2504
Human cardiac pH and Pi concentration during dobutamine stress measured by 7T 31P-MRS1Center for Medical Physics and Biomedical Engineering, Medical University of Vienna, Vienna, Austria, 2Oxford Centre for Clinical Magnetic Resonance Research (OCMR), University of Oxford, Oxford, United Kingdom, 3Department of Imaging Methods, Institute of Measurement Science, Slovak Academy of Sciences, Bratislava, Slovakia, 4Wellcome Centre for Integrative Neuroimaging, FMRIB, University of Oxford, Oxford, United Kingdom, 5The Wolfson Brain Imaging Centre, University of Cambridge, Cambridge, United Kingdom
Synopsis
The hydrolysis of adenosine triphosphate (ATP) to adenosine diphosphate (ADP) in the reaction ATP + H20 ⇌ ADP + Pi (inorganic phosphate) is used to drive all cellular processes, including those involved in ventricular contraction and relaxation. When spectral quality is sufficient to quantify the Pi peak, it is possible to assess the ratio of Pi to phosphocreatine (Pi/PCr), which is an established measure of the muscle control of energy production. It is also possible to assess cardiac intracellular pH from the Pi to PCr frequency offset. Most human cardiac 31P-MRS studies report only the PCr/ATP ratio, and are typically unable to quantify cardiac Pi because of partially overlapping resonances from 2,3-diphosphoglycerate in blood. We aimed to use ultra-high (7T) field strength and a novel 31P STEAM sequence to 1) non-invasively measure myocardial Pi/PCr and pH at rest and 2) for the first time record these parameters during catecholamine stress.
Introduction
The hydrolysis of adenosine triphosphate (ATP) to adenosine diphosphate (ADP) in the reaction ATP + H20 ⇌ ADP + Pi (inorganic phosphate) is used to drive all cellular processes, including those involved in ventricular contraction and relaxation. When spectral quality is sufficient to quantify the Pi peak, it is possible to assess the ratio of Pi to phosphocreatine (Pi/PCr), which is an established measure of the muscle control of energy production.
