2463
A brain extraction algorithm for infant T2-weighted images based on the fuzzy c-means thresholding1Department of Health Sciences and Technology, GAIHST, Gachon University, Incheon, Korea, Republic of, 2College of Health Science, Gachon University, Incheon, Korea, Republic of
Synopsis
Brain extraction is an important step in image processing for research and diagnostic assessments using brain MR images. In this work, we proposed a brain extraction algorithm optimized for both 2D and 3D infant T2-weighted images based on the fuzzy c-means thresholding and spatial information of the neighboring slices. Quantitative analysis using the dice ratio was performed to compare the results of brain extraction using the proposed method, BET, iBEAT, and
Introduction
Brain extraction is an important step in brain MR image analysis because it influences the accuracy of structural information. For adult brains, T1-weighted (T1W) images are conventionally used for brain extraction because they have better image contrast than T2-weighted (T2W) images. Consequently, the conventional brain extraction algorithms are mostly optimized for T1W images, making it difficult to obtain accurate infant brains from T2W images. As brain extraction from T2W infant brain images is also required in certain clinical applications, an optimized brain extraction algorithm for T2W infant brain images is presented in this abstract.Methods
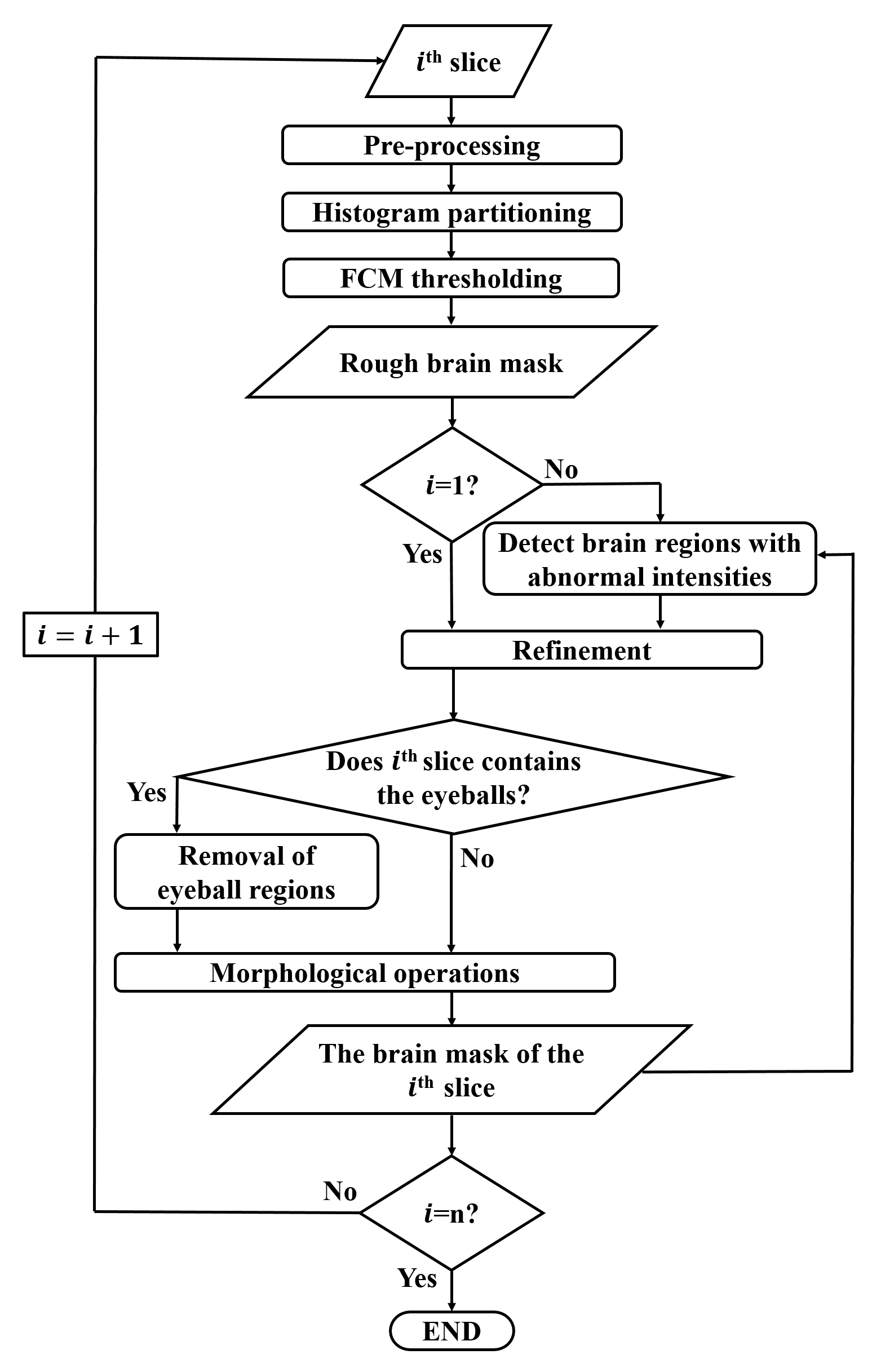
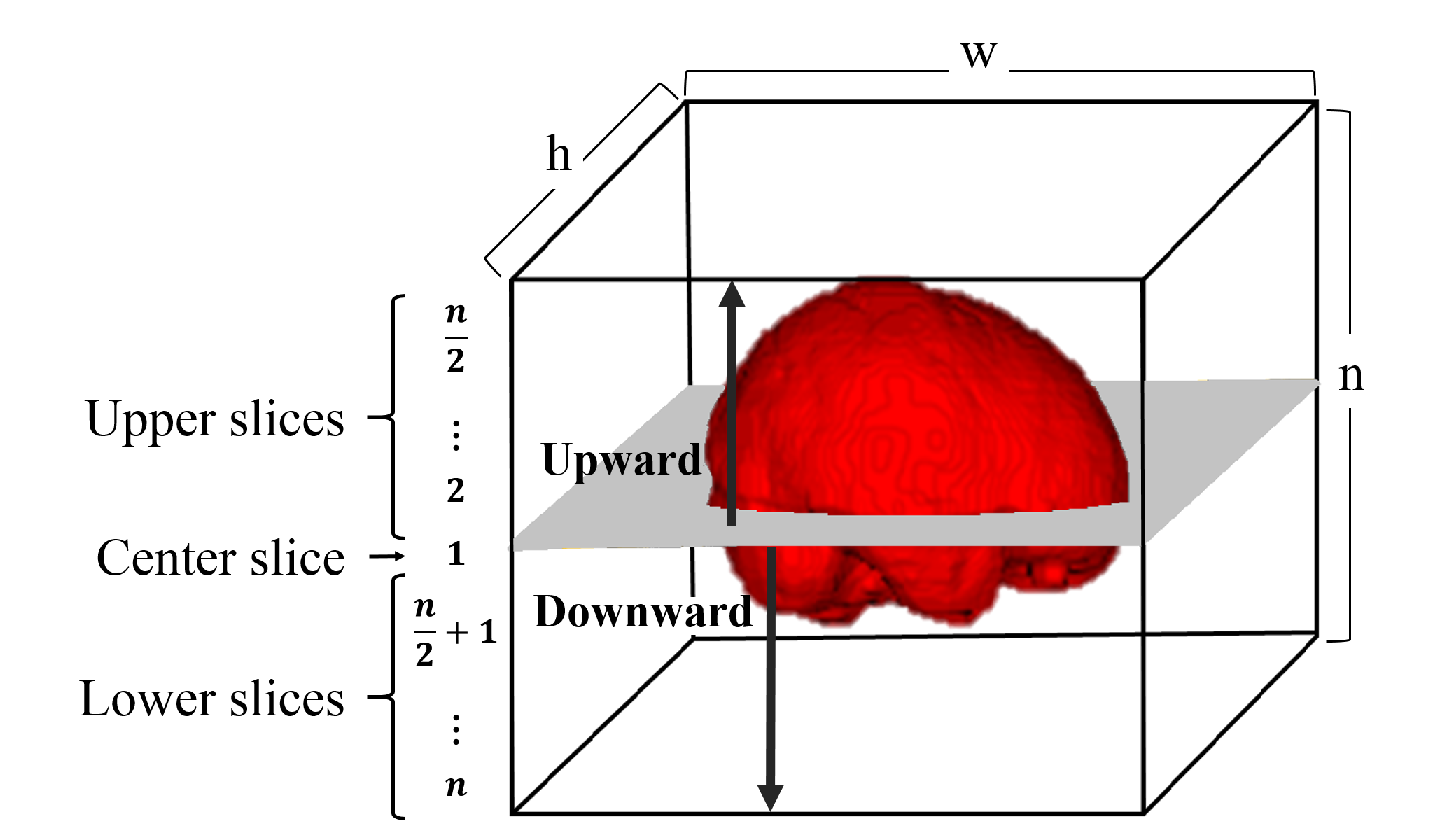
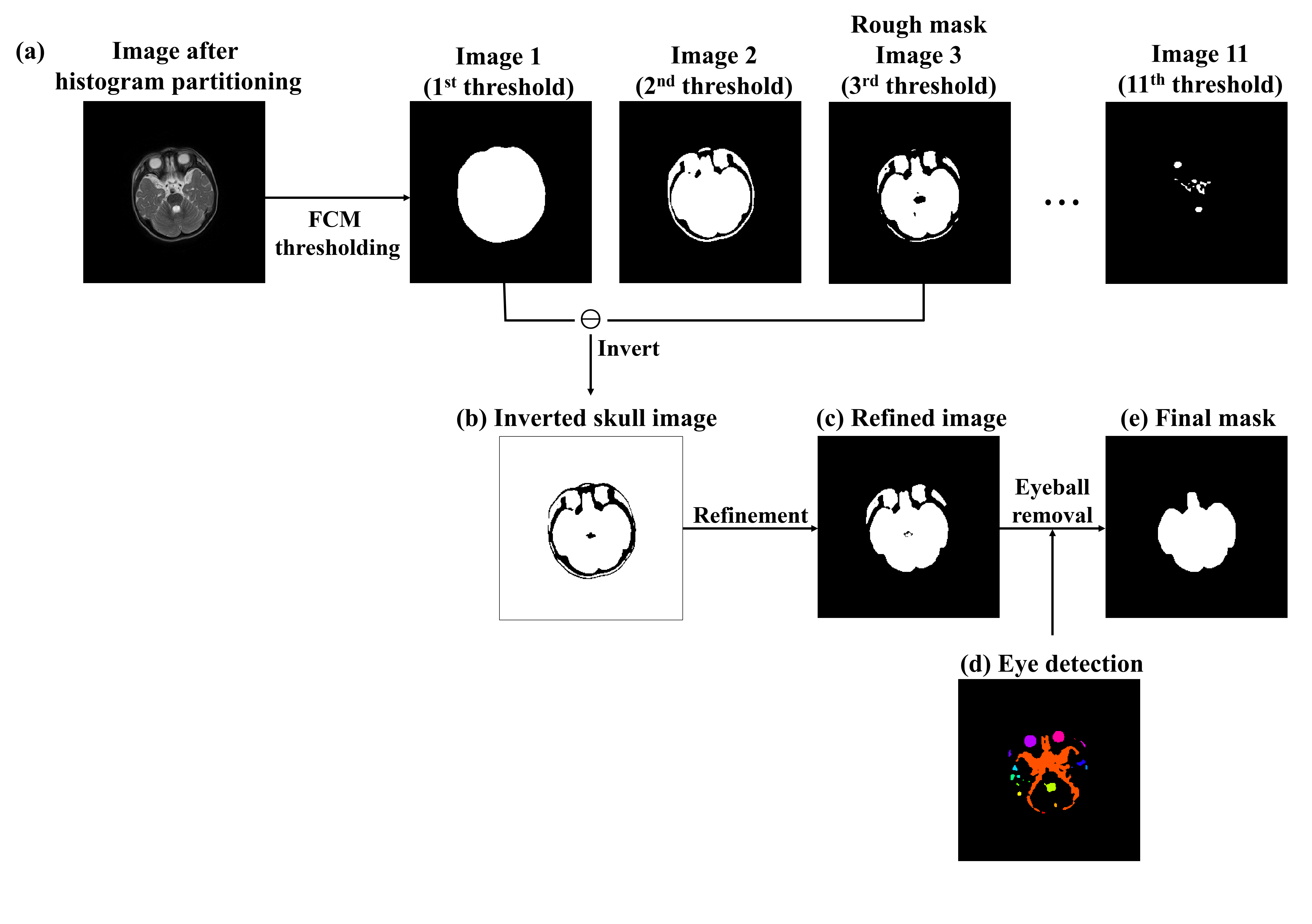
The overall procedure of the proposed method is illustrated in Fig.1. Initially, preprocessing is performed to remove the background noise and to compensate for image inhomogeneity. Then, the center slice located in the middle of the brain volume (Fig.2) is selected to generate an initial mask as follows. First, the image is separated into two regions, i.e., background and brain regions, by using the histogram partitioning1. By applying the 12-class fuzzy c-means (FCM) thresholding2 to the separated brain regions and taking the 3rd threshold image, the rough brain mask of the center slice is generated. Then, refinement is performed to produce the initial mask. The center