2595
Disruption of cortical-basal ganglia motor network affects cognitive function in Parkinson’s disease: a high angular resolution diffusion imaging study1Electronics and Information Engineering, Harbin Institute of Technology at Shenzhen, Shenzhen, China, 2Department of Neurobiology, Neurology and Geriatrics, Xuanwu Hospital of Capital Medical University, Beijing, China, 3Harbin Institute of Technology at Shenzhen, Shenzhen, China
Synopsis
Whether clinical phenotype in Parkinson's disease (PD) is affected by cortical-basal ganglia motor circuit (CBG) dysfunction remains to be investigated. In this study, we utilized a high angular resolution diffusion imaging (HARDI) technique to investigate association between white matter structural connectivity within CBG and cognitive function related to PD. We found that the structural connectivity between the M1 cortical area and other regions within the CBG circuit decreased for those PD patients with severe cognitive symptoms, indicating that the less effective information processing between cortical and subcortical regions in CBG network could lead to cognitive deficits in PD patients.
Introduction
The imbalanced dopamine modulatory in cortical-basal ganglia motor circuit (CBG) is a hallmark of Parkinson’s disease (PD). Previous studies have reported structural and functional deficits within CBG network in PD patients1,2, however, whether clinical phenotype is affected by CBG dysfunction remains to be investigated. Although PD is often characterized as a movement disorder, cognitive decline or dementia affects nearly half of patients. In this study, we utilized a high angular resolution diffusion imaging (HARDI) technique to investigate association between white matter structural connectivity within CBG and cognitive function related to PD.Methods
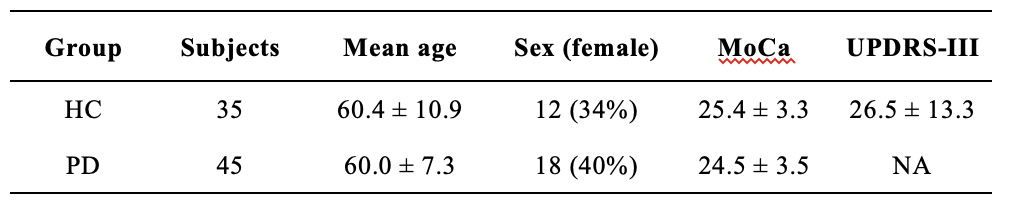
Images from 45 PD patients and 35 healthy controls (HC) recruited by Xuanwu Hospital of Capital Medical University were selected for this study. Demographic and clinical data obtained for patients including motor disability (UPDRS III) and Montreal Cognitive Assessment (MoCA) scales were summarized in Table 1. All the subjects underwent Siemens Skyra 3T MR scans with an MPRAGE sequence (TR = 7 ms, TE = 3 ms, FOV = 256 × 256, thickness/gap =1.2/1.2 mm, flip angle = 8) and spin echo EPI sequence (TR = 5000 ms, TE = 105 ms, FOV = 256 × 256, flip angle = 90, isotropic voxel size = 2 mm, 60 gradient directions with b = 1000/2000 s/mm2). After preprocessing of HARDI images including head-motion, eddy-current and field inhomogeneity correction, fiber orientations from DWI images are estimated using constrained spherical deconvolution (CSD) coupled with a probabilistic streamline algorithm by MRtrix 3 softeware3, with the following tractography parameters: fibre orientation distribution amplitude threshold = 0.1, step size = 1.25 mm, 4 samples per step and maximum curvature per step = 45. The spherical-deconvolution informed filtering (SIFT) algorithm was further applied on the whole brain tractograms to reduce reconstruction biases. To locate the brain structures with CBG circuit on each individual derived tratograms, the T1 weighted images were first linearly coregistrated to b0 image for each individual. After N4ITK bias correction, T1 images of all the subjects were parcellated through a fully automated atlas-based parcellation platform (www.MRICloud.org), resulting an individual-based anatomical parcellation of CBG parcels including supplementary motor area (SMA), primary motor cortex (M1), caudate (Caud), thalamus (Thal), globus pallidus (GP), and putamen (Put) in both hemispheres. Therefore, an individual CBG structural network could be constructed with edges defined as the number of connections per unit surface between the above CBG parcels using a correction term of edge length4.
For the statistical analysis, we applied general linear modal (GLM) to measure the relationship between clinical scales and nodal degree of CBG network on the participants, with age and sex adjusted. The nodal degree is defined as sum of all edges connected with one parcel, representing total connectivity strength of a single structure. Type I errors were controlled by false discovery rate correction. For those significant parcels returned by GLM analysis, Spearman correlation analysis was further conducted. A p value of 0.05 or less for all tests in this study was considered statistically significant.