It is also possible to assess cardiac intracellular pH from the Pi to PCr frequency offset. Most human cardiac 31P-MRS studies report only the PCr/ATP ratio, and are typically unable to quantify cardiac Pi because of partially overlapping resonances from 2,3-diphosphoglycerate in blood. We aimed to use ultra-high (7T) field strength and a novel 31P STEAM sequence to 1) non-invasively measure myocardial Pi/PCr and pH at rest and 2) for the first time record these parameters during catecholamine stress.
Methods
18 healthy volunteers (6 female, age 37±16, BMI 23.70±2.09 kg/m2) were recruited to the study in compliance with local regulations. All scans were performed using a 10cm 1H loop for localisers (Rapid Biomedical, Germany) and a 16-channel 31P array (RAPID Biomedical, Germany) for 31P-MRS [1. 2].
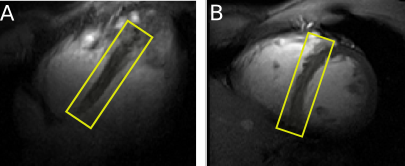
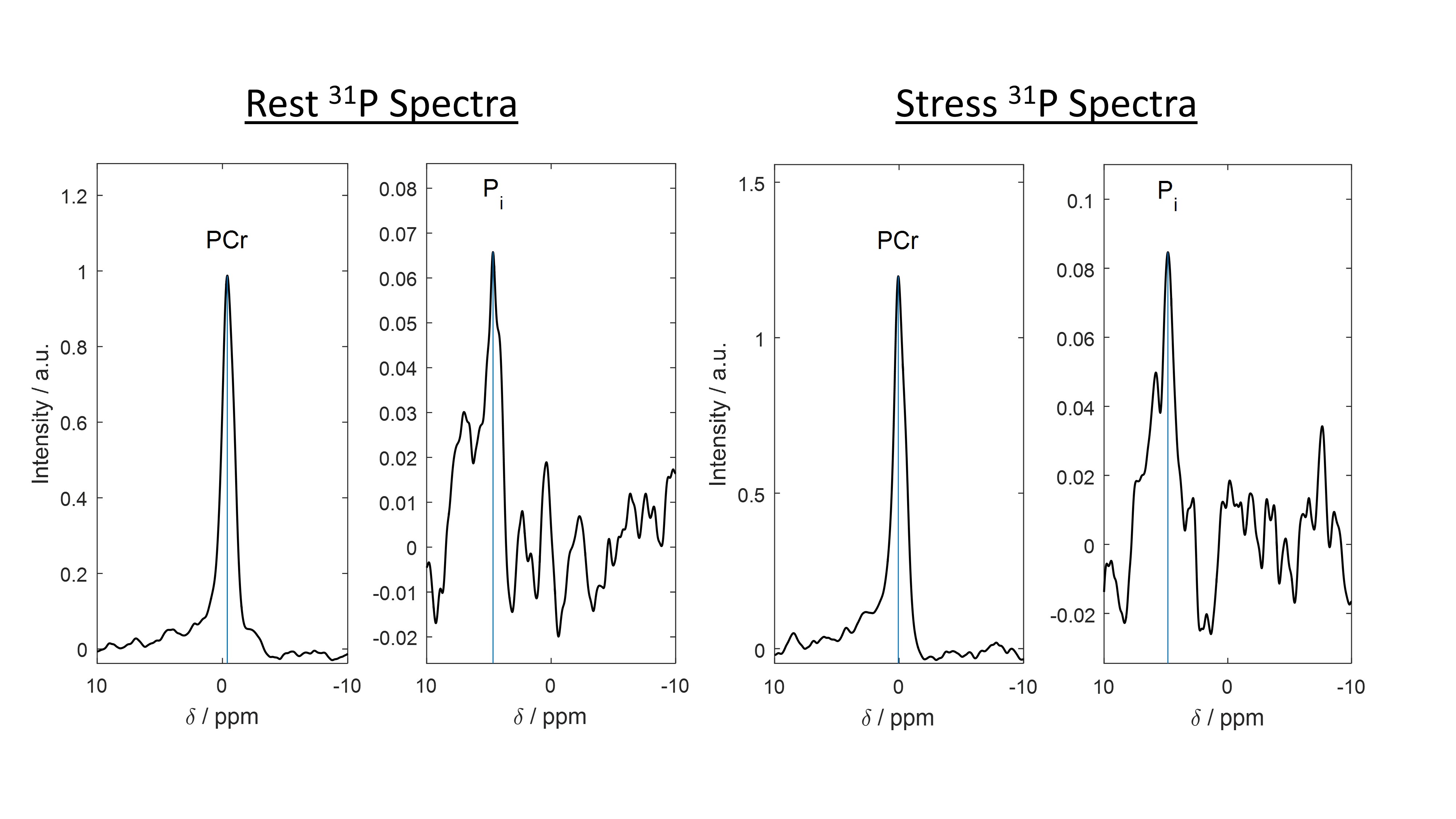
Free-breathing, ECG-triggered data were acquired from the septum (Figure 1) at rest using an interleaved STEAM sequence with even excitations centred at PCr (0ppm) and odd excitations at Pi (4.8ppm), TE=13ms, TM = 7/60ms, TR~7s, 128 averages each. Data were acquired before and during dobutamine infusion (n=14, targeting 65% maximum heart rate, Figure 2). Continuous blood pressure and heart rate measurements (Skidmore Medicals, UK) were undertaken. The OXSA MATLAB toolbox was used to process and fit spectra, using prior knowledge of the expected shifts for each metabolite [3].
PCr/ATP were measured using a acquisition weighted UTE-CSI scan (8 x 16 x 6, FOV 200x200x200mm, 14min scan time) before the STEAM sequence.
Results
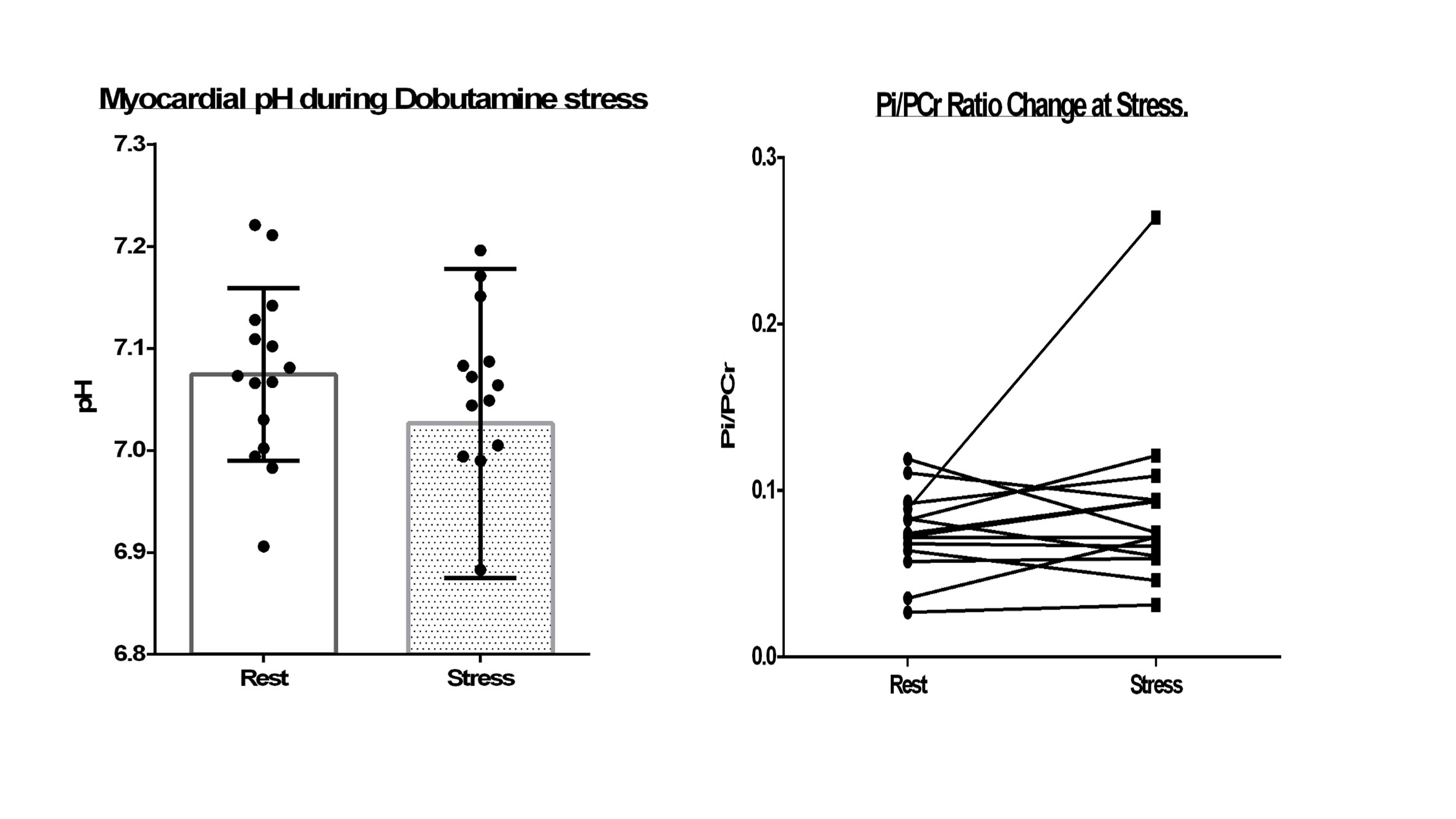
For Pi/PCr calculations, signal-to-noise was acceptable both at rest (Pi 5±4; PCr 74±45) and stress (Pi 5±3; PCr 56±38). Dobutamine levels at the target heart rate was tolerated by all subjects without issues over a period of 15 min. Despite a significant increase in myocardial work (rate-pressure product, mmHg × bpm: 7292 at rest vs 15795 stress, p<10-10), there was no change in myocardial Pi/PCr (0.075±0.023 vs. 0.092±0.053 p=0.15), or pH (7.07±0.09 vs. 7.06±0.16 p=0.70) during stress (Figure 3).Discussion and Conclusion
