2420
Dual-venc phase contrast MRI with increased flow encoding efficiency1Radiology, Northwestern University, Chicago, IL, United States
Synopsis
To decrease scan time while maintaining SNR and velocity dynamic range of dual-venc 2D phase-contrast MRI with 3-directional velocity encoding, the sequence was modified to zero-fill the extremes of k-space in the high-venc (HV) acquisition while collecting fully sampled low-venc (LV). In vitro sensitivity analysis shows antialiasing success over 95% with up to 50% zero-filled HV scans. Preliminary data from a healthy control aorta indicate that antialiasing success approaching 100% can be maintained using HV scans. This promising approach may be extended to further improve flow encoding efficiency in volumetric scans.
Introduction
Dual velocity encoding (dual-venc) phase contrast (PC) MRI enables accurate assessment of both fast (e.g. arterial) and slow (e.g. venous) blood flow by ensuring high signal-to-noise ratio over a wide range of velocities1, 2. However, dual-venc doubles the scan time when using an 8-TR implementation. In this work, a dual-venc approach with low-resolution high-venc acquisition, accomplished via zero-filling, is presented. A sensitivity analysis is conducted using a rotating phantom to determine the highest zero-filling percentage that will allow for identification of at least 95% of aliased voxels compared to full-resolution scans.Methods
