2581
Prognosis of body function in Parkinson’s disease using diffusion magnetic resonance imaging1Healthy Aging Research Center, Chang Gung University, TaoYuan, Taiwan, 2Department of Medical Imaging and Radiological Sciences, Chang Gung University, TaoYuan, Taiwan, 3Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Linkou, Taiwan, 4Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Keelung, Taiwan, 5Neuroscience Research Center, Chang Gung Memorial Hospital, Linkou, Taiwan, 6Clinical Informatics and Medical Statistics Research Center, Chang Gung University, TaoYuan, Taiwan, 7Department of Neurology, Landseed Hospital, TaoYuan, Taiwan
Synopsis
Parkinson’s disease (PD) is a common progressive neurodegenerative disorder characterized by resting tremor, bradykinesia, restricted mobility, and postural instability. PD has a progressive course and is associated with increased mortality, with physical disability and non-motor symptoms exerting a significant negative impact on quality of life. Robust early prediction of clinical outcomes in Parkinson’s disease would be paramount for implementing appropriate management interventions. The predictive power varied according to the clinical measures used and was highest in the prediction of UPDRS. This finding was further confirmed by using bootstrap approach and leave-one-out cross-validation analysis.
INTRODUCTION
Parkinson’s disease (PD) is a common progressive neurodegenerative disorder characterized by resting tremor, bradykinesia, restricted mobility, and postural instability. PD has a progressive course1 and is associated with increased mortality2, with physical disability and non-motor symptoms exerting a significant negative impact on quality of life3. Robust early prediction of clinical outcomes in Parkinson’s disease would be paramount for implementing appropriate management interventions. We therefore examined the prognostic performance of baseline diffusion MRI, measured from multiple affected brain regions, in the prediction of 2-year severity in Parkinson’s disease.
METHODS
The present study was approved by the institutional review board of ChangGung Medical Systems and conducted in accordance with the Declaration of Helsinki A total of 109 patients with PD (61 males and 48 females, mean age: 61.2 ± 7.1 years) were recruited between June 2012 and May 2015. Only patients returned for the follow-up examination were used in the prognosis analysis, which included 82 subjects (45 males and 37 females, mean