2534
Metabolic Markers of Disease Progression in Pediatric Diffuse Intrinsic Pontine Gliomas1Radiology, Children's Hospital Los Angeles/USC, Los Angeles, CA, United States, 2Rudi Schulte Research Institute, Santa Barbara, CA, United States, 3Biostatistics, UPMC Children's Hopital of Pittsburgh, Pittsburgh, PA, United States, 4Radiology, UPMC Children's Hopital of Pittsburgh, Pittsburgh, PA, United States, 5Neurosurgery, UPMC Children's Hopital of Pittsburgh, Pittsburgh, PA, United States
Synopsis
Diffuse intrinsic pontine gliomas (DIPG) are inoperable and highly resistant to chemo- and radiation therapy. DIPG carry the worst prognosis among pediatric brain tumors with progress in the development of therapies compromised by low patient numbers and unavailability of tissue samples to characterize disease status. In this work we present evidence, that non-invasive MR spectroscopy can provide robust early indicators that can assess the effectiveness (or ineffectiveness) of potential new therapeutic approach at an early stage and accelerate the completion of clinical trials in small cohorts of patients.
Introduction
Diffuse intrinsic pontine glioma (DIPG) carry the worst prognoses in pediatric neurooncology, with no substantial improvement in outcomes for decades. There is nevertheless clinically significant heterogeneity in outcomes with some patients only surviving a few months after diagnosis whereas other patients may survive up to a few years. The goal of this study was to identify in vivo metabolic markers that distinguish between these subgroups at different stages of the disease course.Methods
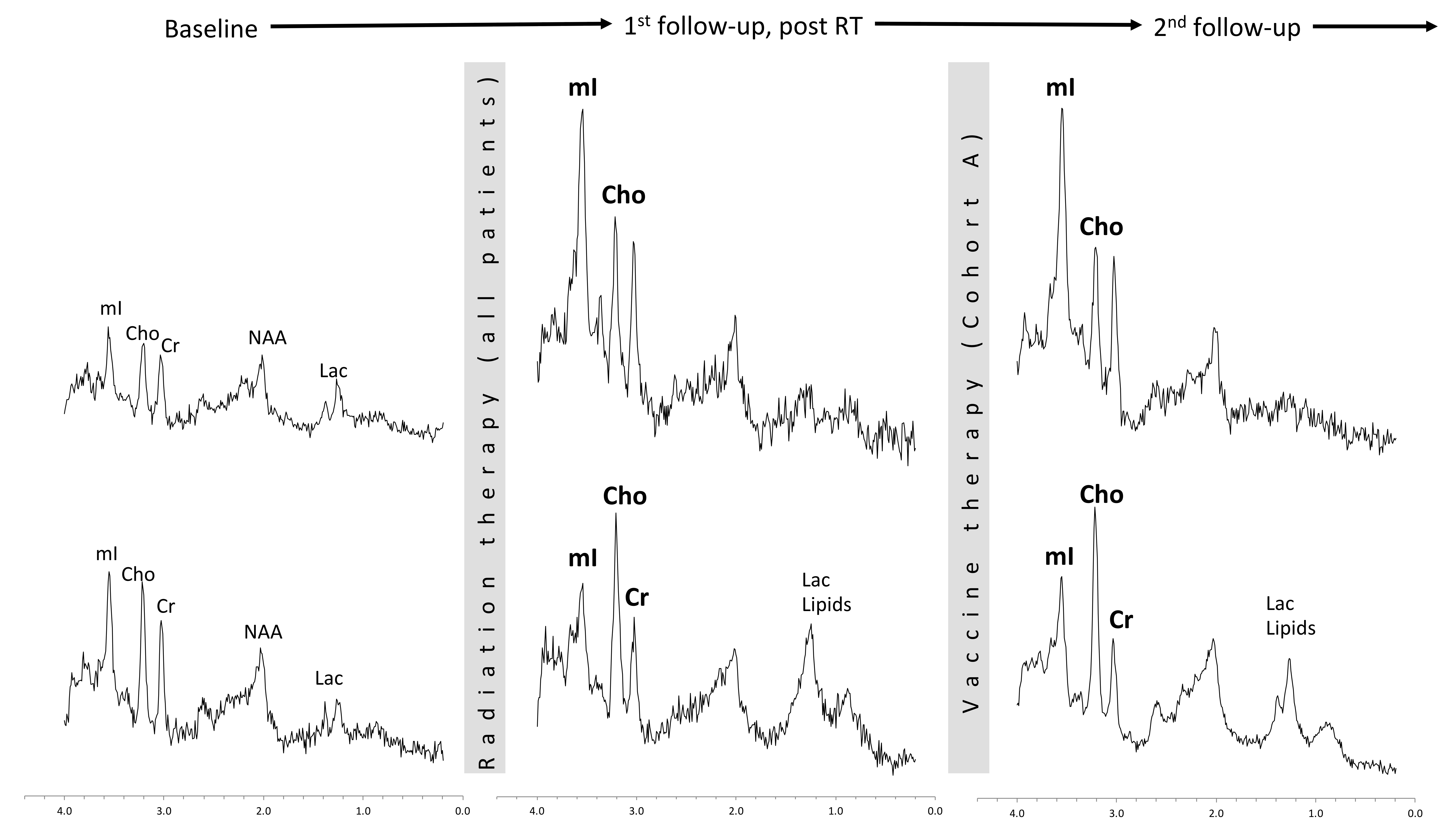
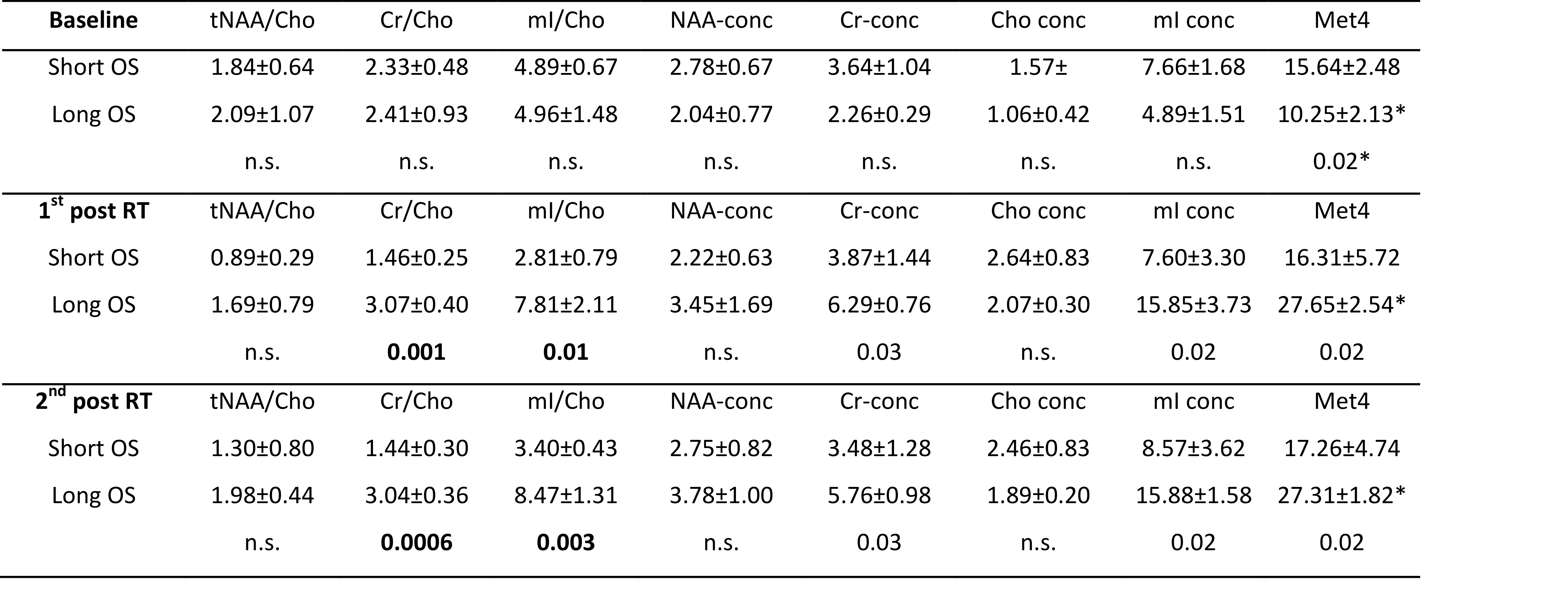