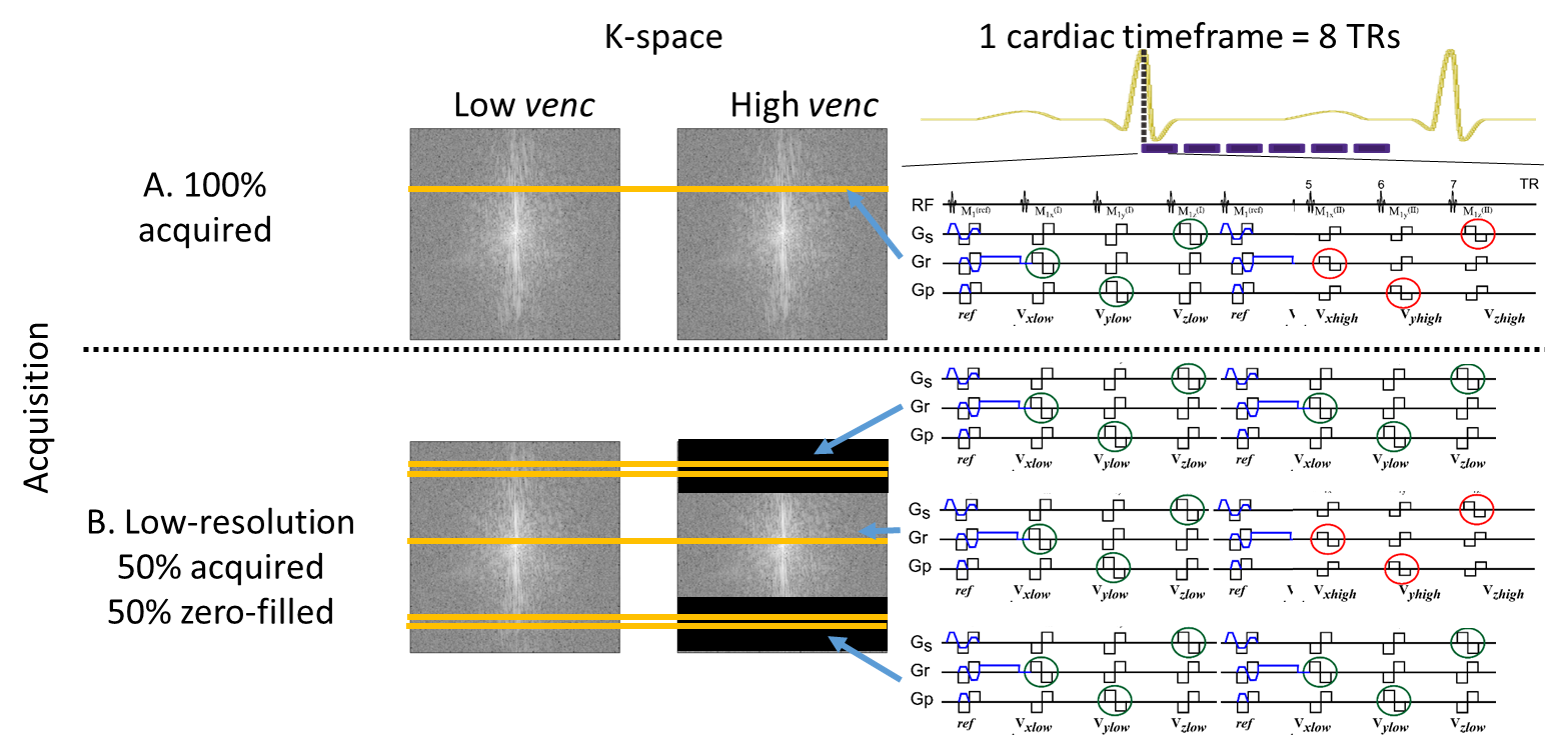
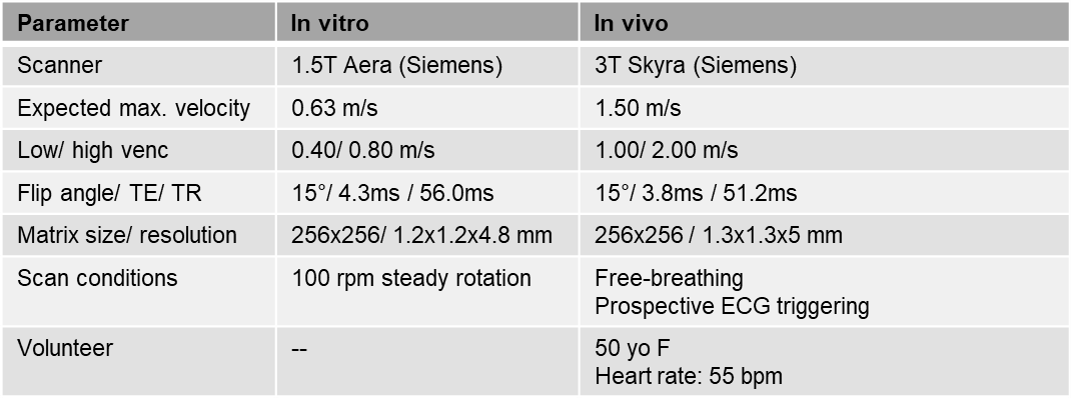
Sequence development: A fully integrated Cartesian ECG-gated dual-venc PC sequence using 8-point encoding was modified to accept a user-defined percentage of phase encoding lines at the extremes of k-space in the high-venc (HV) acquisition to be zero-filled, while collecting fully resolved low-venc (LV) data. LV and HV k-space data were acquired sequentially within 8 TRs (each having their own reference scan) generating automatically coregistered images (Fig.1). Scan parameters were as in Fig.2, with no parallel imaging acceleration and 100% phase sampling. Reconstruction was done in Matlab (Mathworks, USA) using the Walsh method3.
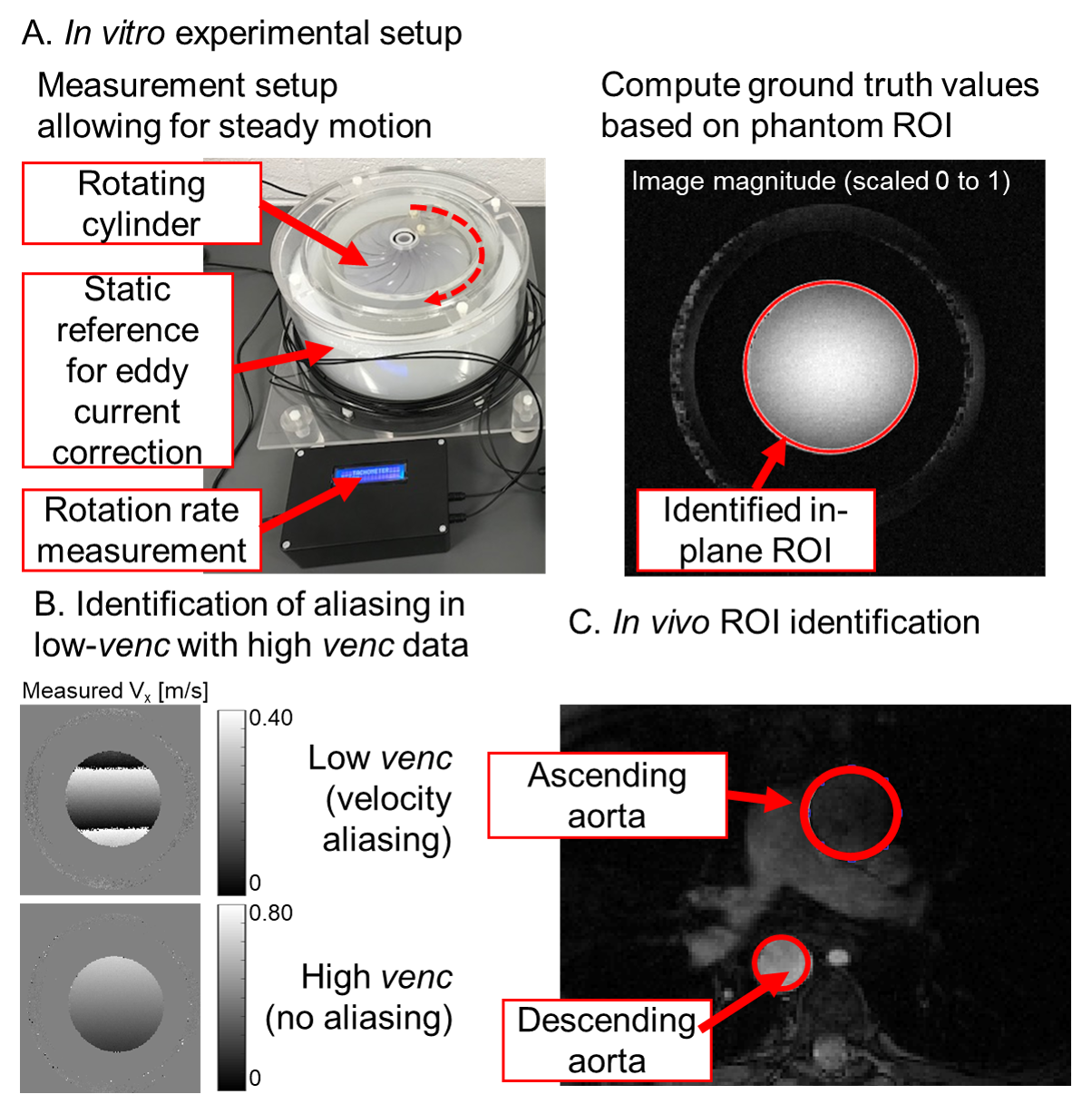
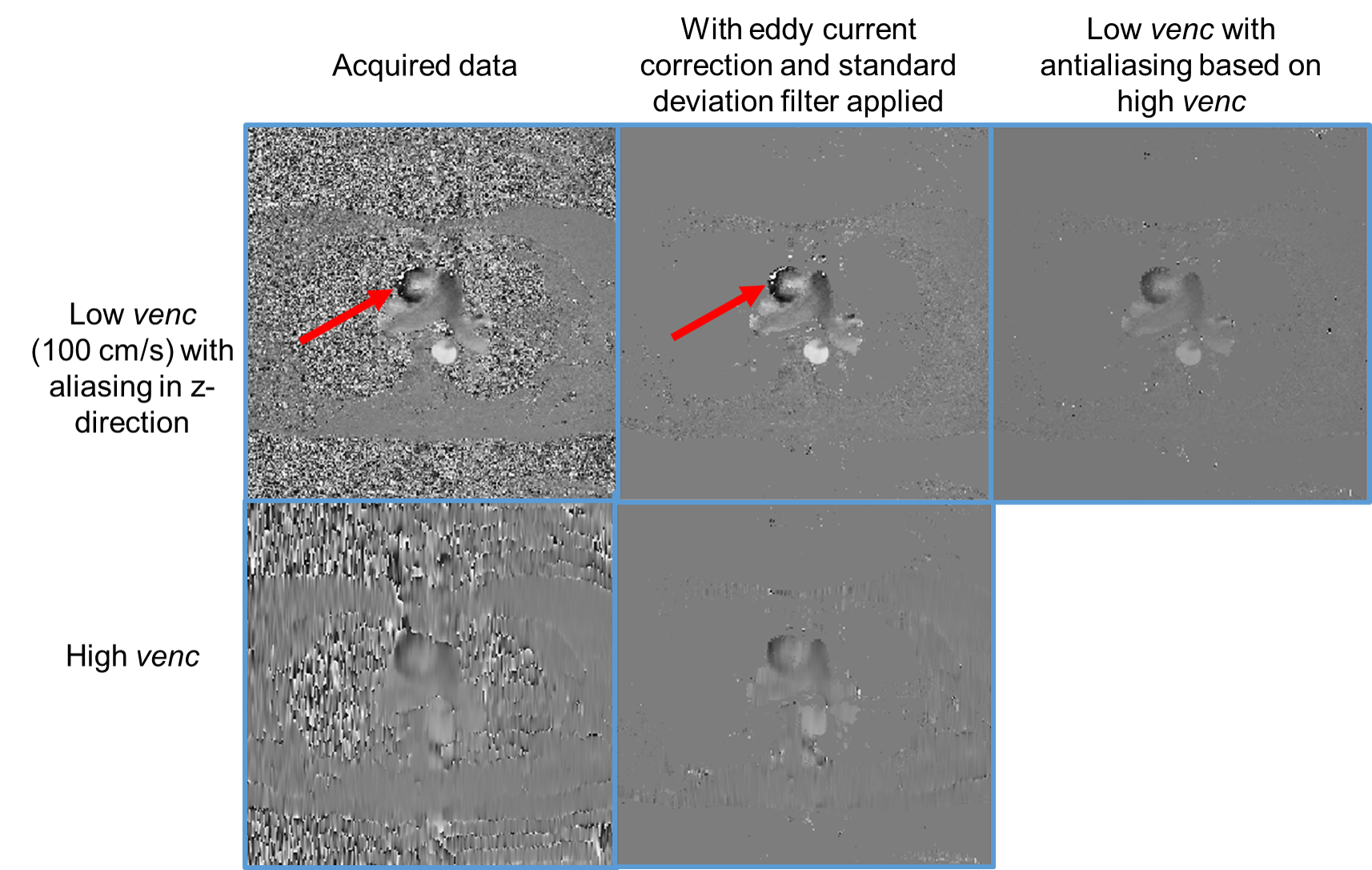
In vitro scans: A dedicated MR-compatible cylindrical phantom with constant rotational speed of approximately 100 rpm around its axis provided a known distribution of velocities (Fig.3A). A single imaging slice was acquired perpendicular to the axis of rotation, so that velocity in both in-plane directions was expected to vary linearly in space with minimal through-plane motion. The LV and HV were chosen, so that only the LV