2590
Acupuncture Relieve Pain in Parkinson’s Disease Through Modulating Pain Matrix1Medical Imaging and Radiology Science, Chang Gung University, TaoYuan, Taiwan, 2Department of acupuncture, Chang Gung Memorial Hospital, TaoYuan, Taiwan, 3Medical Imaging and Intervention, Chang Gung Memorial Hospital, TaoYuan, Taiwan, 4Neurology, Chang Gung Memorial Hospital, TaoYuan, Taiwan
Synopsis
Patients with Parkinson’s Disease may suffer from different pain for years, including aching and burning from muscles, skeleton, or even throughout their body. In the current study, we provide that acupuncture could relieve such specific pain in PD patients through modulating regions related to the pain matrix in brain, especially correlated with primary somatosensory cortex and middle temporal pole. This could be an effective and safe analgesic tool that would relieve patients’ suffering.
INTRODUCTION
Patients with Parkinson’s Disease1may suffer from different pain for years, including aching and burning from muscles, skeleton, or even throughout their body2.Acupuncture has been widely practiced as complementary medicine, which has been used clinically for efficient pain relief3, such as lower back pain, chronic pain or cancer pain4. The aim of our study is to provide image-based evidence of the effectiveness in PD-related pain relief and to investigate the underlying neuro-mechanism by using resting state fMRI.METHODS
The study was approved by the Institutional Review Board, and complied with the Declaration of Helsinki.
Sixteen patients with PD were recruited, who were divided into the acupuncture group (9 (Male/Female = 4/5, aged 60.7±6.3 year old) and the control group (7(Male/Female = 5/2, aged 70.4±8.2 year old). The acupuncture group was treated with both acupuncture and analgesic treatment and the control was treated with analgesic agent only. The diagnosis of idiopathic PD was made according to the UK Brain bank criteria5. The clinical performance was evaluated, including 1) the King’s Parkinson’s Disease Pain Scale (KPPS), 2) Visual Analogue Scale, 3) Beck Depression Inventory-II, 4) Parkinson’s Disease Sleep Scale-2, 5) the 39-Item Parkinson’s Disease Questionnaire, 6) Unified Parkinson’s Disease Rating Scale, and 7) Mini Mental State Examination. Three acupoints were consistently used throughout the complete treatment course, including Bai-Hui (GV20), Kidney Guan (LE44), Yanglingquan (GB34).
Images were acquired using a 3T MR scanner (MAGNETOM Trio a TIM system, Siemens, Erlangen, Germany)at enrollment (baseline) and the end of treatment (complete).The structural images (T1weighted MPRAGE) were acquired using the following parameters: TR/ TE/ TI = 2000/2.63/900 ms, flip angle = 9°, 160 axial slices of voxel size = 1 × 1 × 1 mm3. The resting state fMRIimages were acquired with an Echo Planar Imaging sequence by the following parameters: TR/TE = 3000/45 ms, flip angle=90°, 40 axial slices of voxel size = 3 × 3 × 3 mm3. Subjects were instructed to stay still and not to move, with their eyesopen during the acquisition.
The resting state fMRI was processed by using DPARSF software6. All the statistical analyses were performed in PASW Statistics 21 with significance threshold p < 0.05, and the bonferroni correction was performed for the multiple comparison.
RESULTS
The total score of KPPS and UPDRS decreased significantly in the acupuncture group, compared to control (p=0.023 and 0.005, respectively). A significant decrease of 46.2% in the KPPS total score was observed.
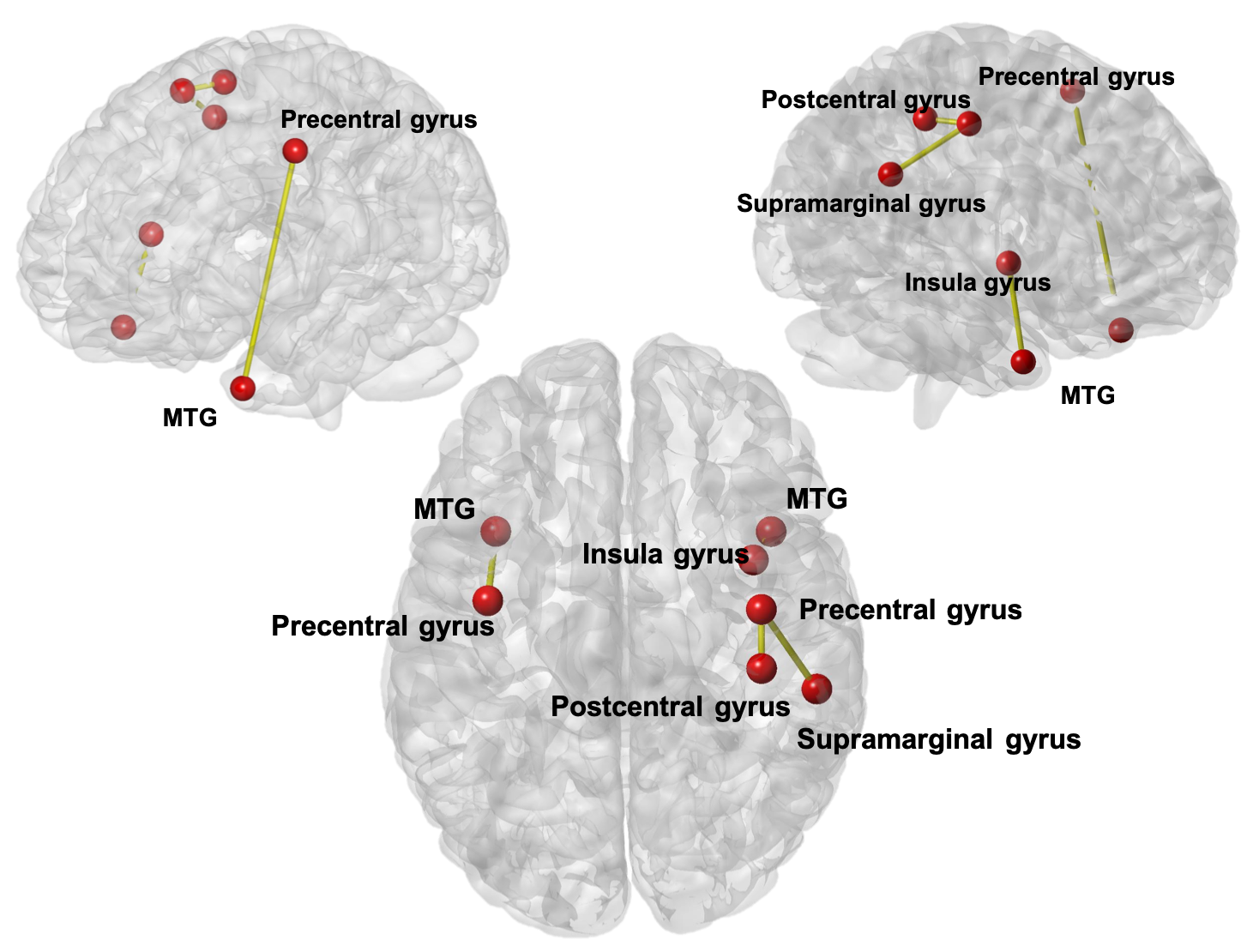