MRS studies from 47 DIPG patients were reviewed for this analysis. Patients were recruited from two sites. 14 patients were enrolled in a highly standardized phase 1 clinical trial of peptide-based vaccine therapy (VT) at the first site (cohort A). In addition, data from 33 patients that were treated with various not-standardized radio-chemotherapies from the second site (cohort B) were analyzed. Initial review indicated comparable trends for both cohorts and all data were thus pooled. Metabolic profiles were binned into clinically equivalent time points and sorted by the length of survival after initial diagnosis. To have an unambigous clear separation of clinical course, MR spectra of four patients with the shortest survival and four patients with the longest survival were compared at initial diagnosis and at the first and second follow-up after radiation therapy (RT) (Tab. 1). All spectra were acquired using a single-voxel PRESS sequence (TE = 35ms, TR = 1.5s, 128 averages, acquisition time: 4min) integrated with routine pre/post contrast MR imaging and performed on 1.5T MR systems (Signa LX, GE Healthcare, Milwaukee, Wisconsin). Spectra were processed with fully automated LCModel (version 6.3-1l) software. Concentrations of the main metabolites N-acetylaspartate (NAA), creatine (Cr), choline (Cho), myo-inositol (mI) and metabolite ratios relative to Cho, as well as lactate (Lac) and lipids (Lip) were evaluated. Student’s t-test was used for statistical tests.Results
At diagnosis, DIPG patients with short survival (< 9 months) presented with generally higher absolute metabolite concentrations than long survivors (>18 months), whereas there was no difference of relative concentrations. At first follow-up after completion of therapy, metabolite levels of longer survivors had increased to the same levels or both those seen in short survivors. The ratios of Cr/Cho and mI/Cho were significant different between these two groups with no overlap. This pattern was confirmed at the second follow-up (Fig. 1, Tab.1).
Discussion