In healthy volunteers using a long-TM 31P STEAM sequence at 7T suppresses blood pool 2,3-DPG enough to enable robust, rapid detection of Pi in the human heart. Importantly, the guidelines in our institution for catecholamine induced stress scanning are in line with international guidelines [4]. This approach is the first method to be quick enough to study myocardial pH and Pi/PCr ratios during dobutamine stress, and we report here these stress values in the human heart for the first time. After changes in heart rate and pressure, the ECG signal was altered to the degree that the trigger algorithm had to be retrained but this was mostly successful, pulse oximeter signal served as backup.
Long-TM 31P-STEAM
is feasible during dobutamine induced stress in volunteers. As expected in
normal volunteers, myocardial Pi/PCr and pH are both well conserved during this
moderate cardiac stress, but are expected to vary in diseased hearts [5]. We anticipate from physiological considerations that Pi/PCr and
cellular pH are likely to be more sensitive energetic markers than PCr/ATP in
disease groups. This is an important progression in non-invasive metabolic
imaging that is now ready for clinical studies.
Acknowledgements
Funded the Austrian Science Fund (Schroedinger fellowship to AIS J 4043), by a Sir Henry Dale Fellowship from the Wellcome Trust and the Royal Society to CTR [098436/Z/12/B] and the Oxford NIHR Biomedical Research Centre. The Slovak Grant Agencies VEGA [2/0001/17] and APVV [15-0029] are also acknowledged. MAP was supported by a British Heart Foundation Clinical Research Training Fellowship (FS/15/80/31803). AA was funded by BHF under code HSR00620.References
1. Stoll et al, Radiology, 2016; https://pubs.rsna.org/doi/10.1148/radiol.2016152629
2. Rodgers CT et al. Proceedings of the 22nd ISMRM 2014; #2896.
3. Purvis LAB et al. PLoS One 2017 https://doi.org/10.1371/journal.pone.0185356
4. Sicari R, Cortigiani L, Cardiovasc. Ultrasound 2017; https://doi.org/10.1186/s12947-017-0099-2
5. Dass et al. European Heart Journal 2015 https://doi.org/10.1093/eurheartj/ehv120
Figures