Figure 1 showed the significant changes of brain connectivity between two visits in the acupuncture group, compared to the control group. Four functional connectivities and seven anatomical regions are found with increased connectivity. The involved connectivity included the connection between the middle temporal pole and precentral area on the left; postcentral and precentral on the right; supramarginal gyrus and precentral on the right, and middle temporal and insula gyrus on the right.
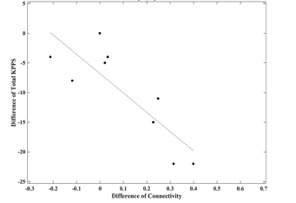
Figure 2 showed the negative correlation between the changes of functional connectivity and total score of KPPS (pre and post treatment) in the acupuncture group in the connection between postcentral gyrus and middle temporal pole on the left side (R = -0.798).
DISCUSSION
Firstly, the effective of pain relief by prescribed fixed acupuncture pointsin PD patients provided an alternative way to improve patients’ life quality. Secondly, the current study indicated modulation in the brain connectivity for pain relief as a result of the acupuncture treatment in patients with PD. The regions with the significant changes of connectivity are part of the pain matrix7, and the increased connectivity might suggest an alteration by the acupuncture treatment in the neural network of patients with PD.
Specifically, the primary somatosensory cortex and middle temporal pole not only participated in the pain matrix, but also associated with the multisensory such as processes visual, odor, and auditory information8, 9. The acupuncture treatment induced enhancement of activity in these regions suggested that the pain relief mechanism of acupuncture might not improving the disease of PD but modulating the sense of pain in brain.
Finally, negative correlation between KPPS and functional connectivity of postcentral and middle temporal pole might further imply that acupuncture relieve the pain through enhancing the connectivity strength.
CONCLUSION
Acupuncture could relieve such specific pain in PD patients through modulating regions related to the pain matrix in brain, especially correlated with primary somatosensory cortex and middle temporal pole. This could be an effective and safe analgesic tool that would relieve patients’ suffering.Acknowledgements
No acknowledgement found.References
1. Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord 2008;23(15):2129-2170.
2. Skogar O, Lokk J. Pain management in patients with Parkinson's disease: challenges and solutions. J Multidiscip Healthc 2016;9:469-479.
3. Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for Chronic Pain: Update of an Individual Patient Data Meta-Analysis. J Pain 2018;19(5):455-474.
4. White A, Foster NE, Cummings M, Barlas P. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology (Oxford) 2007;46(3):384-390.
5. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55(3):181-184.
6. Chao-Gan Y, Yu-Feng Z. DPARSF: A MATLAB Toolbox for "Pipeline" Data Analysis of Resting-State fMRI. Front Syst Neurosci 2010;4:13.
7. Legrain V, Iannetti GD, Plaghki L, Mouraux A. The pain matrix reloaded: a salience detection system for the body. Prog Neurobiol 2011;93(1):111-124.
8. Antal A, Temme J, Nitsche MA, Varga ET, Lang N, Paulus W. Altered motion perception in migraineurs: evidence for interictal cortical hyperexcitability. Cephalalgia 2005;25(10):788-794.
9. Kim W, Kim SK, Nabekura J. Functional and structural plasticity in the primary somatosensory cortex associated with chronic pain. J Neurochem 2017;141(4):499-506.
Figures