Albeit DIPG are considered to have a particular poor prognosis, there are clinically significant differences in survival in individual patients. Early identification and stratification of patients at high risk for early relapse or of patients that are expected to do better would have a significant positive impact on patient management and quality of life. Since biopsies are usually not obtained, non-invasive imaging is required to potentially provide this information. At diagnosis metabolite profiles were comparable, apart from generally high metabolite levels in the subgroup with particularly poor outcome. However, already at the first follow-up study after completion of RT, typically 2-3 months after diagnosis, striking metabolic differences for these two subgroups were observed. The changes from baseline in short survivors (decreasing mI/Cho and Cr/Cho) were consistent with malignant progression (1,2). In addition, MRS at initial follow-up exams could provide early endpoints for clinical trials and thus accelerate clinical research. It appears unlikely that MRS or other advanced non-invasive methods can be used to evaluate treatment options that offer marginal improvement over current therapies. On the other hand, a “game-changing” therapeutic approach could be recognized in a small patient cohort.Conclusions
MRS profiles can be used to stratify DIPG patients at the extremes of clinical outcomes early in the disease course. MRS to monitor treatments could accelerate clinical research considerably.Acknowledgements
Ian's Friends FoundationReferences
1. Panigrahy A, Nelson MD, Jr., Finlay JL, et al. Metabolism of diffuse intrinsic brainstem gliomas in children. Neuro Oncol. 2008; 10(1):32-44.9.
2. Laprie A, Pirzkall A, Haas-Kogan DA, et al. Longitudinal multivoxel MR spectroscopy study of pediatric diffuse brainstem gliomas treated with radiotherapy. Int J Radiat Oncol Biol Phys. 2005; 62(1):20-31.
3. Chen HJ, Panigrahy A, Dhall G, Finlay JL, Nelson MD, Blüml S. Apparent diffusion and fractional anisotropy of diffuse intrinsic brain stem gliomas. AJNR Am J Neuroradiol. 2010; 31(10):1879-1885.
Figures