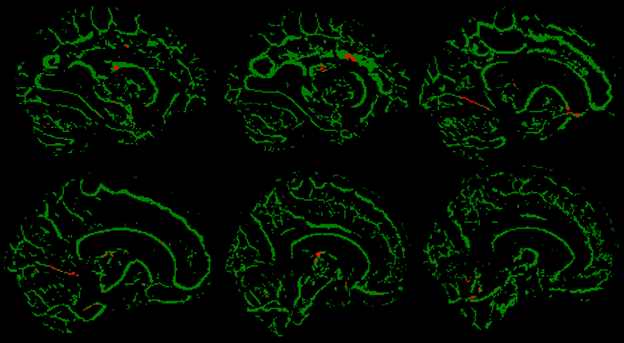
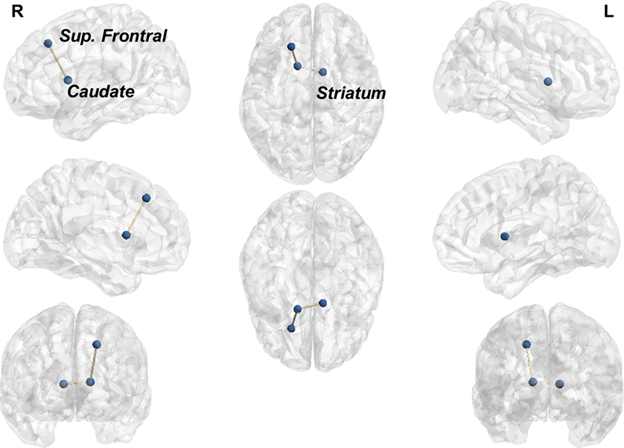
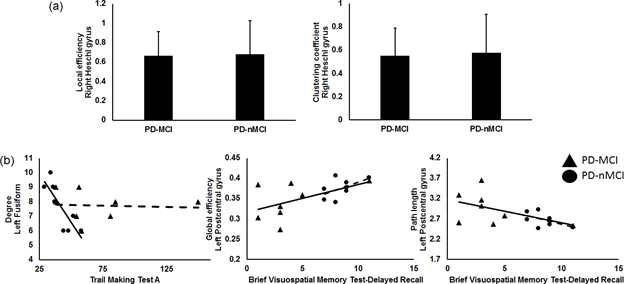
As outlined in Table.1, there were no statistical differences in the demographics of the participants, disease duration, MoCA, MMSE, dominant affected side, MDS-UPDRS-III motor scores. No statistical difference was observed in any dMRI-derived metrics between groups. There was a significant negative association between FA and TMT-A in PD-nMCI (Figure.1) in regions encompassing the cingulum, inferior longitudinal fasciculus, and anterior thalamic radiation tracts. Significantly stronger connectivity was observed in PD-nMCI between striatal-frontal-caudate ROIs (Figure.2). The right Heschl gyrus had a significantly lower local efficiency and clustering coefficient in PD-MCI (Figure.3a). Significantly positive association between global efficiency of the left postcentral gyrus and BVMT in PD-MCI was found. Significantly negative association between left fusiform degree and TMT-A in PD-nMCI, and path length of left postcentral gyrus and BVMT in PD-MCI was also observed (Figure.3b).Discussion and Conclusion
Our preliminary analysis revealed disrupted structural organization that was differentially associated with performance on cognitive measures in PD-MCI and PD-nMCI. Our study demonstrates the feasibility towards identifying neuroanatomical correlates of neuropsychological scores that will not only aid in our understanding of the underlying neural correlates of cognitive impairment in PD, as well as differentiating PD-MCI and PD-nMCI in an objective and reproducible manner.Acknowledgements
This work was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number 5P20GM109025, and private grant funds from the Peter and Angela Dal Pezzo funds, and the young scientist award.References
1 Williams-Gray CH, Mason SL, Evans JR, Foltynie T, Brayne C, Robbins TW et al. The CamPaIGN study of Parkinson’s disease: 10-year outlook in an incident population-based cohort. J Neurol Neurosurg Psychiatry 2013; 84: 1258–1264.
2 Litvan I, Goldman JG, Troster AI, Schmand BA, Weintraub D, Petersen RC et al. Diagnostic criteria for mild cognitive impairment in Parkinson’s disease: Movement Disorder Society Task Force guidelines. Mov Disord 2012; 27: 349–356. 3 Andersson JLR, Sotiropoulos SN. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage 2016; 125: 1063–1078.
4 Wang R, Wedeen VJ. TrackVis.org. In: Proc Intl Soc Mag Reson Med. 2007, p 3720.
5 Tzourio-Mazoyer N, Landeau B, Papathanassiou D, Crivello F, Etard O, Delcroix N et al. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002; 15: 273–289.
6 Keuken MC, Bazin P-L, Crown L, Hootsmans J, Laufer A, Muller-Axt C et al. Quantifying inter-individual anatomical variability in the subcortex using 7 T structural MRI. Neuroimage 2014; 94: 40–46.
7 Cheng H, Wang Y, Sheng J, Sporns O, Kronenberger WG, Mathews VP et al. Optimization of seed density in DTI tractography for structural networks. J Neurosci Methods 2012; 203: 264–272.
8 Wang J, Wang X, Xia M, Liao X, Evans A, He Y. GRETNA: a graph theoretical network analysis toolbox for imaging connectomics. Front Hum Neurosci 2015; 9: 386.
9 Zalesky A, Fornito A, Bullmore ET. Network-based statistic: identifying differences in brain networks. Neuroimage 2010; 53: 1197–1207.
Figures