2536
Neurometabolic consequences of perinatal HIV infection and exposure are still observed in children at 11 years1Department of Human Biology, University of Cape Town, Cape Town, South Africa, 2Department of Statistical Sciences, University of Cape Town, Cape Town, South Africa, 3Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa, 4A.A. Martinos Centre for Biomedical Imaging, Massachusetts General Hospital, Boston, MA, United States, 5Department of Radiology, Harvard Medical School, Boston, MA, United States, 6Cape Universities Body Imaging Center, University of Cape Town, Groote Schuur Hospital, Cape Town, South Africa
Synopsis
HIV establishes reservoirs within the brain, causing damage despite individuals adhering to antiretroviral therapy. The long-term consequences of perinatal HIV infection and early treatment in children remain unclear. Proton magnetic resonance spectroscopy was carried out to assess the effects of HIV on neurodevelopment, at a metabolic level, comparing HIV-positive, HIV-exposed-uninfected (HEU) and HIV-unexposed children at 11 years old. Absolute metabolite concentrations were compared between these groups, through linear regression analysis. Elevated choline levels within two regions of interest suggest putative inflammation in HIV-positive children. A reduction of N-acetyl-acetate in a white-matter region of HIV-positive and HEU children implies axonal damage.
Introduction
In spite of seropositive individuals adhering correctly to treatment plans, harmful effects of HIV are still observed in the brain.1 Early treatment of perinatally HIV-infected infants is vital for reducing child mortality rates.2 However, the long-term effects of HIV and antiretroviral therapy (ART) are unclear for perinatally exposed and infected children.
Proton magnetic resonance spectroscopy (1H-MRS) contributes a key link between alterations to the immune system, neurological structures and cognition, that occur with HIV infection.3,4 More subtle effects of HIV can be detected at a chemical level.5 At younger ages, metabolic changes have been noted within the basal ganglia and midfrontal gray matter regions of the brain, in children from the children with HIV early antiretroviral therapy (CHER) trial enrolled into this study.2,4,6 In this project we are interested in neurometabolic activity in children at 11 years, as they enter adolescence, a period where hormonal and structural changes are enhanced. 7,8
Methods
A total of 127 children at the age of 11 years (11.60 ± 0.25), from the CHER trial, 2 participated in this study. Scanning was performed with a 3T Siemens Skyra scanner (Siemens, Erlangen Germany) at the Cape Universities Body Imaging Centre, Cape Town. Structural scans and single-voxel 1H-MRS were carried out, utilizing a point resolved spectroscopy (PRESS) sequence (64 averages, TR = 2000 ms, TE = 30ms, spectral bandwidth = 1500Hz, voxel size = 1.5x1.5x1.5 cm3) with CHESS water suppression 6 to obtain spectra in the basal ganglia (BG), midfrontal gray matter (MFGM) and peritrigonal white matter (PWM) regions. Segmentation and spectral quantitation via the water-scaling method were performed using Statistical Parametric mapping (SPM12) software and LCModel (version 6.3-1) 9,10 respectively, yielding absolute metabolite concentrations and ratios to creatine.
Linear regression models were generated in R, 11 to compare metabolite concentrations in 75 HIV-positive and 24 HIV-exposed-uninfected (HEU) children, to 28 HIV-unexposed (HU) control children. Confounders included the proportion of gray/white matter content, age at the time of scan, sex and ethnicity. The metabolites investigated were total choline (glycerophoshocholine + phosphocholine), total creatine (creatine + phosphocreatine), total N-acetyl aspartate (NAA+NAAG), glutamate and myo-inositol.
