2592
Temporal Atrophy Predicts the Deterioration of Cognition in Multiple Domains: a Longitudinal Clinical Study in Parkinson’s Disease1Department of Radiology, The Second Affiliated Hospital, Zhejiang University School of Medicine, HangZhou, China
Synopsis
To specify the critical structural alterations of cognitive deterioration in Parkinson’s disease (PD) and explored the underlying mechanism of structural changes. We combined cross-sectional and longitudinal VBM analyses to explore the structural topologies between PD patient who convert to mild cognitive impairment (PD converter). The relationships between dopamine transporter (DAT), CSF proteins and structural alterations were assessed. PD converters showed progressive temporal atrophy associated with multiple cognitive domains. DAT results were significantly associated with temporal atrophy. In conclusion, temporal lobe is a crucial node in modulating cognitive status in multi-domains. Dopamine deficiency may contribute to cognition-related temporal atrophy.
Introduction
Cognitive impairment is a common symptom in the trajectory of Parkinson’s disease (PD). Structural alterations were explored by researchers and found extensive cortical and subcortical atrophy might be related to the development of cognitive impairment in PD 1-6. However, the critical alterations of cognitive impairment, especially the differences between PD patients who convert to PD-MCI (PD converters) and those who remain cognitively stable (PD nonconverters) were unclear. Moreover, few studies have explored the association between PD related metabolic and pathological alterations and the gray matter (GM) changes.