slice is selected for the initial mask because it usually contains the largest cross-section of the brain. After generating the initial brain mask, brain extraction is performed for the next slice from center to upward, followed by center to downward directions (Fig.2). For the (i+1)th slice, a rough brain mask is generated as explained above. As some regions with abnormal intensities can be falsely included or excluded during the FCM thresholding, the previous (ith) brain mask is used to estimate the shape of the current brain slice and to compensate for the errors. However, the previous brain mask may not be suitable for certain image sets having abrupt shape changes between slices (e.g. due to slice gaps), Thus, an inverted skull mask is additionally utilized as a complementary measures. Finally, to include the brain regions that are not connected to the largest component of the brain, the overlap-test3 between the current ((i+1)th) and the previous (ith) brain masks is performed. In addition, the eyeball regions are excluded from the mask by considering the location and size of eyeballs4 (Fig.3). After removing the eyeball regions, region filling is conducted to refine the brain mask.Results
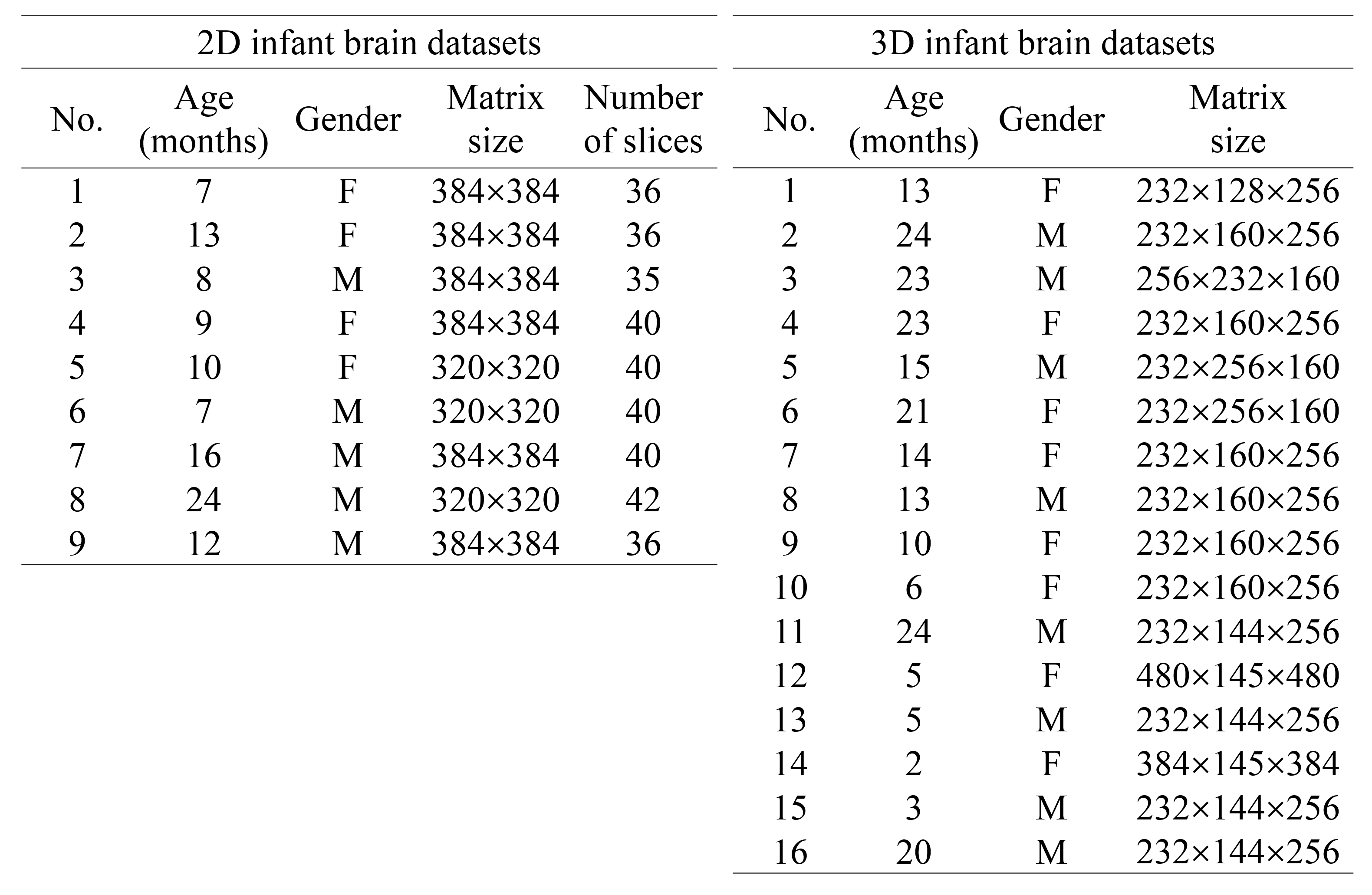
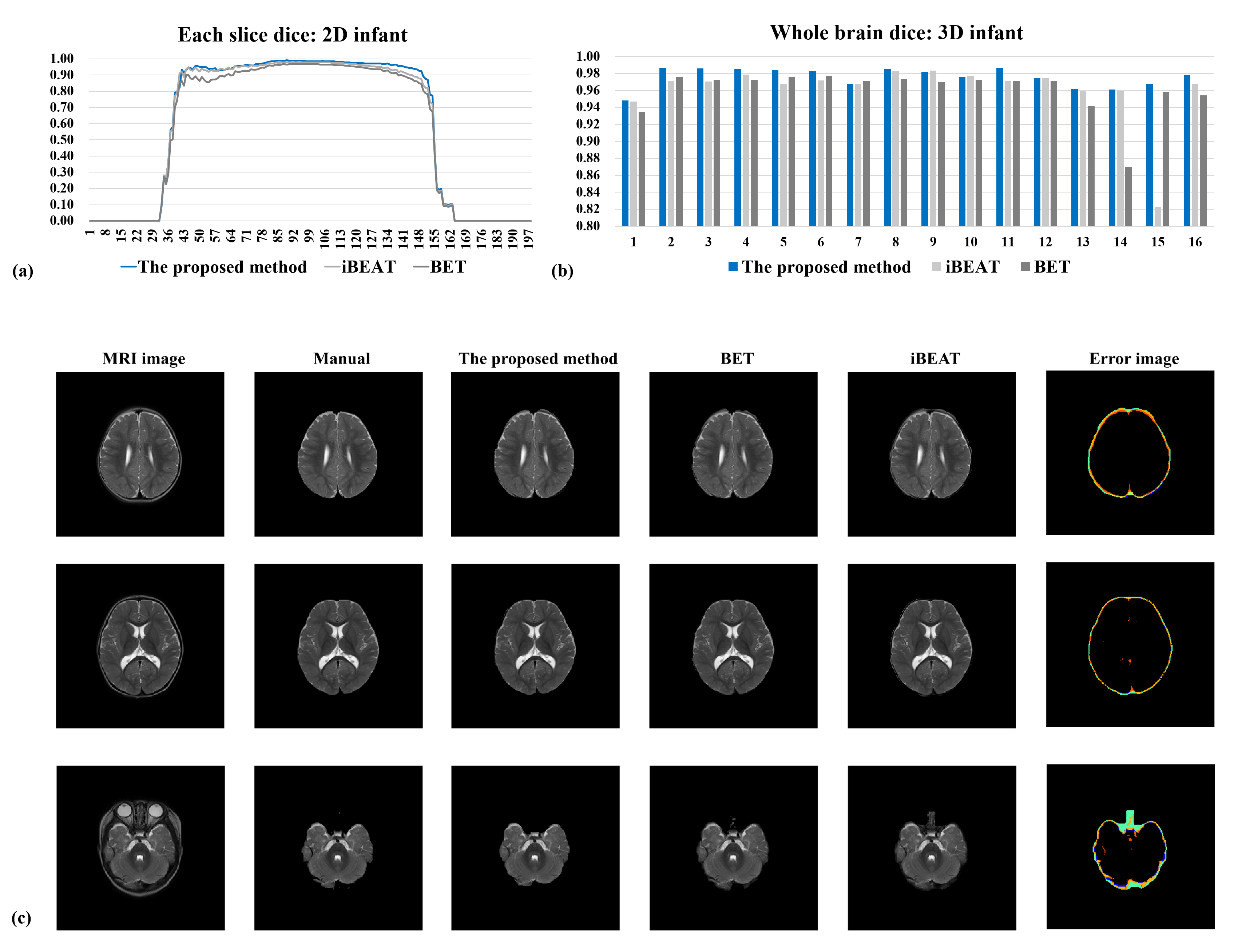
We used 2D and 3D infant T2W images acquired at 3T MRI of different vendors (Philips,Siemens) (Table.1). The images were interpolated and registered to RAS coordinates to have voxel sizes of 1×1×1 mm3 and matrix sizes of 256×256×198. 3D datasets contained images with no structural abnormalities and 2D datasets contained images from normal infants and infants with pathological characteristics, including hypo- and hyper-intensities. To quantitatively compare the proposed method, iBEAT5, BET6 and manual segmentation, dice ratio was calculated after brain extraction. For demonstration purposes, inter-subject average of each slice was calculated for 2D datasets, where the proposed method showed the highest dice ratio (0.8742±0.23), followed by iBEAT (0.8609±0.23) and BET (0.8352±0.23) (Fig.4a). In 3D datasets, dice coefficients of the whole brain volume was calculated to remove the bias due to registration errors and