2561
Correlation between internal carotid artery flow and circle of Willis anatomy1Department of Radiology, Chi-Mei Medical Center, Tainan, Taiwan, 22. Department of Radiology, E-DA Hospital, I-Shou University, Kaohsiung, Taiwan
Synopsis
Measurement of proximal cerebral inflow volume and individual cerebral angio-architecture are crucial for patient-specific analysis of hemodynamic effects of cerebrovascular disease. However, the detail of bilateral ICA flow in individuals of complete but asymmetric COW is lacking. This retrospective study included total 210 healthy adult for delineation of the relationship between detailed COW variations and bilateral ICA flow volume in healthy adults. Furthermore, the correlation of ICA diameter to ICA flow in the setting of circle of Willis variants was also proposed.
Introduction: Measurement of proximal cerebral inflow volume and individual cerebral angio-architecture are crucial for patient-specific analysis of hemodynamic effects of cerebrovascular disease. It is well known that both anterior communicating artery(Acom) and posterior communicating artery(Pcom) aneurysms are found to be more often associated with incomplete circle of Willis(COW), such as Acom aneurysm in case of A1 aplasia and PcomA aneurysms in case of fetal-origin posterior cerebral artery(PCA). On the other hand, several studies1-3 focused on blood flow distribution in the COW variants had showed increased ipsilateral internal carotid artery(ICA) flow with dominant A1 or fetal-type PCA. However, the detail of bilateral ICA flow in individuals of complete but asymmetric COW is lacking. This retrospective study will focus on the relationship between detailed COW variations and bilateral ICA flow volume in healthy adults.
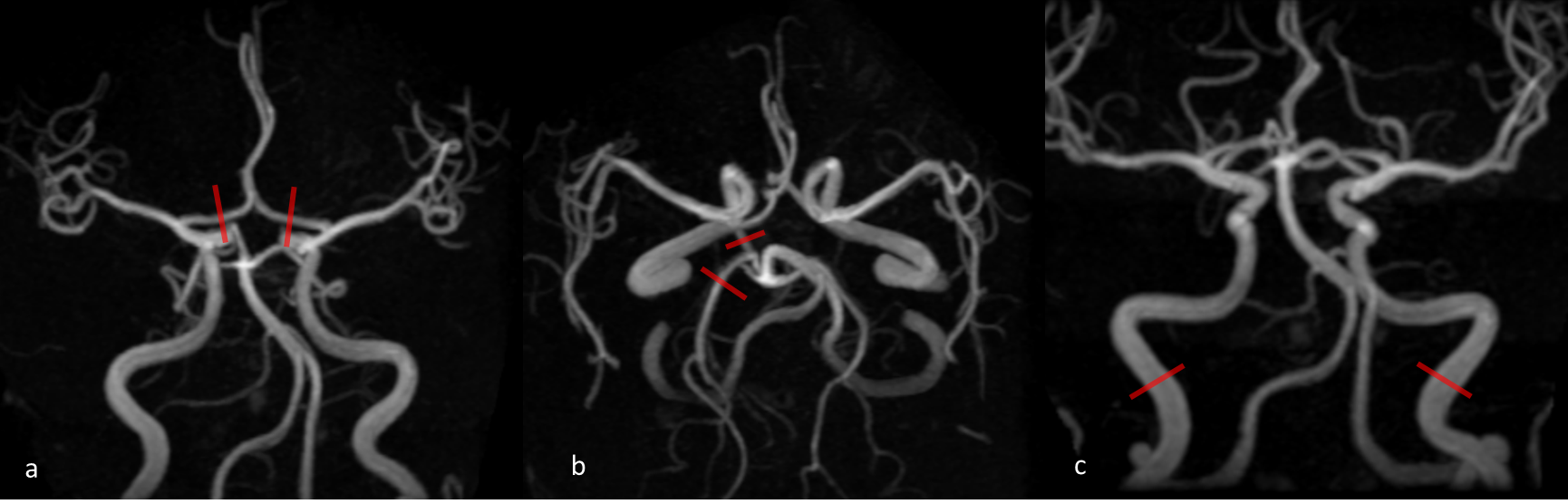
Methods: This retrospective study was approved by the Institutional Review Board of our institution(Chi-Mei Medical Center, Tainan, Taiwan). The requirement to obtain informed consent was waived due to its retrospective nature. We retrospectively review Picture Archiving and Communication System(PACS) of our institution from January, 2017 to June, 2018 to enroll 223 cases, receiving simultaneous examinations of head & neck MR angiography and carotid