Thus, we combined cross-sectional and longitudinal voxel-based morphometry (VBM) analyses to observe the structural topologies of PD converters and further update current knowledge regarding the roles of pathological proteins as well as dopamine in cognition related structural alterations.
Methods
This retrospective study collected fifty-one PD patients with normal cognition at baseline and 25 healthy controls (HCs) from PPMI. Those who convert to PD-MCI at follow-up (mean 12 months) were classified as PD converters (n = 18). And patients keep cognitively intact at follow-up were defined as PD nonconverters (n=33).
Clinical and neuropsychological data, MRI scans, dopamine transporter (DAT) scans and Cerebrospinal fluid (CSF) specimens (Aβ42, α-syn, and p-tau) information were included in this study. According to the DAT results, the striatal binding ratios (SBRs) in the right and left caudate nucleus and putamen were calculated separately.
We analyzed the GM volume differences in cross-sectional comparison and explored the progressive alterations within group. The relationships between GM atrophy and cognitive performance were assessed. Furthermore, DAT and CSF proteins were compared among three groups and the relationships with GM atrophy were evaluated.
Results
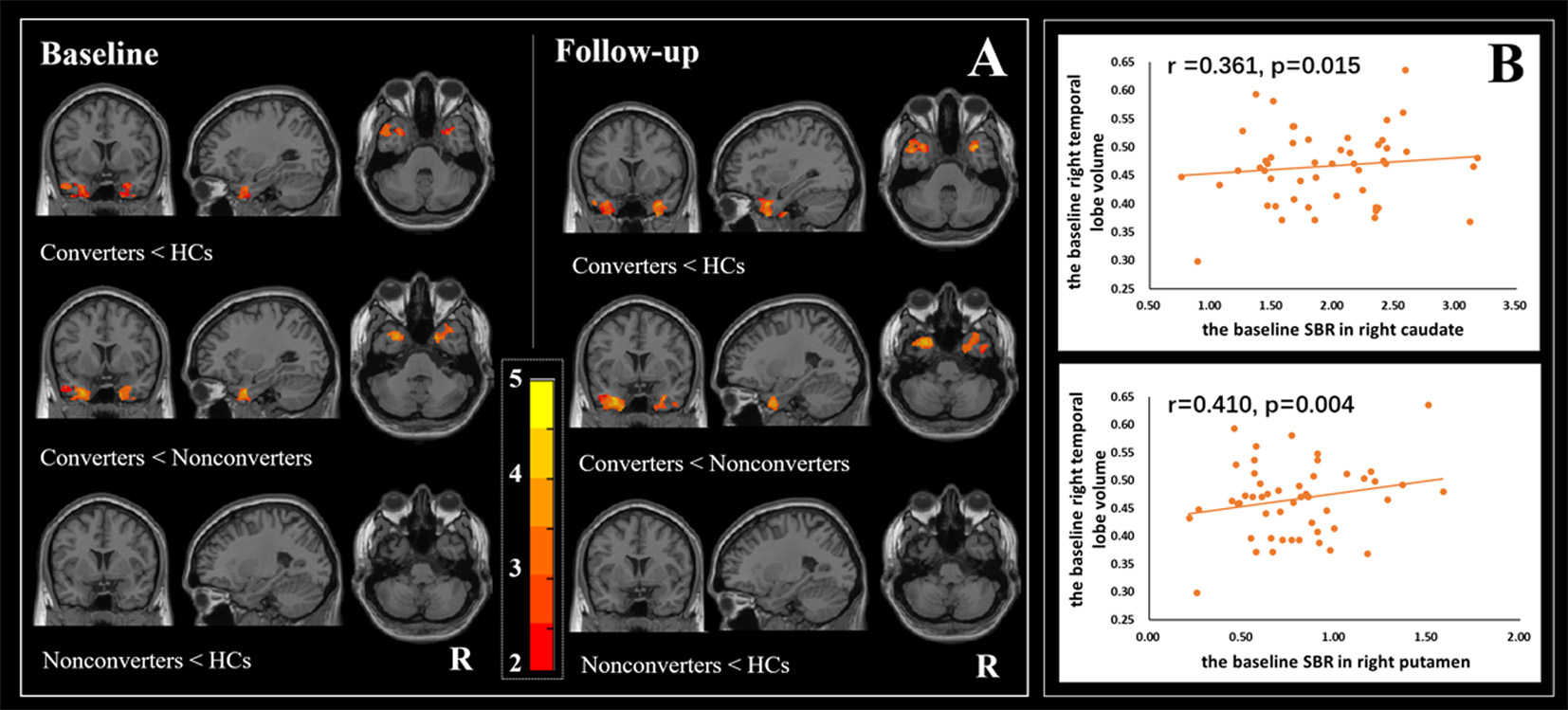
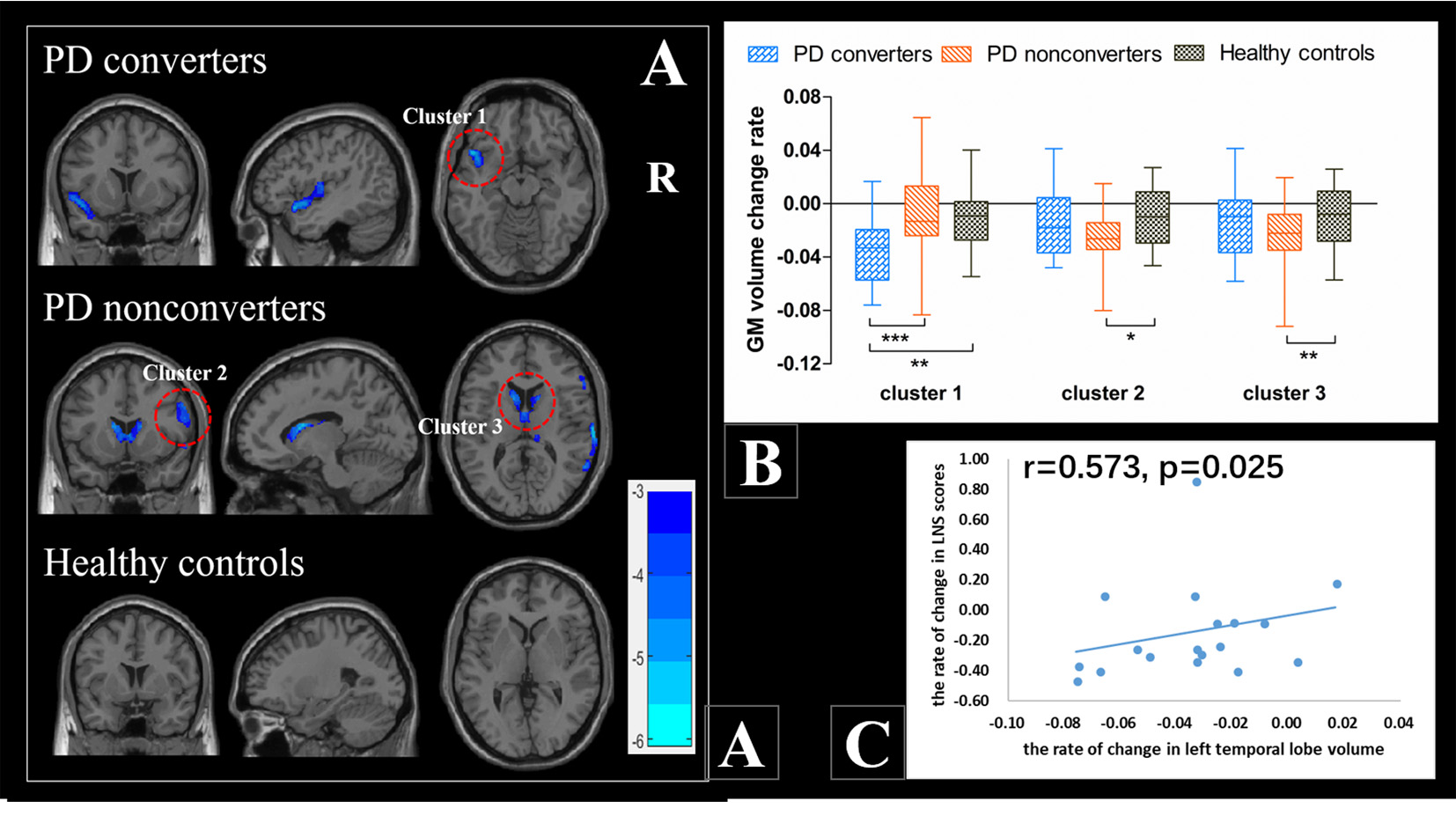
Cross-sectionally, PD converters showed bilateral temporal atrophy at baseline, and progressive atrophy in these regions at follow-up (Figure 1A). Longitudinal comparison within group also showed increased left temporal atrophy in PD converters (Figure 2).
