2575
Cortical thinning pattern according to the differential nigrosome involvement in patients with Parkinson’s disease1Department of Radiology, Gachon University Gil Medical Center, Incheon, Korea, Republic of, 2Department of Radiology, The Catholic University of Korea, Seoul, Korea, Republic of, 3Department of Biomedical Engineering, College ofHealth and Medical Science, Catholic University of Daegu, Gyeongsan-si, Gyeongbuk, Korea, Republic of, 4Department of Neurology, Gachon University Gil Medical Center, Incheon, Korea, Republic of
Synopsis
The dopaminergic neurons within the substantia nigra pars compacta form five clusters (nigrosomes 1-5 [N1-N5]), and N1 has been considered to be the most affected, followed by N2, N4, N3, and N5 in Parkinson’s disease (PD). Recently, N4 was defined on 3T MRI and found to be involved in late-stage PD compared to N1, suggesting sequential involvement from N1 to N4. We found wider cortical thinning in patients with N4 loss compared to those with N1 loss, similar to the cortical thinning propagation pattern seen with PD progression, which supports the sequential progression hypothesis.
Introduction
The pathological hallmark of Parkinson’s disease (PD) is the progressive degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNc). The dopaminergic neurons within the SNc form five clusters called nigrosomes 1-5 (N1-N5). Among these clusters, N1 is the largest and is considered to be the most affected by PD, followed by N2, N4, N3, and N5.1, 2 Recently, an MRI study reported that N4 loss more frequently occurred in late-stage PD, while N1 loss was more frequently observed in early-stage PD. Moreover, N4 loss always followed N1 loss, suggesting a sequential progression of loss from N1 to N4.3 As cortical thinning is found even in early-stage PD4 and the extent of the involved region widens as PD progresses,5, 6 observing a wider cortical thinning area in patients with N4 loss than in those with N1 loss might support the sequential progression hypothesis. Therefore, we aimed to define whether differential involvement of N1 and N4 may affect the degree of cortical thinning in patients with PD.Methods
A total of 88 PD patients and 40 healthy control subjects underwent high-resolution (0.5 x 0.5 x 1.0 mm3) multi-echo gradient-recalled echo imaging for reconstructing susceptibility map-weighted imaging (SMWI) which was used to assess the N1 or N4 region. All participants also underwent 3-dimensional T1-weighted imaging (1.0 x 1.0 x 1.0 mm3) for cortical thickness analysis. N1 and N4 loss was assessed on each side of the SNc area on SMWI by two independent reviewers. The PD patients were divided into two groups according to the loss of N1 or N4: the N1 group when N1 loss was found on either side, but with the N4 intact on both sides; and the N4 group when N4 loss was found on either side. We used the Automated Anatomical Labeling (AAL) template for the region-of-interest (ROI)-wise cortical thickness analysis. We compared mean cortical thickness extracted from each ROI of the AAL template on each pair of the three groups by ANCOVA with age, sex, and intracranial volume as covariates.Results
Among 88 PD patients, 32 patients showed N1 loss on at least one side (both sides [n=27]; only left side [n=4]; and only right side [n=1]) without N4 loss. Fifty-six patients showed N4 loss on either side (both sides [n=29]; only left side [n=15]; and only right side [n=12]). All patients with N4 loss had bilateral N1 loss with the exception of one patient who had only ipsilateral N1 loss. The N4 and N1 groups were significantly older than the controls. The N4 group included more men and showed higher Hoehn & Yahr scale and UPDRS III scores compared to the controls, without statistical significance (Table).Compared to the controls, the N1 group showed significant cortical thinning in the left orbitofrontal cortex. The cortical thinning area extended to the bilateral superior, left medial, and right middle frontal gyri, bilateral superior and middle, and left inferior temporal gyri, and left lingual gyrus in the N4 group relative to the controls. No significant difference was found in cortical thickness between the N1 and N4 groups (Figure).Discussion
Previous studies have shown either no cortical thinning or cortical thinning limited to the frontal area in early-stage PD,4, 6 with the cortical thinning area spreading to the bilateral medial and lateral prefrontal and temporal cortices in late-stage PD.5, 6 In our study, the N1 group showed cortical thinning only in the left orbitofrontal area, which is commonly associated with olfactory function. As olfactory dysfunction is one of the most frequent prodromal symptoms, cortical thinning in the orbitofrontal area in early-stage PD corresponds to a prioriknowledge. Moreover, the N4 group showed cortical thinning in the bilateral frontal and temporal areas similar to the pattern reported in late-stage PD, supporting the sequential progression hypothesis of loss from N1 to N4 rather than different regional vulnerability.Conclusion
Our results showed wider cortical thinning in patients with N4 loss compared to those with N1 loss. The cortical thinning pattern was similar to the cortical thinning propagation seen with PD progression, supporting the hypothesis of sequential progression of loss from N1 to N4.Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education(NRF-2016R1C1B1009247 and NRF-2014R1A1A2055116).References
1. Damier P, Hirsch EC, Agid Y, Graybiel AM. The substantia nigra of the human brain. I. Nigrosomes and the nigral matrix, a compartmental organization based on calbindin d(28k) immunohistochemistry. Brain. 1999;122 ( Pt 8):1421-14362.