age: 60.9 ± 7.3 years) who visited between June 2014 and 2015 (after a mean of 23.7±0.7 months). All participants were diagnosed and treated according to the normal clinical routine. The following parameters were recorded: body mass index, education. The following measures were used in the analysis: disease severity by the Unified PD Rating Scale (UPDRS), Modified Hoehn and Yahr staging (MHY) and Levodopa equivalent daily dose (LEDD). MRI was performed on a 3T scanner (Trio, A TIM system, Magnetom, Siemens, Erlangen, Germany). The imaging parameters for T1-weighted images were: repetition time/echo time/inversion time/flip angle = 2000 ms/2.63 ms/900 ms/9°, slice thickness = 1 mm, number of slices = 160, voxel size = 1 × 1 × 1 mm3. Diffusion-weighted images were acquired using a spin-echo echo-planar-imaging sequence with repetition time/echo time/slice thickness = 5700 ms/108 ms/3 mm, number of slices = 40, voxel size = 2 × 2 × 3 mm3. The b-value was 1000 s/mm2 and applied along 30 non-collinear directions. Diffusion images were normalized and parcellated according to Automatic Anatomical Labelling template. Statistical analyses were performed in SPSS 20. Parameters selected by least absolute shrinkage and selection operator (LASSO) were entered into a stepwise multivariate regression model, followed by a leave-one-out cross validation.Results
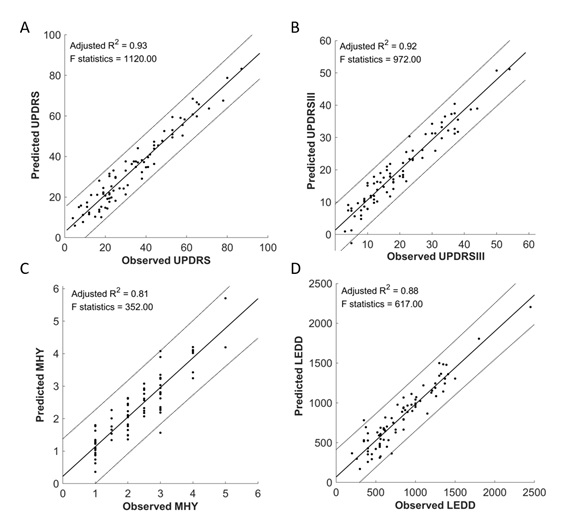
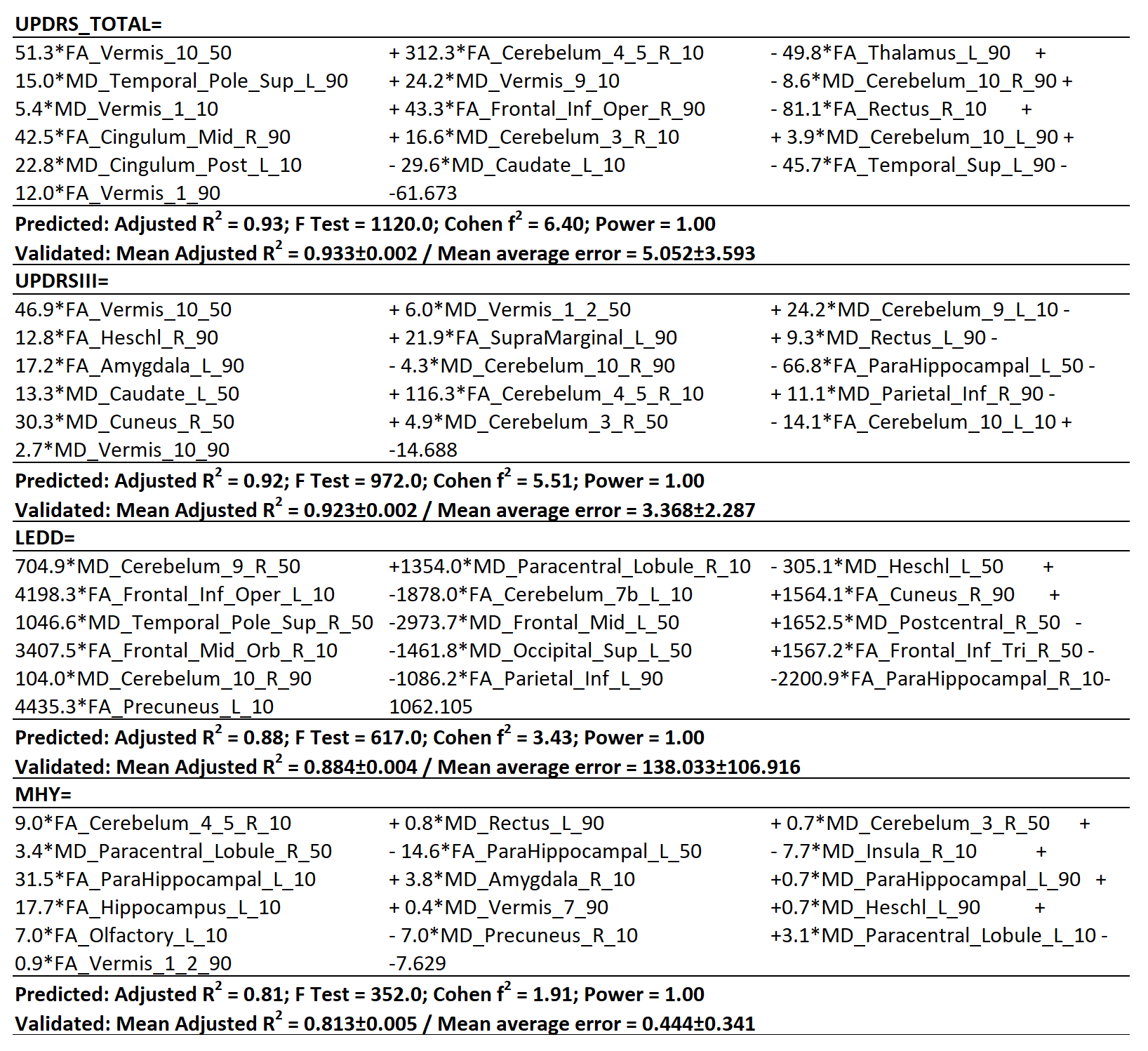
Regression analyses revealed strong-to-excellent associations between baseline diffusion parameters and clinical parameters at follow-up. All of the variance inflation factors were both within the normal range and <3.1, which suggests that the assumption of multicollinearity was not violated. The predicted score at follow-up were plotted against the observed value in Figure 1, including the total score of UPDRS, motor subdomain of UPDRS, LEDD, and MHY. The observed UPDRS at follow-up were significantly in line with those predicted by regression models with the highest adjusted R2 (predicted 0.93, cross validation 0.933±0.002, maximum error at 5.052±3.593 Panel A, Figures 1). UPDRS III, the motor subdomain of UPDRS, can be predicted at an adjusted R2 (predicted 0.92, cross validation 0.923±0.002, maximum error at 3.368±2.287 Panel B, Figures 1). Noticeably, MHY can be predicted at an adjusted R2 (predicted 0.81, cross validation 0.813±0.005, maximum error at 0.444±0.341 Panel C, Figures 1). LEDD can be also predicted at an adjusted R2 of 0.88 (both at prediction and validation, Panel D, Figures 1). Dependent variables and the corresponding unstandardized coefficients for each assessment are reported, from which clinical changes in individual patient could be calculated by the combination of diffusion parameters calculated from multiple brain regions (Table 1).Discussion