In PD patients, the temporal volume was positively correlated with visuospatial function which showed poor performance at baseline. And the temporal atrophy was correlated with the cognitive performance in multiple domains which were poor performed at follow-up.
The SBRs of the caudate and putamen were significantly associated with the temporal atrophy (Figure 1B). No correlation was found between CSF proteins and temporal atrophy.
Discussion
Firstly, growing evidences showed that neuroimaging alterations in temporal lobe which caused by pathological changes of PD and Alzheimer’s disease were closely associated with cognitive decline in PD 3, 5, 7. Consistent with our findings, Mak et al. observed significant temporal cortical thinning in PD converters 1. The well-matched results of correlation analysis and cognitive performance further demonstrated the crucial role of temporal atrophy in the future cognitive decline in multiple domains.
Then, temporal cortex also receive abundant dopaminergic innervation and reduced dopamine receptor of the temporal lobe was detected in PD patients by using F18-DOPA positron emission tomography (PET) scan 8, 9. Credible evidence suggested that the denervation of temporal lobes could contribute to the posterior cortical deficits 10. And the loss of dopamine further influenced the function and structure of cortex 11-13. A recent hybrid PET/MR study revealed that the degeneration of striatal dopaminergic could contribute to the alterations of GM density through cortical-striatal circuits in PD 14. Consistently, a recent study report that DAT density was correlated with the GM volume of temporal gyrus in PD patients. Therefore, dopaminergic deficit might be a potential cause of cognition related temporal atrophy in PD.