duplex within one week duration for the purpose of self-pay imaging health examination. The major extracranial arteries in the neck were first visualized by contrast-enhancing MRA on a 3T Discovery MR 750 (GE Medical system, Milwaukee, Wis) using Gadobutrol (Gd-BT-DO3A, Gadovist™, Bayer Healthcare, Leverkusen, Germany) with MR parameters including TR/TE, 4/1 millisecond; flip angle, 25°; FOV, 300 mm; matrix, 320/224; NEX, 1. Then, a three-dimensional MRA TOF of the head was obtained with parameters: TR/TE, 21/2 millisecond; flip angle, 20°; FOV, 200 mm; matrix, 320x192; Nex, 1. Carotid Doppler was performed on a Philips HD15 ultrasound system and reviewed for bilateral ICA flow volume collection. The exclusion criteria include segmental narrowing(>50%) of common/ internal carotid arteries(three case), proximal ACA/ middle cerebral artery(MCA; four cases) and vertebral/ basilar artery, persistent carotid-vertebrobasilar anastomoses, such as persistent trigeminal artery(one case), vascular anomaly such as cerebral aneurysm(two cases), arteriovenous malformation/ fistula(two cases), moyamoya syndrome(one case), ever craniotomy/ craniectomy and ever intracranial hemorrhage/ stroke, except lacunar infarcts. Finally, total 210 cases were included in this study. For COW classification, the diameter of bilateral A1 segments, Pcom and P2 segments of each case were record as index case of figure 1a and 1b. The diameter of bilateral distal cervical ICAs were measured at one centimeter below the petrous segment of ICA. According to the diameter ratio difference of bilateral A1 segments, three anterior cerebral artery asymmetry(AA) groups were defined as AA1 group(19 cases; 9%) with one-side A1 aplasia; AA2 group(33 cases; 15.7%) with bilateral A1 ratio difference >0.5 and AA3 group(15 cases; 7.1%) with bilateral A1 ratio difference <0.5. Similarly, bilateral Pcom diameter ratios were referred to the ipsilateral P2 segment diameter. Three Pcom asymmetry(PA) groups were defined as PA1 group(15 cases; 7.1%) with one fetal-origin PCA and absent Pcom on the contralateral side; PA2 group(45 cases; 21.4%) with bilateral Pcom diameter ratio> 0.5 and PA3 group(18 cases; 8.6%) with bilateral PcomA diameter ratio <0.5. The symmetric group(88 cases; 41.9%) was defined as no diameter ratio difference in bilateral A1 and bilateral Pcom.
