2471
Accurate Prenatal Diagnosis of Cleft Palate Using Magnetic Resonance Imaging with 3D Super-resolution Reconstruction1Department of Biomedical Engineering, Guangzhou Medical University, Guangzhou, China, 2Qingyuan People’s Hospital, Qingyuan, China, 3The Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, China, 4Philips Healthcare, Guangzhou, China
Synopsis
The routine clinical technique for prenatal diagnosis of cleft palate (CP) is ultrasound (US). However, the technique has difficulties on definitive diagnosis of fetal CP especially cleft posterior palate because of its technical limitations. Previous studies have demonstrated that magnetic resonance (MR) imaging can be a useful adjunct to the diagnosis of fetal CP and provides better diagnosis performance than US. However, these studies are mainly based on 2D MR imaging which has limited resolution along slice selective direction and cannot freely visualize the fetal palate from any orientation. To address this issue, we sought to use a 3D super-resolution reconstruction method to reconstruct 3D isotropic volumetric images from 2D images stacks and evaluate its feasibility of CP diagnosis.
Introduction:
Cleft palate (CP) is one of the most common human birth defects, which occurs in isolation or as part of a broad range of chromosomal, mendelian or teratogenic syndromes1. The routine clinical technique for prenatal diagnosis of CP is ultrasound (US) . However, the technique has difficulties in definitive diagnosis of fetal CP especially cleft posterior palate because of its technical limitations, such as difficulty in penetrating bone and operator dependent. Previous studies have demonstrated that magnetic resonance (MR) imaging can be a useful adjunct to the diagnosis of fetal CP and provides better diagnosis performance than US2,3. However, these studies are mainly based on 2D MR imaging which has limited resolution along slice selective direction and cannot freely visualize the fetal palate from any orientation4. As fetal CP are small to be clearly visualized on a 2D MR image, we hypothesized that 3D isotropic high resolution MR images can help to improve definitive diagnosis of fetal CP. In this study, we sought to use a 3D super-resolution reconstruction method to reconstruct 3D isotropic volumetric images from 2D image stacks and evaluate its feasibility in CP diagnosis.Methods:
MR Experiment: The IRB approved study consecutively enrolled 10 pregnant patients (gestation 24±2weeks) who have been confirmed by US that their fetuses have malformations including CP. The study was performed on a 3.0T scanner (Achieva, Philips) equipped with a 16 channel phased array body coil by a single shot fast spin echo (SSFSE) sequence. The sequence parameters included: TR/TE= 4273/102ms, FOV =350mm×350mm, spatial resolution = 1.2mm×1.2mm and reconstructed to 0.68mm×0.68mm, slice thickness = 3.0mm. Data from standard transverse, coronal, sagittal and two oblique planes of the fetus was acquired for diagnosis and 3D super-resolution reconstruction.
3D super-resolution reconstruction: All acquired 2D images were loaded to a workstation (Z840, Hewlett-Packard Development Company) for 3D super-resolution volumetric reconstruction based on a SVR algorithm5,6. The spatial resolution of the reconstructed 3D volume was set to 0.75mm×0.75mm×0.75mm. The reconstruction steps were briefly described as follows. First, active contour (also called snakes) was used to segment all the slices automatically. Then motion estimation was made to select the registration template and reject stacks with too much motion. After this, 3D volumetric registration was performed between all stacks and the template stack to account for global transformations. Finally, iterations were executed to reconstruct the high resolution 3D images using SVR algorithm. To speed up the process, we implemented the proposed algorithm using GPUs and Nvidia’s compute unified device architecture (CUDA). The reconstruction processing time was less than 3 minutes.