Conclusion
In conclusion, our research provided a better understanding of the deterioration of cognitive impairment in PD and dopamine deficiency related structural alterations should come into our notice.Acknowledgements
The authors thank the team at the department of Radiology, the Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310009, China. And the data used in the preparation of this article were obtained from the PPMI database (www.ppmi-info.org/data). PPMI—a public-private partnership—is funded by the Michael J. Fox Foundation for Parkinson's Research and funding partners, including Abbvie, Allergan, Avid, Biogen, Biolegend, Bristol-Myers Squibb, GE Healthcare, Genentech, GlaxoSmithKline, Lilly, Lundbeck, Merck, Meso Scale Discovery, Pfizer, Piramal, Roche, SANOFI GENZYME, Servier, Takeda, Teva, and UCB (www.ppmi-info.org/fundingpartners).References
1. Mak E, Su L, Williams GB, et al. Baseline and longitudinal grey matter changes in newly diagnosed Parkinson's disease: ICICLE-PD study. Brain. 2015-10-01 2015;138(Pt 10):2974-2986.
2. Kandiah N, Zainal NH, Narasimhalu K, et al. Hippocampal volume and white matter disease in the prediction of dementia in Parkinson's disease. Parkinsonism Relat Disord. 2014-11-01 2014;20(11):1203-1208.
3. Pereira JB, Svenningsson P, Weintraub D, et al. Initial cognitive decline is associated with cortical thinning in early Parkinson disease. Neurology. 2014-06-03 2014;82(22):2017-2025.
4. Agosta F, Canu E, Stefanova E, et al. Mild cognitive impairment in Parkinson's disease is associated with a distributed pattern of brain white matter damage. Hum Brain Mapp. 2014-05-01 2014;35(5):1921-1929.
5. Hanganu A, Bedetti C, Degroot C, et al. Mild cognitive impairment is linked with faster rate of cortical thinning in patients with Parkinson's disease longitudinally. Brain. 2014-04-01 2014;137(Pt 4):1120-1129.
6. Foo H, Mak E, Yong TT, et al. Progression of subcortical atrophy in mild Parkinson's disease and its impact on cognition. Eur J Neurol. 2017-02-01 2017;24(2):341-348.
7. Braak H, Ghebremedhin E, Rub U, Bratzke H, Del TK. Stages in the development of Parkinson's disease-related pathology. Cell Tissue Res. 2004-10-01 2004;318(1):121-134.
8. Picco A, Morbelli S, Piccardo A, et al. Brain (18)F-DOPA PET and cognition in de novo Parkinson's disease. Eur J Nucl Med Mol Imaging. 2015-06-01 2015;42(7):1062-1070. 9. Joyce JN, Janowsky A, Neve KA. Characterization and distribution of [125I]epidepride binding to dopamine D2 receptors in basal ganglia and cortex of human brain. J Pharmacol Exp Ther. 1991-06-01 1991;257(3):1253-1263.
10. Nobili F, Abbruzzese G, Morbelli S, et al. Amnestic mild cognitive impairment in Parkinson's disease: a brain perfusion SPECT study. Mov Disord. 2009-02-15 2009;24(3):414-421.
11. Tian T, Qin W, Liu B, et al. Catechol-O-methyltransferase Val158Met polymorphism modulates gray matter volume and functional connectivity of the default mode network. Plos One. 2013-01-20 2013;8(10):e78697.
12. Williams-Gray CH, Hampshire A, Barker RA, Owen AM. Attentional control in Parkinson's disease is dependent on COMT val 158 met genotype. Brain. 2008-02-01 2008;131(Pt 2):397-408.
13. Scherfler C, Esterhammer R, Nocker M, et al. Correlation of dopaminergic terminal dysfunction and microstructural abnormalities of the basal ganglia and the olfactory tract in Parkinson's disease. Brain. 2013-10-01 2013;136(Pt 10):3028-3037.
14. Choi H, Cheon GJ, Kim HJ, et al. Gray matter correlates of dopaminergic degeneration in Parkinson's disease: A hybrid PET/MR study using (18) F-FP-CIT. Hum Brain Mapp. 2016-05-01 2016;37(5):1710-1721.