Results
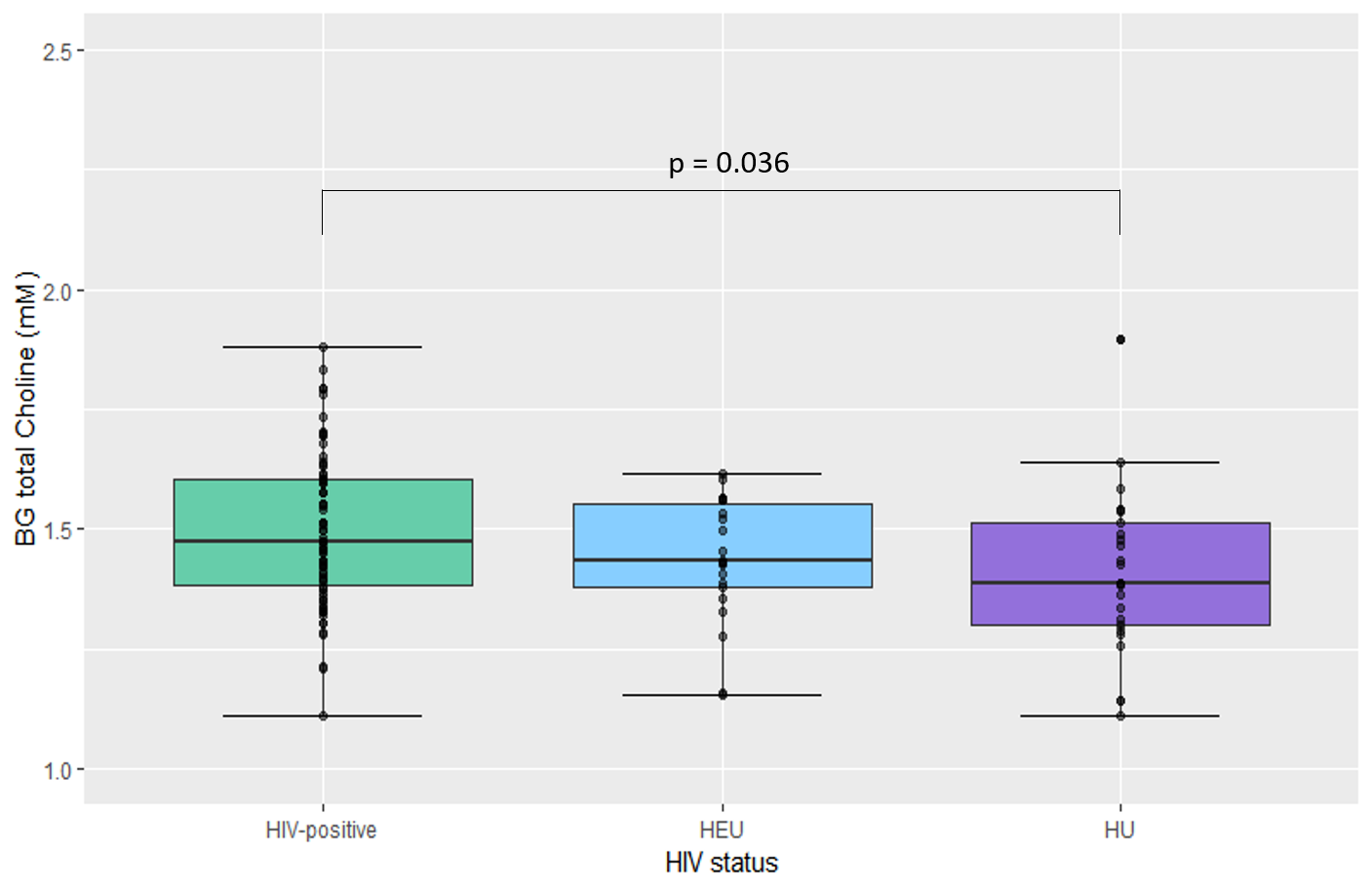
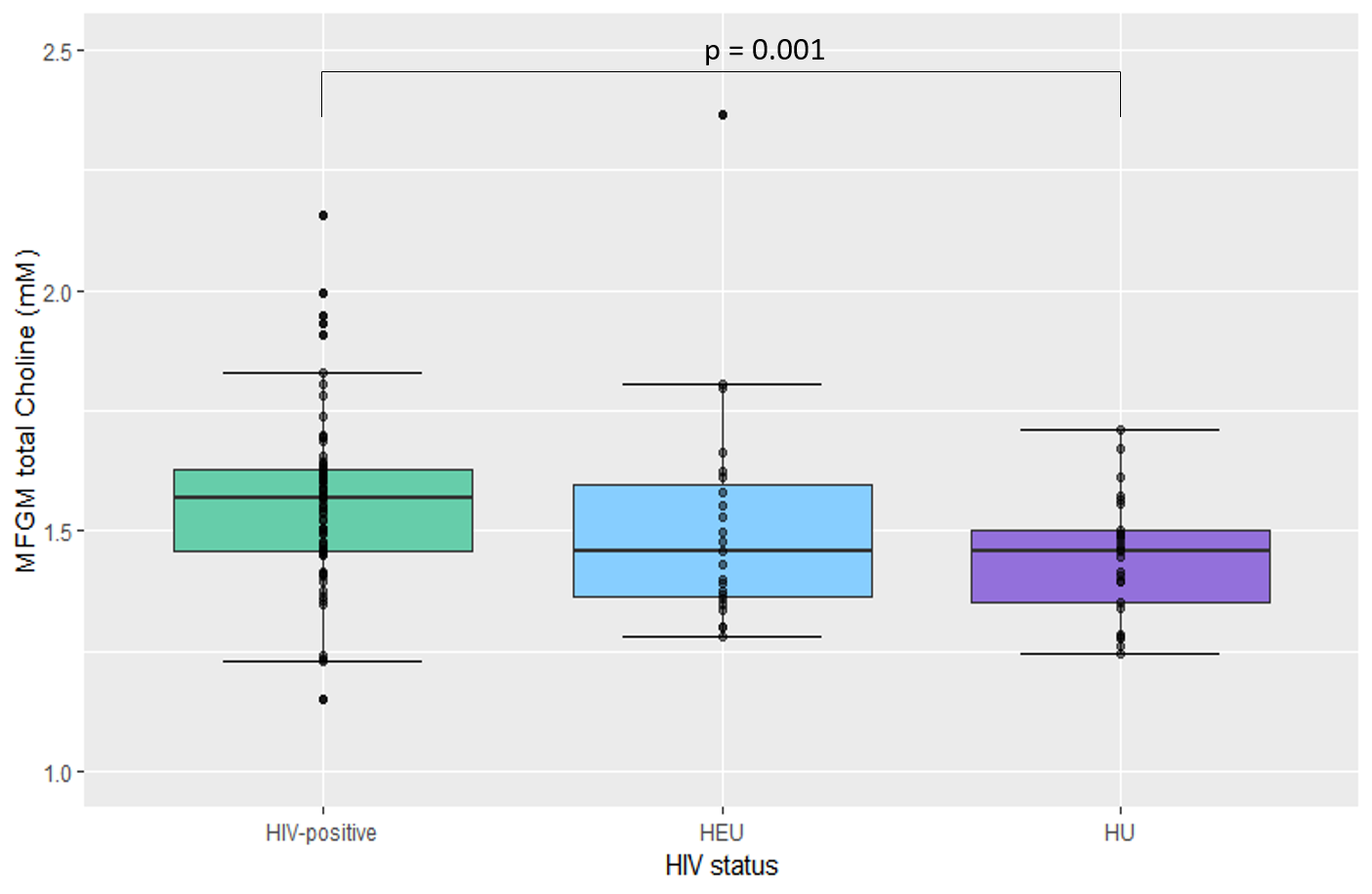
An elevation in total choline levels is observed in the BG (β= 0.075, se= 0.035, p= 0.036) and MFGM (β= 0.141, se= 0.040, p= 0.001) of HIV-positive children in comparison to HU controls at the age of 11 years (figure 1 and 2). The metabolic activity in these regions does not differ significantly between HEU and HU children.