would be aliased and the HV can be used for antialiasing (Fig.3B). Two approaches were tested: 1. Six data sets with 50, 60, 70, 80, 90 and 100% of LV resolution were acquired at scanner (measured data) and 2. retrospective zero-filling of the fully resolved data set by replacing corresponding k-space lines with zeros (simulated).
In vivo scan: ECG-gated dual-venc 2D PC MR imaging plane with 3-directional velocity encoding was positioned across the ascending and descending aorta of a consented healthy volunteer (Fig.3C). Only a fully resolved data set without zero-filling was acquired in vivo. Zero-filling was achieved by retrospectively removing and zero-filling k-space lines as above. Spatial resolutions of 10, 20, 30, 40, 50, 60, 70, 80, 90 and 100% for the HV compared to LV were tested.
Post-Processing: In-house developed tools were used to correct for noise (standard deviation filter) and phase offset, and to identify ROIs. In vitro ground truth values were calculated based on phantom geometry and rotational speed. Aliasing identification was assessed by comparing voxels where velocity aliasing was identified in measured data sets, relative to ground truth calculations (in vitro) or 100% resolution data (in vivo).
Results
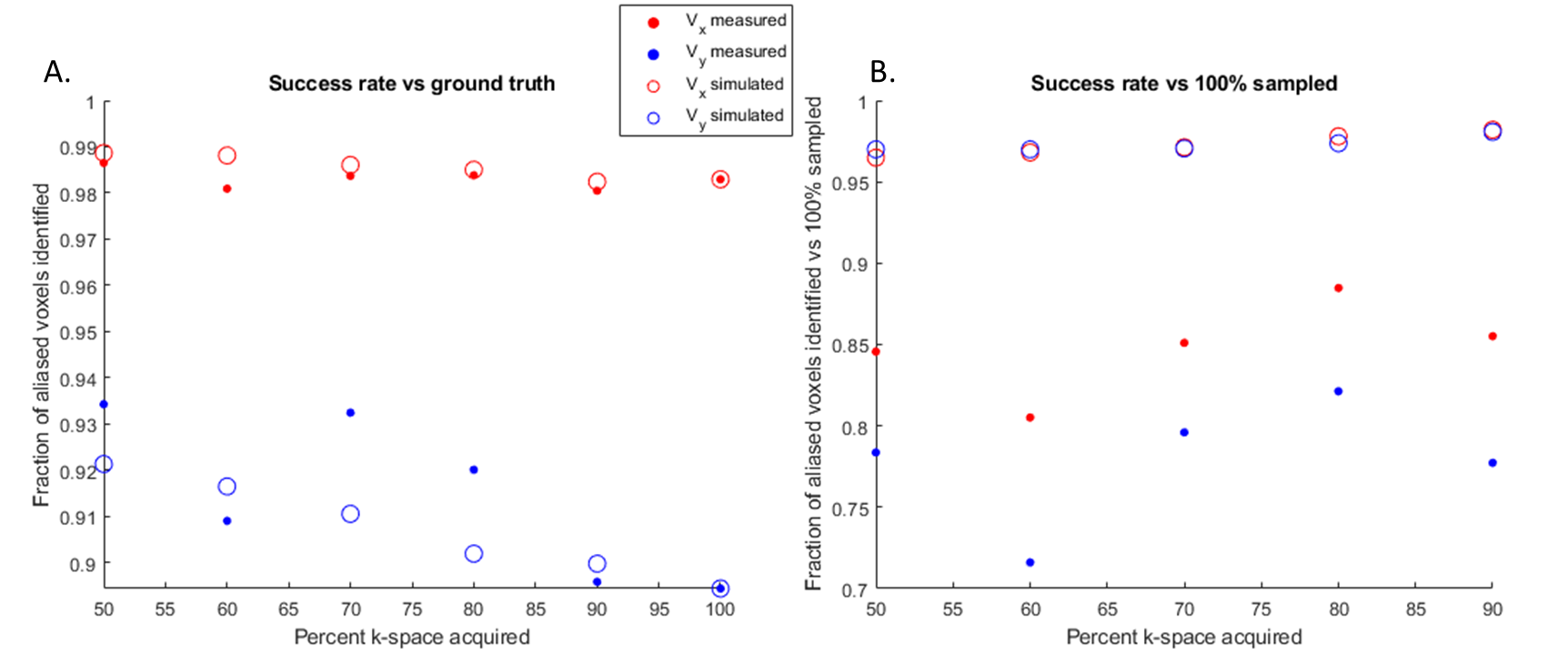