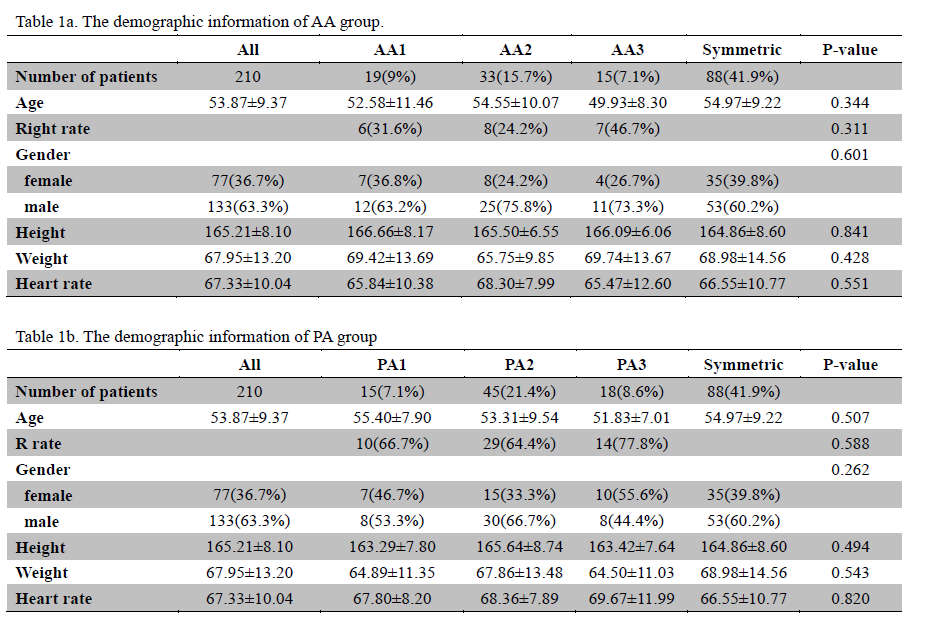
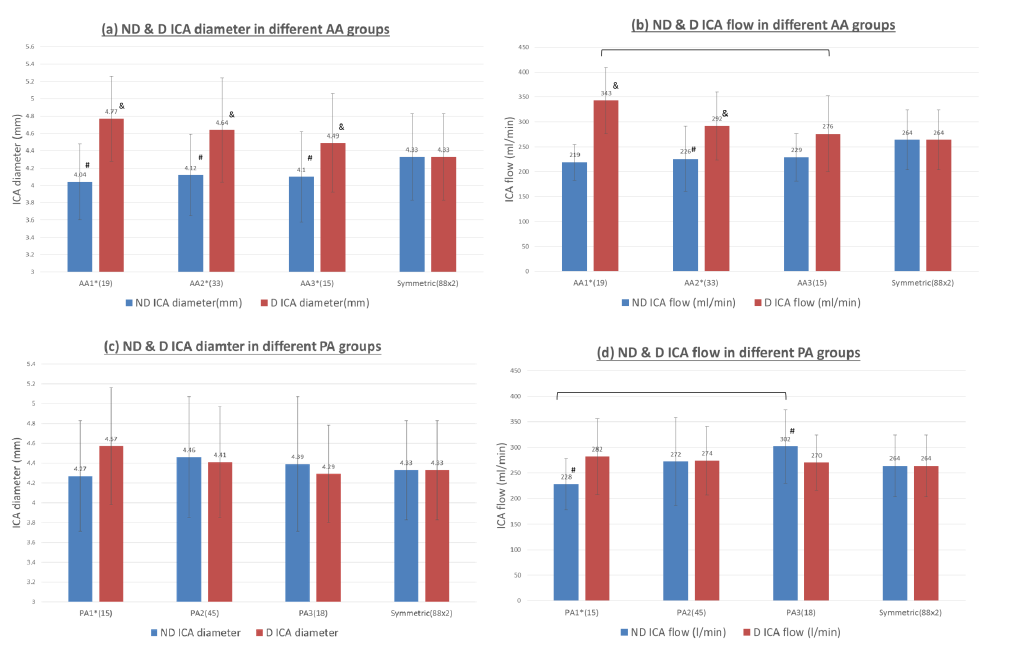
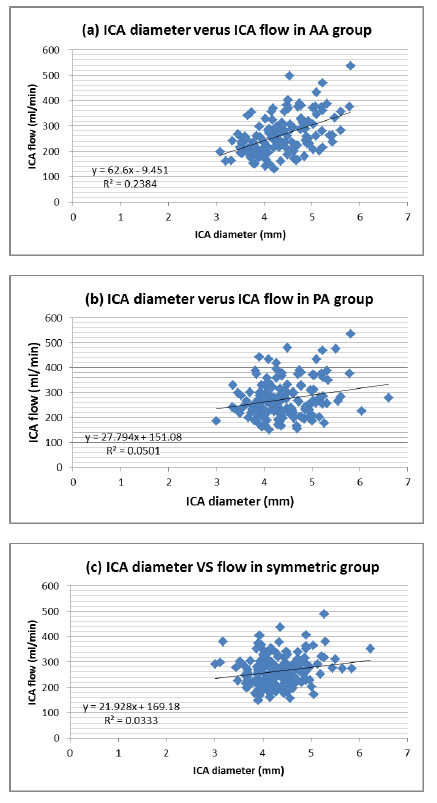
Results: The demographic information of all patients, symmetric group and each AA, PA groups were listed in Table 1a and 1b. There is no significant difference of baseline information between each groups. While anterior cerebral artery asymmetry is present, there are significant differences of ICA diameter between dominant and non-dominant sides in each AA1, AA2 and AA3 group(Fig 2a). As compared with symmetric group, the ICA diameter with dominant ACA is significantly larger and the ICA diameter on the non-dominant ACA side is significant smaller in each AA1, AA2 and AA3 group. Similarly, significant differences of bilateral ICA flows were also found in AA1 and AA2 groups(Fig 2b). More asymmetric between bilateral ACA, higher ICA low on the dominant side. As for PA group, bilateral ICA diameter and flow difference was only found in PA1 group(Fig 2c and 2d). The ICA flow on the non-dominant side rather than on the dominant side changes significantly in PA1 and PA3 groups as compared with the symmetric group. Following linear regression analysis of ICA diameter and flow, there is mild positive correlation between ICA diameter and ICA flow in the all AA groups.
Conclusion: ACA asymmetry plays an important role on ICA flow distribution. On the other hand, only fetal-origin PCA change ICA flow distribution significantly.
Acknowledgements
No acknowledgement found.References
- Hendrikse J, van Raamt AF, van der Graaf Y, et al. Distribution of Cerebral Blood Flow in the Circle of Willis. Radiology 2005;235:184-189.
- Tanaka H, Fujita N, Enoki T, et al. Relationship between variations in the circle of Willis and flow rates in internal carotid and basilar arteries determined by means of magnetic resonance imaging with semiautomated lumen segmentation: reference data from 125 healthy volunteers. AJNR 2006;27(8): 1770-1775.
- Amin-Hanjani S, Du X, Pandey DK et al. Effect of age and vascular anatomy on blood flow in major cerebral vessels. Journal of cerebral blood flow & metabolism 2015;35: 312-318
Figures