Image Analysis:
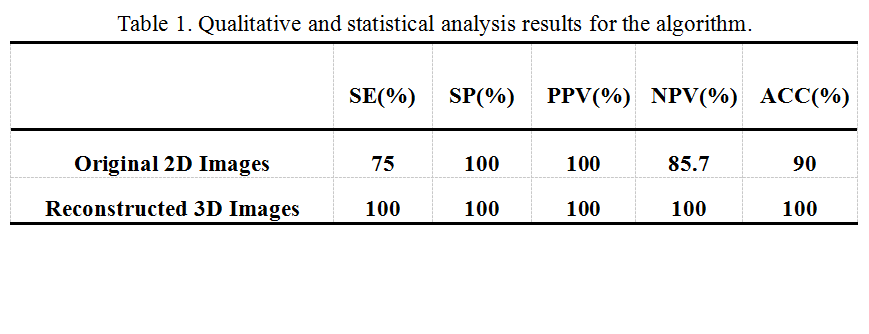
All MR images, including the original 2D and the reconstructed 3D images, were loaded on a workstation (Intellispace Portal) for image analysis and review. Two radiologists blinded to all subjects’ information and imaging protocols independently assessed the randomized images and made a diagnosis of fetal CP (presence or absence). The image quality and diagnosis confident scores were also assessed by the two radiologists based on a four points scale: (1 = poor, 2 = fair, 3 = good, and 4 = excellent). The sensitivity (SE), specificity (SP), positive and negative predictive values (PPV and NPV), and the accuracy (ACC) were calculated with reference to the findings at birth.Results:
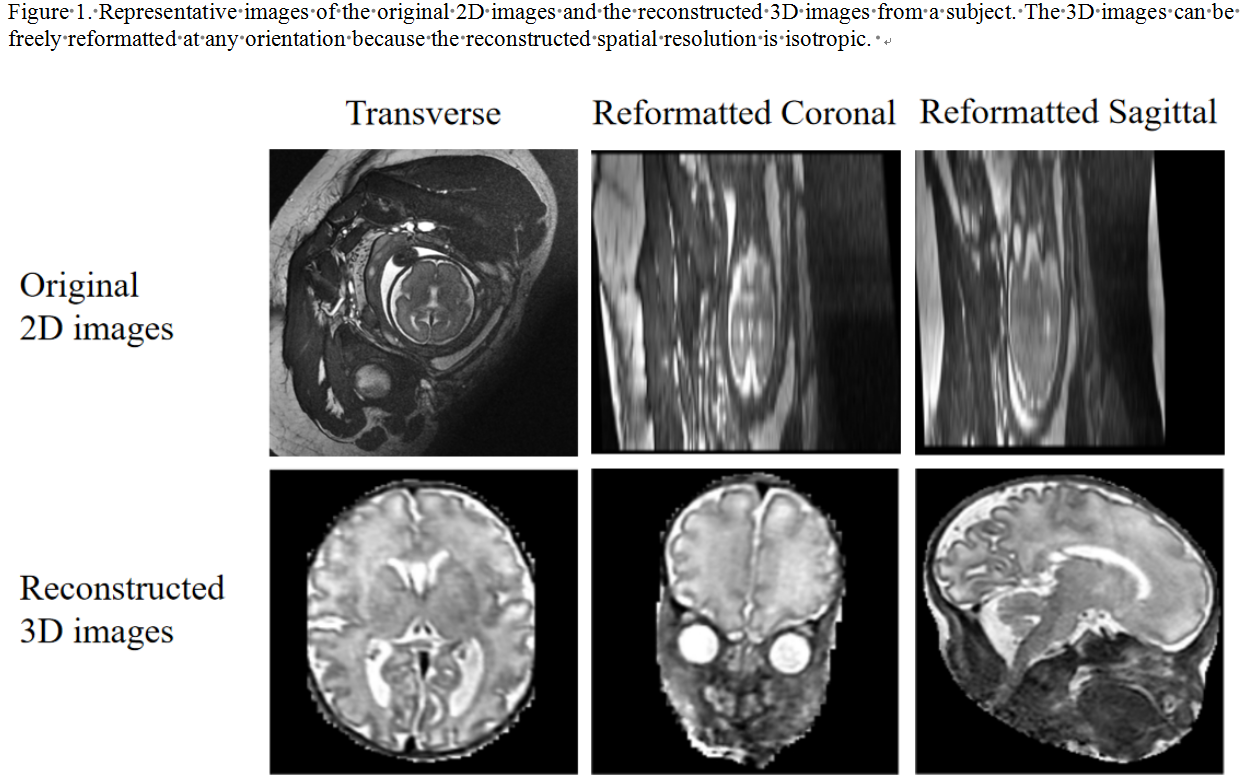
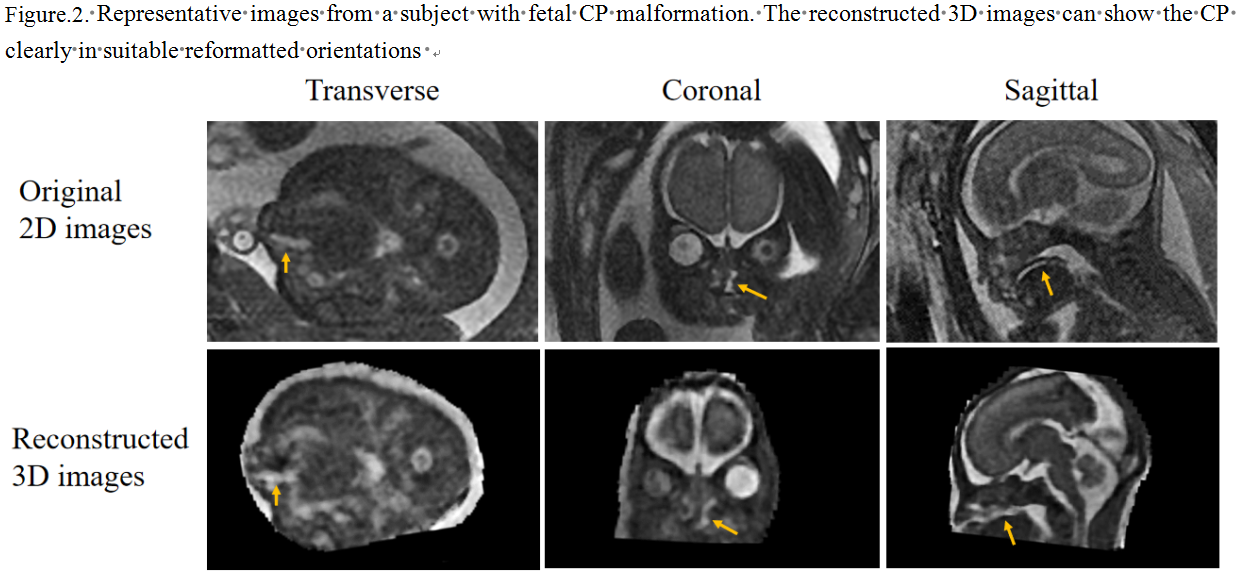
The isotropic high resolution 3D images were successfully reconstructed from the original 2D images for all subjects. Compared to the original 2D images, the reconstructed 3D images can be freely reformatted for any orientations (Figure 1) and had better image quality and diagnosis confident scores (i.e., 3.4 ± 0.7 vs. 3.0 ± 0.8, p = 0.046, and 3.8 ± 0.4 vs. 3.1 ± 0.9, p = 0.038, respectively). The CP malformation was visualized clearer on the reconstructed 3D images than on the original 2D ones (Figure 2). According to the findings at birth, four participants were diagnosed CP. Using the findings as standard reference, the participants with CP were all correctly identified based on the reconstructed 3D images. The SE, SP, PPV, NPV and ACC of diagnosing CP based on the original 2D and the reconstructed 3D images were shown in Table 1.Conclusion:
The reconstructed 3D images with high and isotropic spatial resolution can be freely reformatted and viewed from any orientations, allowing to clearly visualize the fetal palate and thus to improve the accuracy and efficiency of the prenatal diagnosis of CP.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 81741010,No. 81571669)References
1. A. OginoEmail, K. Onish, Y. Maruyama. Congenital oral synechia associated with cleft palate: Cleft palate medial synechia syndrome? European Journal of Plastic Surgery. 2015;27(7):338-340.
2. B. Ertl-Wagner, A. Lienemann, A. Strauss, and M.F. Reiser. Fetal magnetic resonance imaging: Indications, technique, anatomical considerations and a review of fetal abnormalities. Eur Radiol. 2002;12(8):1931-1940.
3. D. Prayer, P. Brugger, and L. Prayer. Fetal MRI:Techniques and protocols. Pediatric Radiol. 2004;34(9):685-693.
4. B. Kainz et al. Fast volume reconstruction from motion corrupted stacks of 2D slices. IEEE Trans. Med Imag. 2015;34(9):1901-1913.
5. B. Fei, J. L. Duerk, D. T. Boll, J. S. Lewin, and D. L. Wilson. Sliceto-volume registration and its potential application to interventional MRI-guided radio-frequency thermal ablation of prostate cancer. IEEE Trans. Med. Imag. 2003;22(4):515-525.
6. A. Gholipour, J. A. Estroff, and S. K. Warfield. Robust super-resolution volume reconstruction from slice acquisitions: Application to fetal brain MRI. IEEE Trans. Med Imag. 2010;29(10):1739-1758
Figures