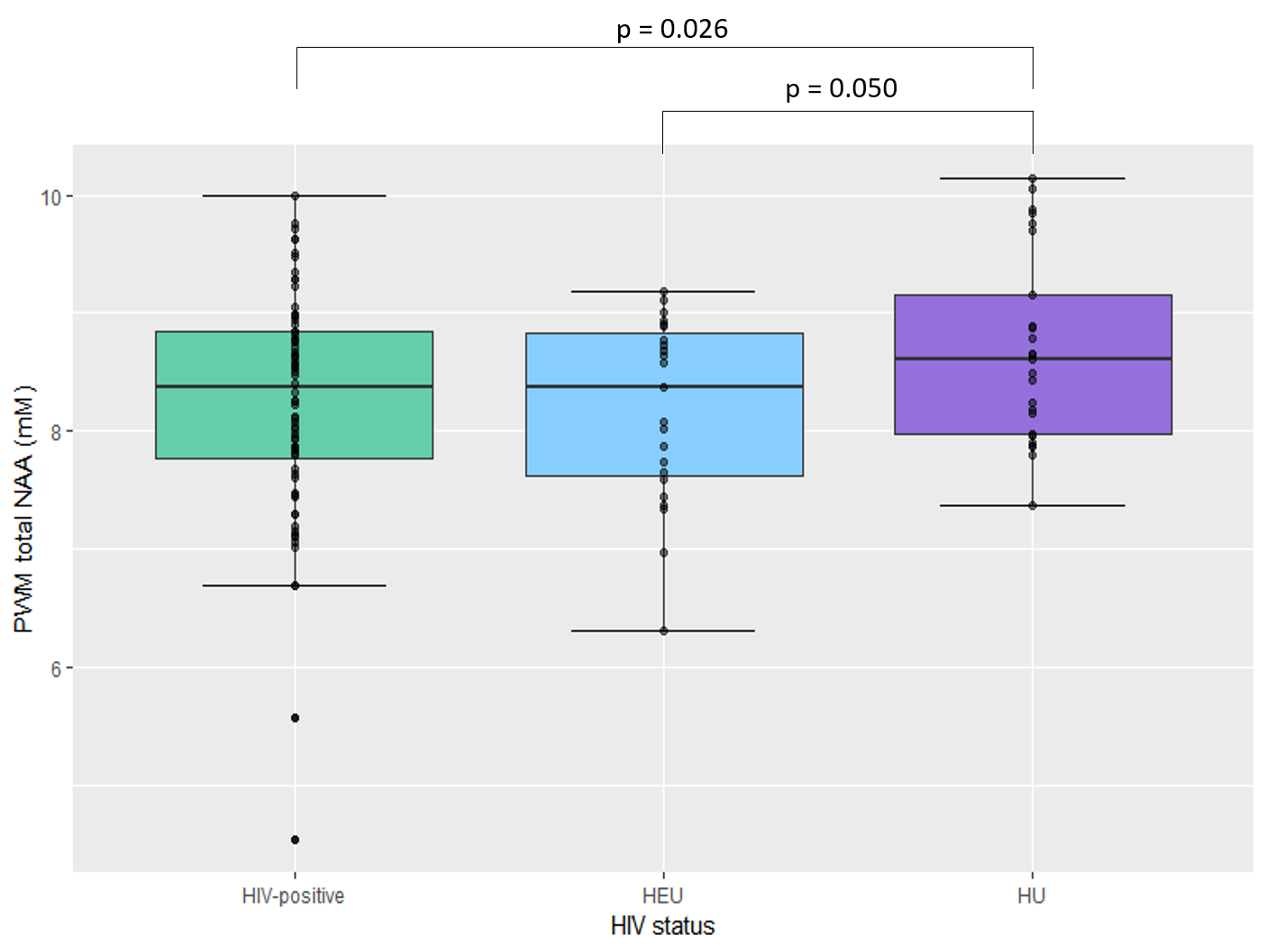
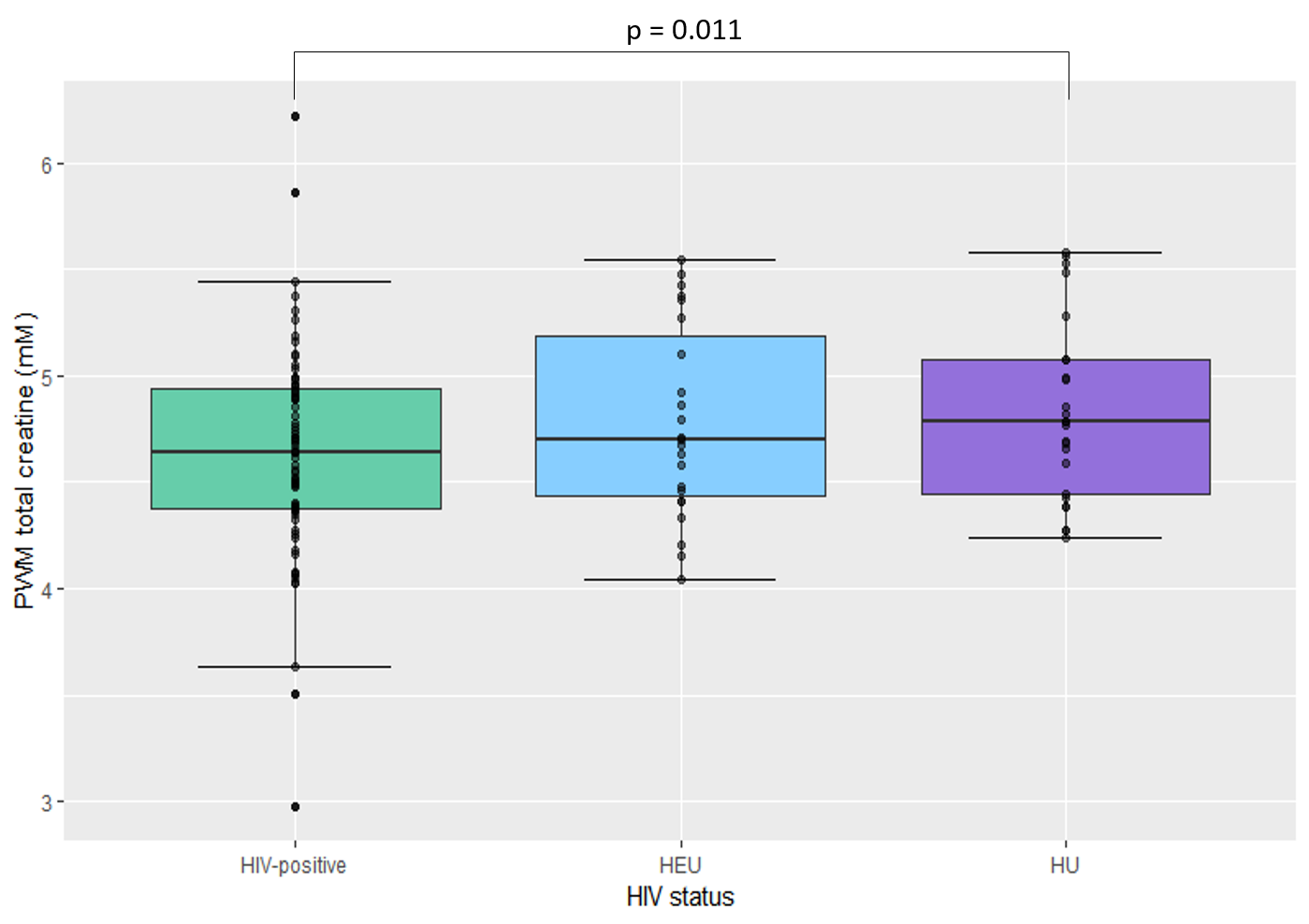
By 11 years, significant reductions in total NAA (β= - 0.431, se= 0.192, p= 0.026) and total creatine (β= - 0.211, se= 0.081, p= 0.011) concentrations are seen in the PWM of HIV-positive children compared to HU children (figure 3 and 4). HEU children have lower total NAA levels (β= - 0.494, se= 0.249, p= 0.050) compared to HU children in this region.
The results in the BG and MFGM are further confirmed by analysis of the ratios of the metabolites to creatine, revealing elevated total choline:creatine. In the PWM, significantly higher total choline:creatine levels are also noted in HIV-positive children compared to HU children (β= 0.017, se= 0.008, p= 0.033), while total NAA:creatine levels do not differ according to HIV status.
Discussion and conclusions
Although the effects of perinatal HIV infection and early ART cannot be distinguished in this study, their combined influence on neurometabolic development can be observed in 11-year-old children. Elevated choline levels in the BG and MFGM of HIV-positive children at 11 years suggest that inflammation may occur in these regions despite early treatment of HIV infection.