the proposed method also provided better performance in general (Fig.4b). The average dice ratio was 0.9759±0.01 for the proposed method, 0.9608±0.03 for iBEAT, and 0.9603±0.02 for BET, demonstrating that the proposed method generated more accurate brain masks with less performance deviations across datasets. Although iBEAT generated slightly higher dice coefficients in datasets 9 and 10, it showed a large deviation of performance and significant failures in some dataset (data15). In Fig.4c, error images of three different methods and the manual segmentation were also illustrated with different colors, where the proposed method showed the least amount of errors in all slices.Discussion & conclusion
The proposed method significantly improved the accuracy of brain extraction in infant T2W images, both in 2D and 3D MR images, by using the FCM thresholding with the spatial information of the brain region in the previous slice and the inverted skull mask. While the characteristics of training and test sets may influence the performance of machine-learning based algorithms (as used in iBEAT), the proposed method can be more generally used because it utilizes the characteristics of the target images themselves. The quantitative analysis showed that the proposed method could be efficiently used to extract brain region from infant brain MR images.Acknowledgements
No acknowledgement found.References
1. A.G. Balan, A.J. Traina, M.X. Ribeiro, et al. Smart histogram analysis applied to the skull-stripping problem in T1-weighted MRI. Comput Biol Med. 2012;42(5):509-22.
2. S. Sumathi, S. Paneerselvam. Computational Intelligence Paradigms: Theory & Applications using MATLAB. 2010
3. K. Somasundaram, T. Kalaiselvi. Fully automatic brain extraction algorithm for axial T2-weighted magnetic resonance images. Comput. Biol. Med. 2010;40(10):811-22
4. R.N. Hussain, F. Shahid, G. Woodruff. Axial length in apparently normal pediatric eyes. Eur J Ophthalmol. 2014;24(1):120-3
5. Y. Dai, F. Shi, L. Wang, et al. iBEAT: A toolbox for infant brain magnetic resonance image processing. Neuroinformatics. 2013;11(2):211-25.
6. S.M. Smith. Fast Robust Automated Brain Extraction. Hum. Brain Mapp. 2002;17(3):143-55.
Figures