Figures
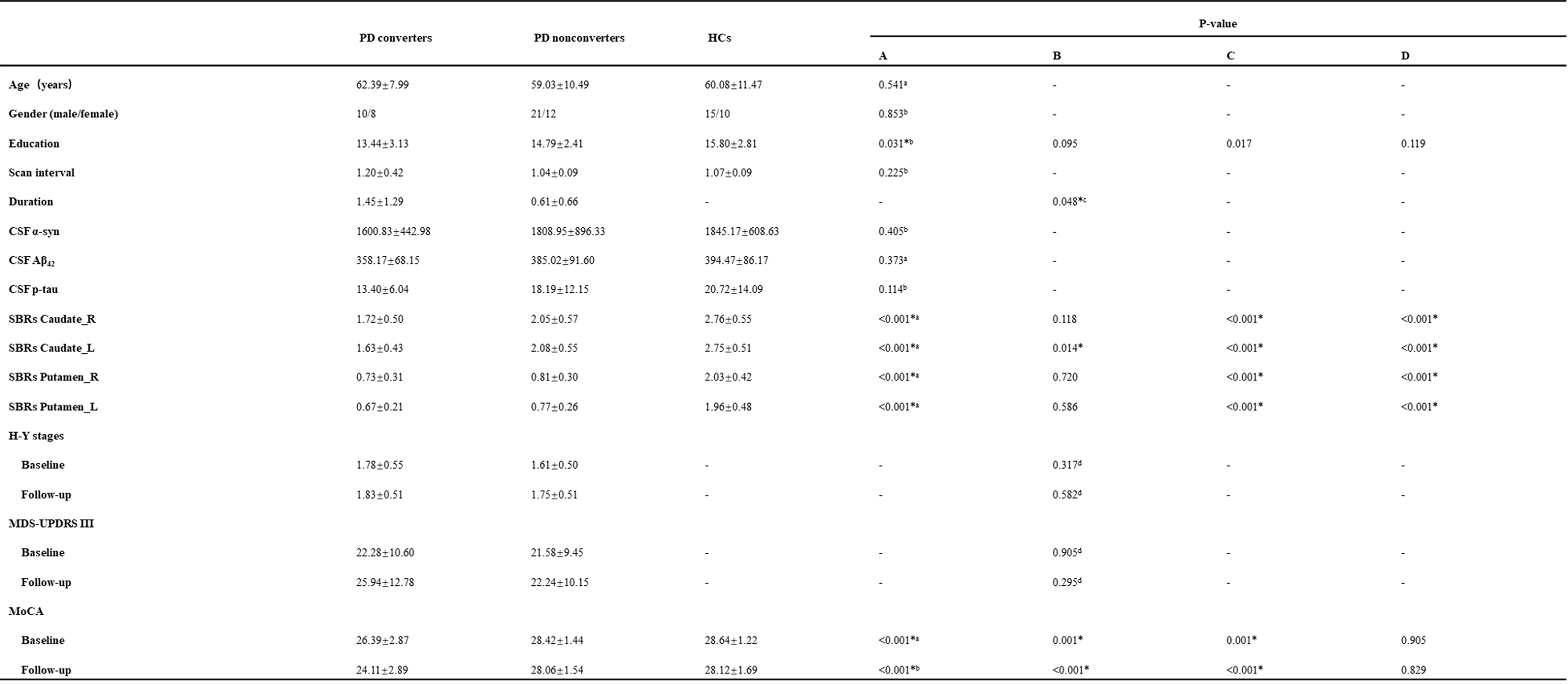
Baseline and longitudinal participants characteristics.