The effects of HIV/ART exposure are only observed in the PWM at 11 years, with lower NAA levels in HEU and HIV-positive children indicating possible axonal damage or reduced axonal density in this region. A reduction in total creatine in the PWM of HIV-positive children in comparison to controls, firstly suggests a decline in energy metabolism, and secondly reveals that creatine may not be a valid internal reference in studies assessing the effects of HIV on the brain, as is common practice in MRS studies. Altered creatine levels between HIV status groups provide an explanation for the different findings when analysing absolute and creatine-relative concentrations in the PWM.
The metabolic changes found to occur in the BG, MFGM and PWM may, in future, be linked to structural and functional changes which are observed in these children. This work is part of a longitudinal study from 5-11 years, which ultimately will provide a reference set of neurometabolic profiles specific to HIV-positive and HEU children in South Africa.
Acknowledgements
Funding provided by the NRF/DST South African Research Chairs Initiative; NRF grant CPR20110614000019421; South African Medical Research Council (SAMRC); US National Institute of Allergy and Infectious Diseases (NIAID) (CIPRA network, Grant U19 AI53217); NIH grants (R01HD071664, R01HD093578, R21MH096559 and R21MH108346). Our thanks to the radiographers at CUBIC, UCT, Petronella Samuels, Ingrid Op’t Hof and Mazwi Maishi, and to Research staff Thandiwe Hamana.
References
1. Robertson KR, Smurzynski M, Parsons TD, Wu K, Bosch RJ, Wu J, McArthur JC, Collier AC, Evans SR, Ellis RJ (2007) The prevalence and incidence of neurocognitive impairment in the HAART era. AIDS.
2. Violari A, Cotton MF, Gibb DM, Babiker AG, Steyn J, Madhi SA, Jean-Philippe P, McIntyre JA (2008) Early antiretroviral therapy and mortality among HIV-infected infants. N Engl J Med.
3. Van Dalen YW, Blokhuis C, Cohen S, Ter Stege JA, Teunissen CE, Kuhle J, Kootstra NA, Scherpbier HJ, Kuijpers TW, Reiss P (2016) Neurometabolite alterations associated with cognitive performance in perinatally HIV-infected children. Medicine.
4. Mbugua K, Holmes M, Cotton M, Ratai E, Little F, Hess A, Dobbels E, Van der Kouwe A, Laughton B, Meintjes E (2016) HIV-associated CD4+/CD8+ depletion in infancy is associated with neurometabolic reductions in the basal ganglia at age 5 years despite early antiretroviral therapy. AIDS.
5. Wilkinson ID, Lunn S, Miszkiel KA, Miller RF, Paley MN, Williams I, Chinn RJ, Hall-Craggs MA, Newman SP, Kendall BE (1997) Proton MRS and quantitative MRI assessment of the short term neurological response to antiretroviral therapy in AIDS. Journal of Neurology, Neurosurgery & Psychiatry.
6. Robertson FC, Holmes MJ, Cotton MF, Dobbels E, Little F, Laughton B, Van Der Kouwe, André JW, Meintjes EM (2018) Perinatal HIV Infection or Exposure is Associated with Low N-acetylaspartate and Glutamate in Basal Ganglia at age 9 but not 7 Years. Frontiers in Human Neuroscience.
7. Giedd, Jay N. "Structural Magnetic Resonance Imaging of the Adolescent Brain." Annals of the new York Academy of Sciences, vol. 1021, no. 1, 2004, pp. 77-85.
8. Sisk, Cheryl L., and Julia L. Zehr. "Pubertal Hormones Organize the Adolescent Brain and Behavior." Frontiers in Neuroendocrinology, vol. 26, no. 3-4, 2005, pp. 163-174.
9. Ernst, T., Kreis, R. & Ross, B.D. 1993. Absolute quantitation of water and metabolites in the human brain. I. Compartments and water. Journal of Magnetic Resonance, Series B. 102(1):1-8.
10. Provencher, S.W. 2001. Automatic quantitation of localized in vivo 1H spectra with LCModel. NMR in Biomedicine. 14(4):260-264. 11. R Core Team (2018) R: A Language and Environment for Statistical Computing. In: https://www.R-project.org
Figures