Results
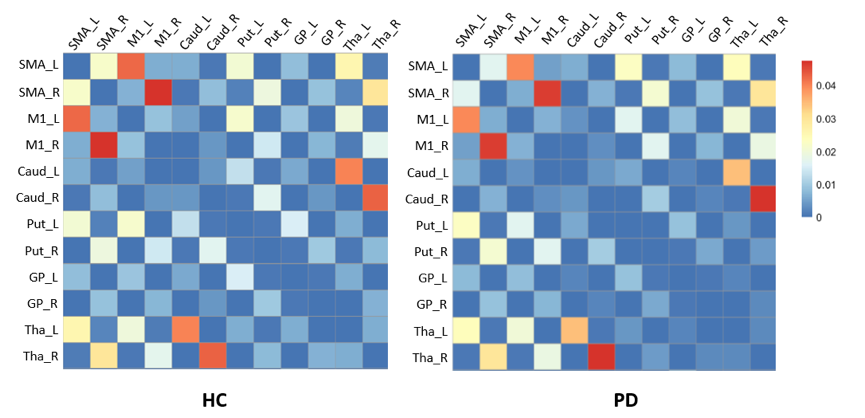
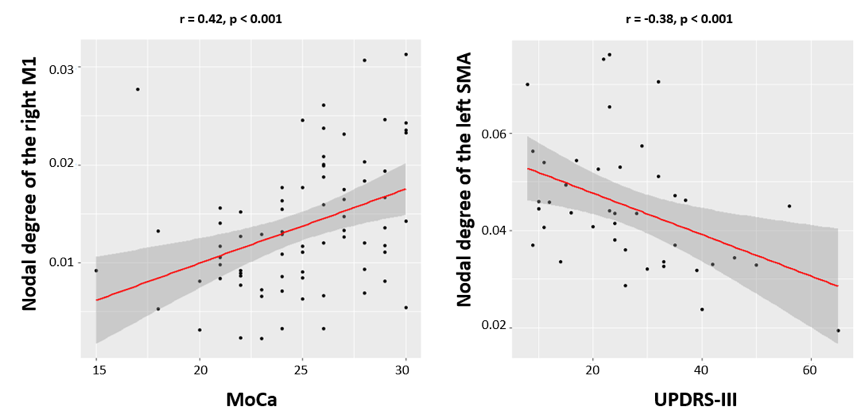
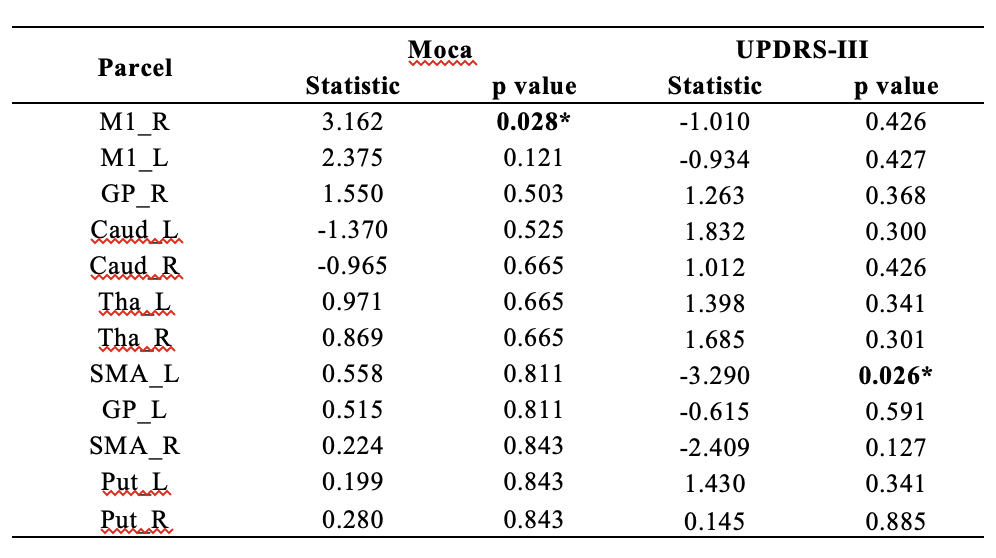
Fig.1 demonstrats the mean correlation matrix of CBG network for each group. The nodal degree of the right M1 is significantly associated with MoCa score among all participants (p = 0.028), and the nodal degree of the left SMA is significantly associated with UPDRS-III score among PD patients (p = 0.026), as shown in Table 2. Spearman correlation analysis reveals that the nodal degree of the right M1 is significantly positive correlated with MoCa score (r = 0.42, p < 0.001), and the left SMA exhibits significantly decreased nodal degree as the UPDRS motor score increases (r = -0.38, p < 0.001), as shown in Fig. 2.Discussion
The present study was designed to investigate the association between structural connectivity of the CBG circuit and cognitive function in PD patients. From the results of GLM analysis, the structural connectivity related to a key region of the CBG circuit was found to be correlated with motor dysfunction, which has been consistently reported in previous studies2. More importantly, we found that the structural connectivity between the M1 cortical area and other regions within the CBG circuit decreased for those PD patients with severe cognitive symptoms. This finding indicates that the less effective information processing between cortical and subcortical regions in CBG network could lead to cognitive deficits in PD patients, which will help better explore the pathophysiology underlying the dementia in PD. Another merit of this study is the employment of HARDI technique, since it can provide superior delineations of white matter tracts than the diffusion tensor model, especially robust in crossing fiber scenario.Acknowledgements
This study is supported by grants from the Basic Research Foundation Key Project Track of Shenzhen Science and Technology Program (JCYJ20160509162237418, JCYJ20170413110656460).References
1. Wei L, Zhang J, Long Z, et al. Reduced Topological Efficiency in Cortical-Basal Ganglia Motor Network of Parkinson's Disease: A Resting State fMRI Study. Plos One, 2014, 9(10):e108124.
2. Sharman, Michael, Valabregue, Romain, Perlbarg, Vincent, et al. Parkinson's disease patients show reduced cortical-subcortical sensorimotor connectivity. Movement Disorders, 2013, 28(4):447-454.
3. Tournier J.D, Calamante F, et al. MRtrix: Diffusion tractography in crossing fiber regions. International Journal of Imaging Systems and Technology, 2012, 22(1).
4. Hagmann P, Cammoun L, Gigandet X, et al. Mapping the Structural Core of Human Cerebral Cortex. Plos Biology, 2008, 6(7):e159.
Figures