R: Right; L: Left; MDS-UPDRS III: part III of the Movement Disorder Society Unified Parkinson’s Disease Rating Scale; CSF: cerebrospinal fluid; SBRs: striatal binding ratios; MoCA: Montreal Cognitive Assessment. A = Comparison among PD converters, nonconverters and HCs; B = PD converters vs PD nonconverters; C = PD converters vs HCs; D = PD nonconverters vs HCs. a ANOVA = PD converters, PD nonconverters, HCs; b Kruskal Wallis Test = PD converters, PD nonconverters and HCs; c Wilcoxon rank-sum test = PD converters, PD nonconverters; d Independent Sample T test = PD converters, PD nonconverters
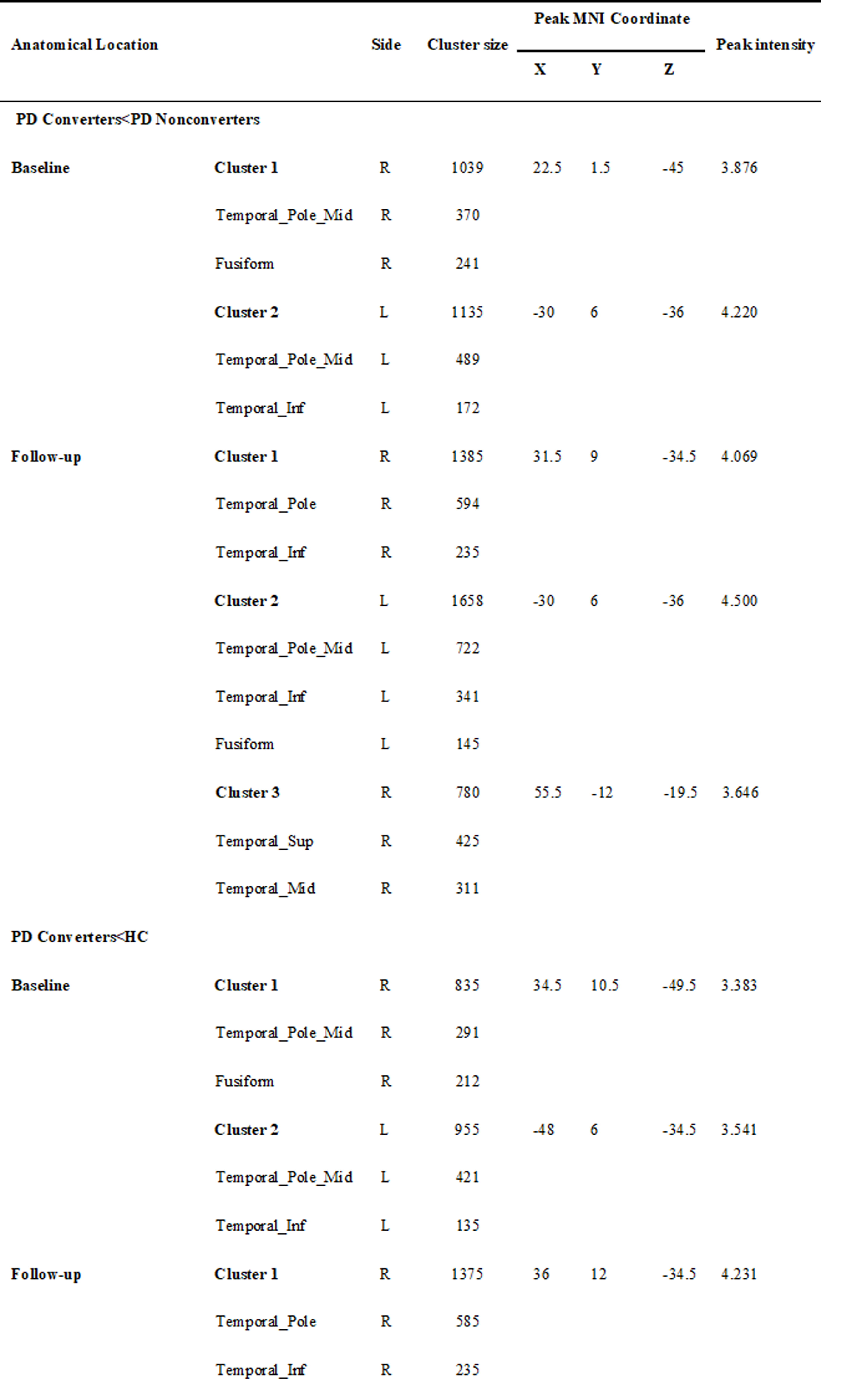
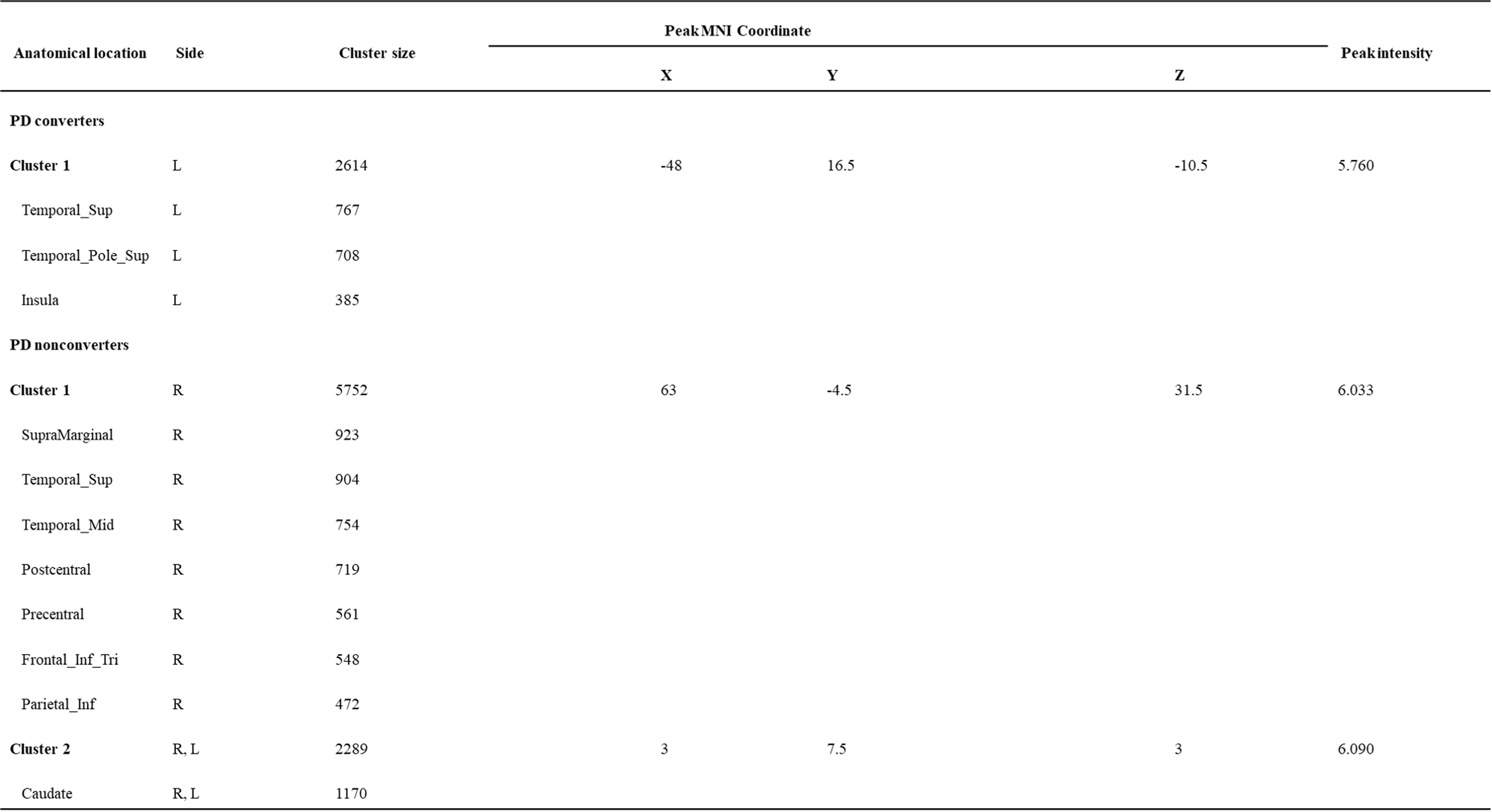
Anatomical location of significant GMV differences among three groups.
R: Right; L: Left; Sup: superior; Mid: middle; Inf: inferior.
Significant GMV differences in longitudinal comparison.
R: Right; L: Left. Sup: superior; Mid: middle; Inf: inferior.