The study proposed to examine the prognostic performance of diffusion MRI on the clinical severity of patients with PD. The results of our study indicate that the clinical severity over a 2-year follow-up period can be confidently predicted by baseline diffusion parameters measured in multiple parcellated brain regions. The brain connectivity within a whole neural network was found to alter in PD patients, which might be changed to a relatively normal pattern by the administration of levodopa4. Our observations of the multiple cortical involvement might lend further support to the contention that the pathogenesis and severity of PD could extend far beyond the basal ganglia5-7. Importantly, diffusion parameters were found to predict the clinical trajectory of PD over time on an individual patient basis. The predictive power varied according to the clinical measures used and was highest in the prediction of UPDRS. This finding was further confirmed by using bootstrap approach and leave-one-out cross-validation analysis.Acknowledgements
No acknowledgement found.References
1. Morrish PK, Rakshi JS, Bailey DL, Sawle GV, Brooks DJ (1998) Measuring the rate of progression and estimating the preclinical period of Parkinson's disease with [18F]dopa PET. J Neurol Neurosurg Psychiatry 64:314-319 2
2. Louis ED, Marder K, Cote L, Tang M, Mayeux R (1997) Mortality from Parkinson disease. Arch Neurol 54:260-264 3
3. Menon B, Nayar R, Kumar S et al (2015) Parkinson's Disease, Depression, and Quality-of-Life. Indian J Psychol Med 37:144-148 4
4. Wu T, Wang L, Chen Y, Zhao C, Li K, Chan P (2009) Changes of functional connectivity of the motor network in the resting state in Parkinson's disease. Neurosci Lett 460:6-10 5
5. Blandini F, Nappi G, Tassorelli C, Martignoni E (2000) Functional changes of the basal ganglia circuitry in Parkinson's disease. Prog Neurobiol 62:63-88 6
6. Brooks DJ (2010) Imaging approaches to Parkinson disease. J Nucl Med 51:596-609 7
7. Calabresi P, Picconi B, Tozzi A, Ghiglieri V, Di Filippo M (2014) Direct and indirect pathways of basal ganglia: a critical reappraisal. Nat Neurosci 17:1022-1030
Figures