2. Damier P, Hirsch EC, Agid Y, Graybiel AM. The substantia nigra of the human brain. Ii. Patterns of loss of dopamine-containing neurons in parkinson's disease. Brain. 1999;122 ( Pt 8):1437-14483.
3. Sung YH, Lee J, Nam Y, Shin HG, Noh Y, Shin DH, et al. Differential involvement of nigral subregions in idiopathic parkinson's disease. Hum Brain Mapp. 2018;39:542-5534.
4. Uribe C, Segura B, Baggio HC, Abos A, Garcia-Diaz AI, Campabadal A, et al. Cortical atrophy patterns in early parkinson's disease patients using hierarchical cluster analysis. Parkinsonism Relat Disord. 2018;50:3-95.
5. Yau Y, Zeighami Y, Baker TE, Larcher K, Vainik U, Dadar M, et al. Network connectivity determines cortical thinning in early parkinson's disease progression. Nat Commun. 2018;9:126.
6. Zarei M, Ibarretxe-Bilbao N, Compta Y, Hough M, Junque C, Bargallo N, et al. Cortical thinning is associated with disease stages and dementia in parkinson's disease.J Neurol Neurosurg Psychiatry. 2013;84:875-881
Figures
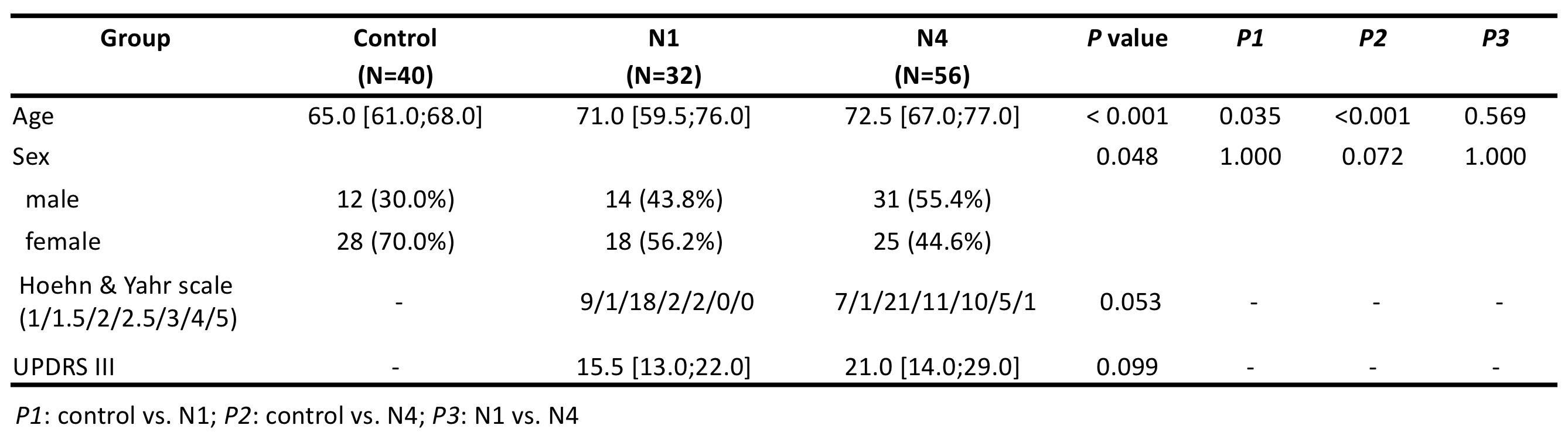
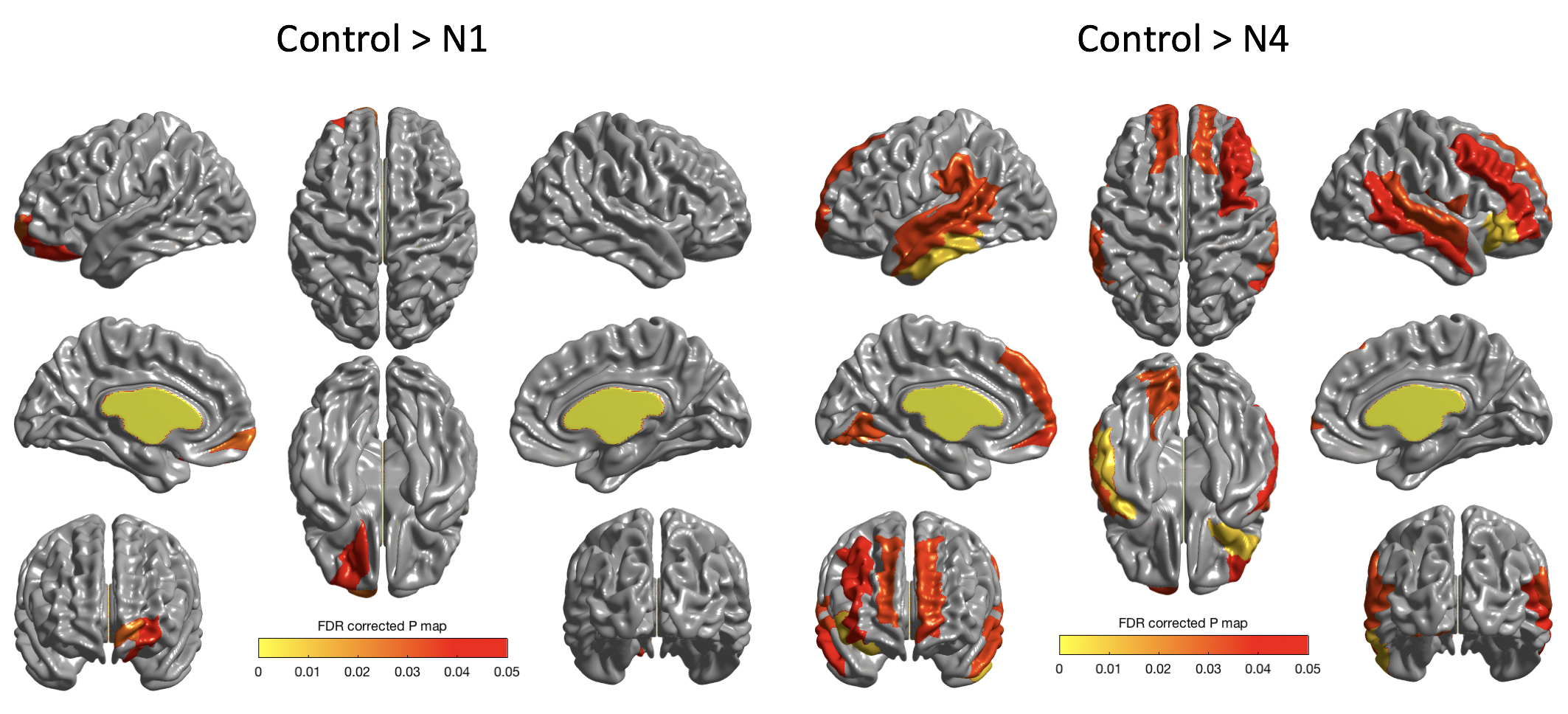
Figure. Cortical thinning in the PD patients with the loss of nigrosome 1 (left) and nigrosome 4 (right) compared to the controls