Acquisition time for lower resolution scans was decreased up to 25% in the case of 50% high-venc zero-filling. Phantom rotational speed was measured at 99±7 rpm. The dual-venc data allowed for over 97% success in aliasing correction relative to ground truth for all zero-filling schemes tested in the x-direction (Fig.4A). Misidentification of the phantom ROI in the y-direction was observed due to distortion (resulting in an ellipsoid instead of sphere) with corresponding lower performance. Relative to 100% sampled data, measured data acquired with 50-90% of zero-filling have 70-88% aliasing identification along y-direction (Fig.4B). However, retrospectively simulated zero-filled data (which does not contain scan-to-scan variability in velocity) has over 95% aliasing identification accuracy even with 50% zero filling.
In vivo, at all resolution values tested, all 23 aliased voxels identified were correctly identified (Fig.5). Thus, final velocity measurements were identical among all resolutions tested.
Discussion and conclusion
Low-resolutionHV acquisitions within the dual-venc paradigm allows up to 25% reduction in acquisition time while identifying at least 95% of aliased voxels compared to non-zero-filled HV using simulated data (same scan). In vivo data shows 100% aliasing identification even at 10-fold-reduced HV spatial resolution, though this result is unlikely to generalize to smaller flow regions and requires further investigation.
This study was limited by the quality of ROI identification in the phantom, which is likely to have caused the apparent systematic differences between computed and measured values, and the lack of correction for Maxwell terms. Finally, in vivo results are limited by small aliasing areas and use of a single subject. However, this method may allow for substantial time savings while retaining the benefits of dual-venc acquisition for clinical applications and could be extended to dual-venc 4D Flow MRI. Future work will include further in vivo evaluation and integration with advanced acceleration methods to image 3D volumes.
Acknowledgements
F30 HL140910
R01 HL117888
16SDG 30420005
References
1. Turski P, Scarano A, Hartman E, Clark Z, Schubert T, Rivera L, et al. Neurovascular 4dflow mri (phase contrast mra): Emerging clinical applications. Neurovascular Imaging. 2016;2.
2. Schnell S., C. Wu, J. Garcia, I.G Murphy, O.A. Rahman, A.A. Rahsepar, M. Aristova, J. D Collins, J.C Carr, M. Markl. Accelerated dual-venc 4d flow mri for neurovascular applications. J Magn Reson Imaging. 2017 46:102-114.
3. Walsh, D. O., Gmitro A.F., Marcellin, M. W. Adaptive reconstruction of phased array MR imagery. Magn Reson, Med. 2000;43: 0740-3194.
Figures